(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st was host to the session Presidential Symposium 1. Dr. Christof Vulsteke presented the LBA2 - Perioperative (enfortumab vedotin (EV) plus pembrolizumab (pembro) in participants (pts) with muscle-invasive bladder cancer (MIBC) who are cisplatin-ineligible: The phase 3 KEYNOTE-905 study.
Dr. Vulsteke opened by emphasizing that neoadjuvant cisplatin-based chemotherapy (with or without perioperative durvalumab or adjuvant nivolumab for high-risk disease) followed by radical cystectomy (RC) and pelvic lymph node dissection (PLND) remains the standard of care for patients with MIBC.1-3 However, nearly 50% of patients are cisplatin-ineligible per Galsky criteria, typically older, frailer, and with greater comorbidity burden, leaving them without effective neoadjuvant options.4 Limited data in this population show poor outcomes with RC + PLND alone, underscoring a major unmet clinical need, as no prior phase 3 trial has demonstrated perioperative benefit in this subgroup. Based on strong biologic rationale, the phase 3 KEYNOTE-905 trial was designed to evaluate perioperative enfortumab vedotin (EV) + pembrolizumab compared with surgery alone in cisplatin-ineligible or cisplatin-declining patients with MIBC.1
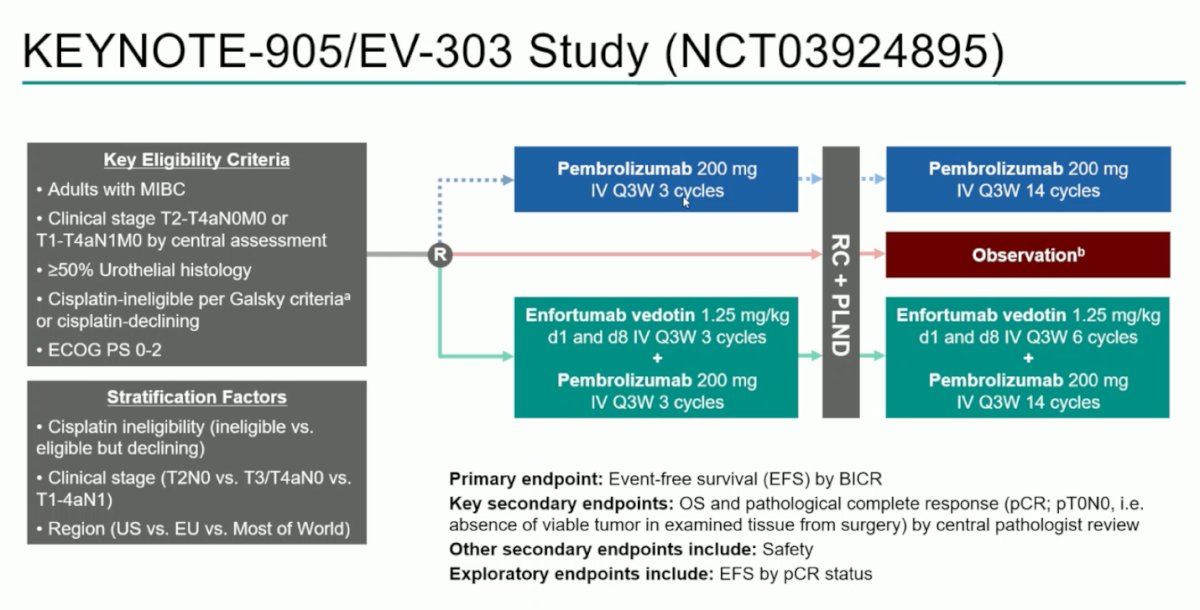
KEYNOTE-905 (EV-303; NCT03924895) enrolled adults with MIBC (≥50% urothelial histology) who were either cisplatin-ineligible per Galsky criteria or declined cisplatin,4 had an ECOG PS 0-2, and clinical stage T2-T4aN0M0 or T1-T4aN1M0 disease. Patients were randomized across three study arms: two experimental perioperative arms, one with pembrolizumab alone and another with enfortumab vedotin plus pembrolizumab and a control arm of RC + PLND followed by observation. Treatment in the experimental arms included three neoadjuvant cycles of pembrolizumab (with or without EV), followed by RC + PLND, and continued with 14 adjuvant cycles of pembrolizumab (plus six cycles of EV in the EV combination arm).
Stratification factors included cisplatin eligibility, clinical stage, and region. The primary endpoint was event-free survival (EFS) by blinded independent central review (BICR), with key secondary endpoints including overall survival (OS) and pathological complete response (pCR), along with safety and exploratory analyses of EFS by pCR status. The study design is shown below.
Dr. Vulsteke presented the first interim analysis of the phase 3 KEYNOTE-905/EV-303 trial (NCT03924895), comparing observation versus perioperative enfortumab vedotin plus pembrolizumab, consisting of neoadjuvant EV + pembrolizumab followed by RC + PLND and adjuvant EV + pembrolizumab as highlighted below.
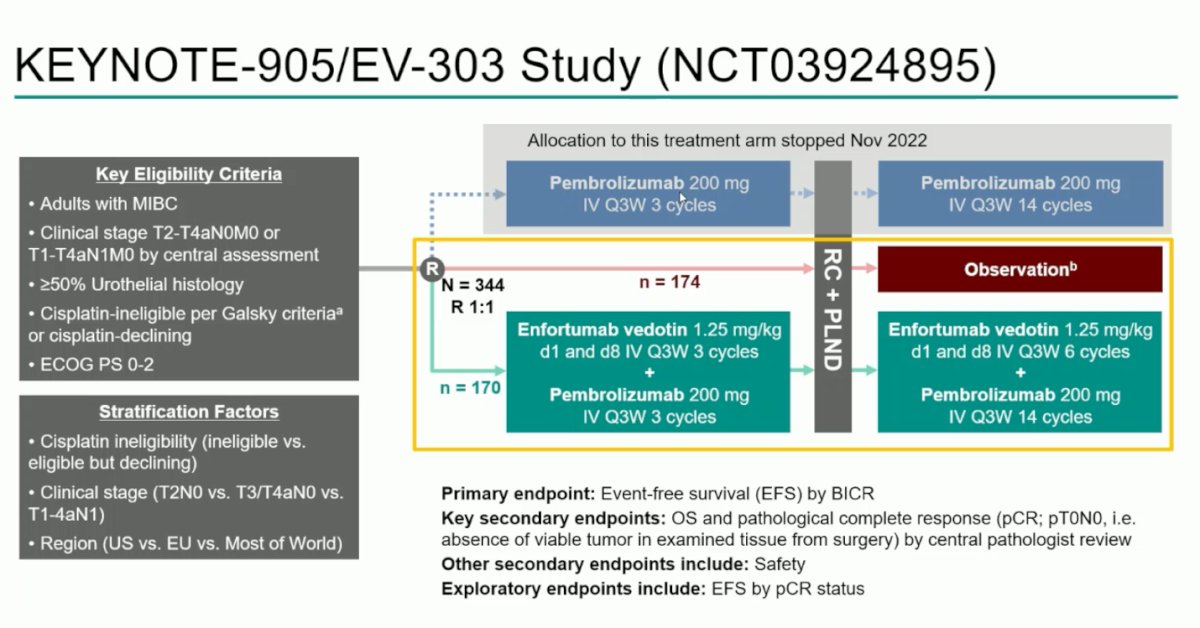
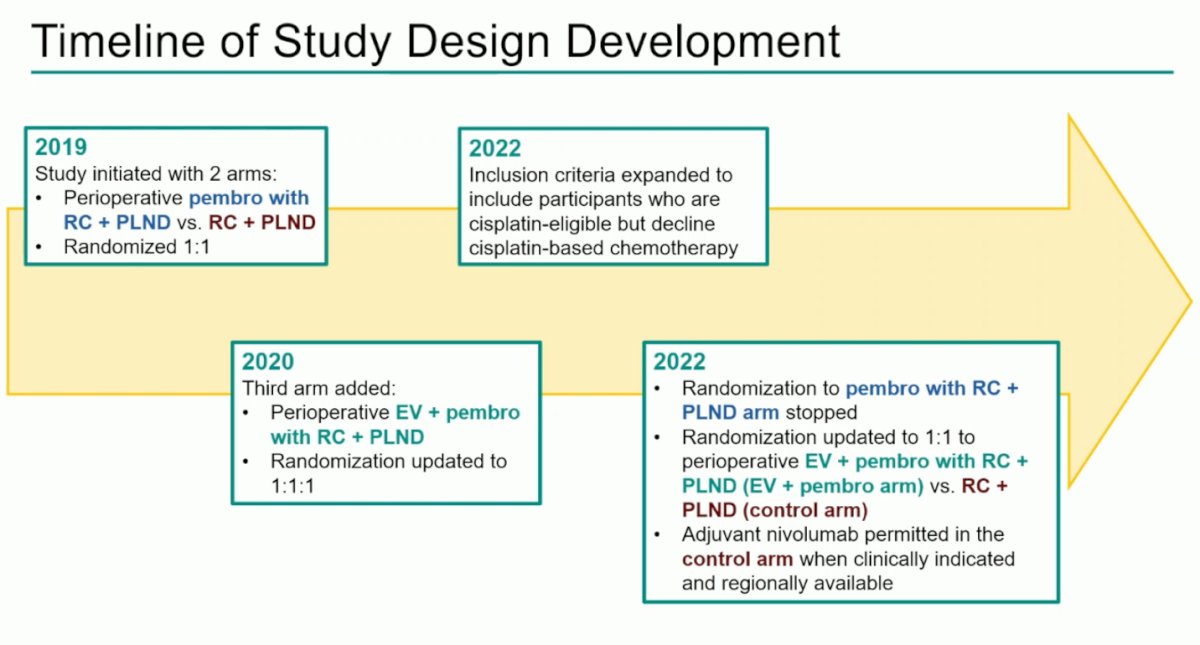
The study was initiated in 2019 with two arms: perioperative pembrolizumab with RC + PLND versus RC + PLND alone. In 2020, a third arm evaluating perioperative enfortumab vedotin plus pembrolizumab was added based on encouraging results in the metastatic setting. (1) Randomization was later amended to 1:1 after discontinuation of the pembrolizumab-only arm in 2022.
The statistical design controlled the familywise type I error at a one-sided α of 2.5% using the Maurer and Bretz graphical method. Initially, the entire α was allocated to EFS for the EV + pembrolizumab versus control comparison (α=0.025), then hierarchically split to test OS and pCR. Efficacy was assessed in all concurrently randomized participants, and TEAEs were evaluated in all patients who received ≥1 dose of study treatment, including during surgery.

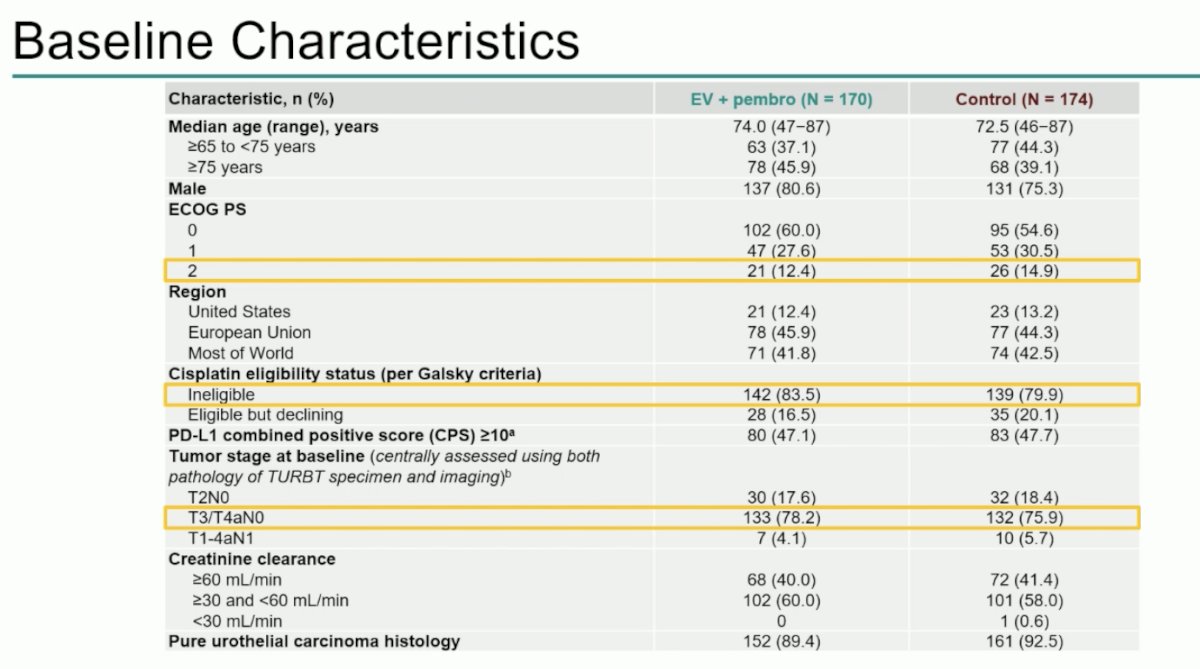
Baseline characteristics were well balanced between arms. The median age was approximately 74 years in the experimental arm and 72.5 in the control arm, older than in prior MIBC trials. Dr. Vulsteke highlighted that 12-15% of patients were ECOG 2. Around 80% were cisplatin-ineligible, most commonly due to renal impairment. Tumor stage was centrally assessed using both TURBT pathology and imaging, with most patients presenting T3/T4aN0 disease. Nearly all (89 -92.5%) had pure urothelial carcinoma histology. Baseline characteristics are outlined below.
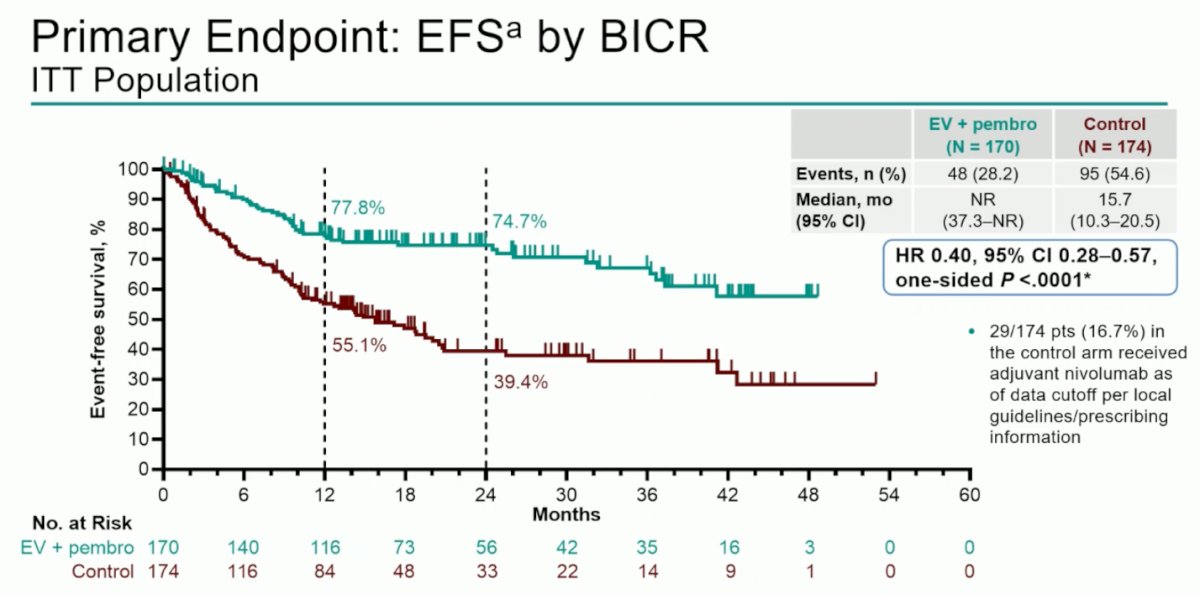
The primary endpoint of EFS by BICR demonstrated a significant improvement with EV + pembrolizumab versus control, with median EFS not reached compared to 15.7 months (HR 0.40, 95% CI 0.28–0.57; one-sided p < 0.0001). The Kaplan-Meier curves showed early and sustained separation, underscoring the poor outcomes typically seen in cisplatin-ineligible patients. As defined, EFS events included progression precluding surgery, residual or recurrent disease, metastasis, or death. Notably, 16.7% of patients in the control arm received adjuvant nivolumab per local guidelines.
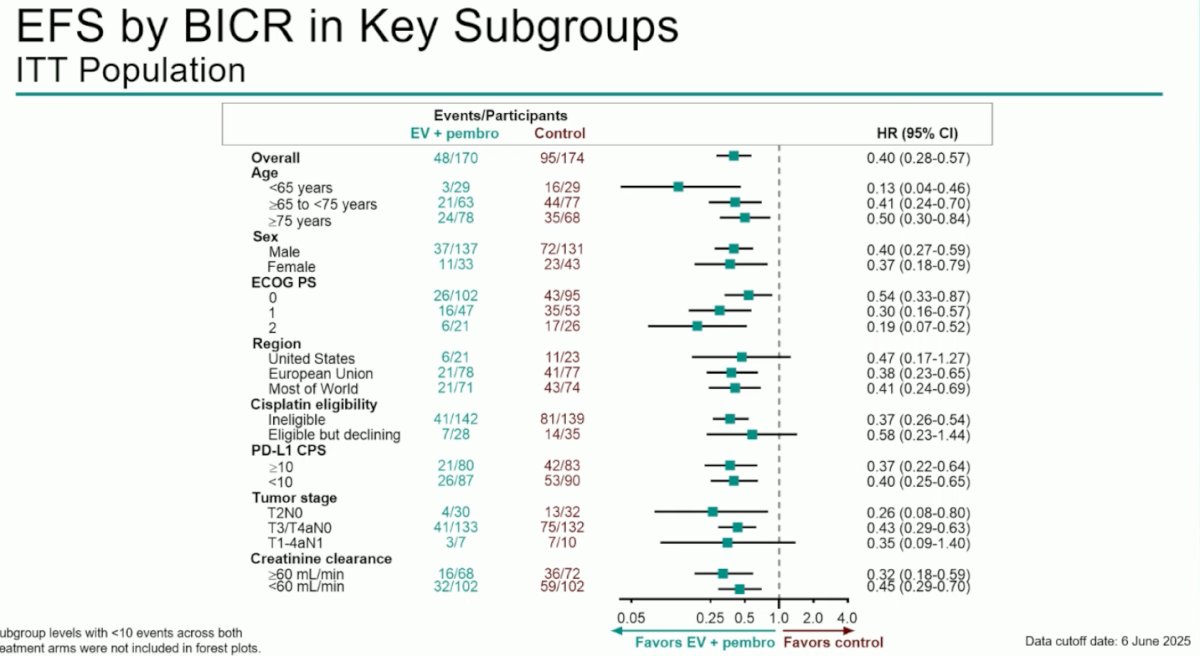
EFS benefit with EV + pembrolizumab was consistent across all predefined subgroups, including age, ECOG performance status, PD-L1 CPS, and tumor stage. The magnitude of benefit was maintained in both cisplatin-ineligible and cisplatin-declining patients, with HRs favoring EV + pembrolizumab across most subgroups.
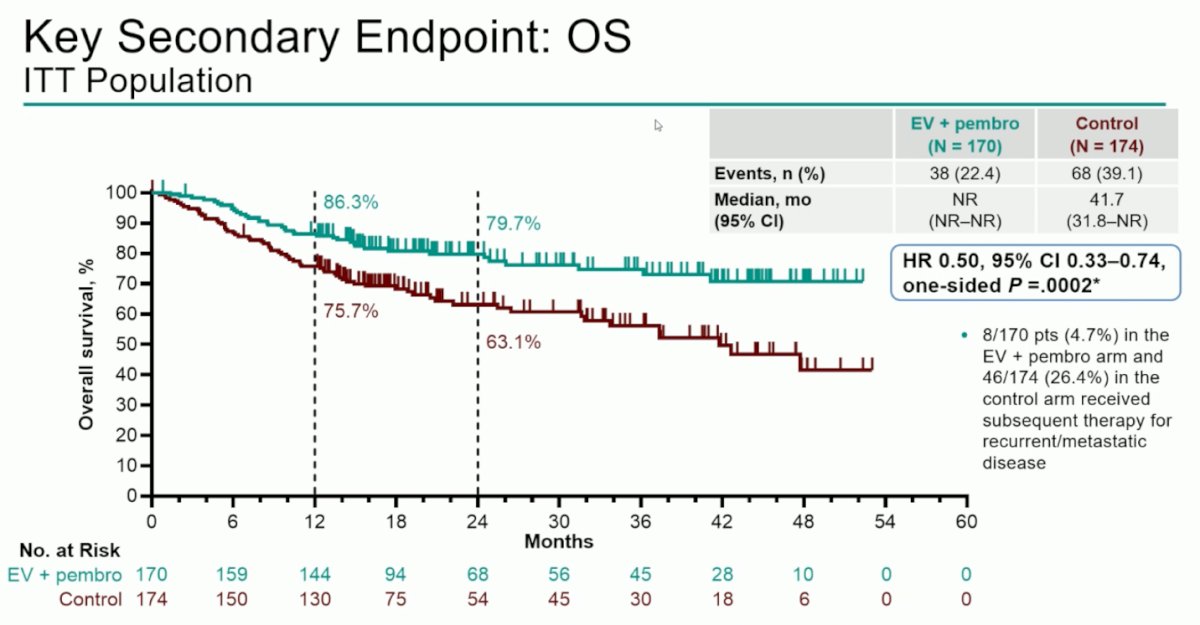
The key secondary endpoint of OS showed a median of 41.7 months in the control arm versus not reached with EV + pembrolizumab (HR 0.50, 95% CI 0.33–0.74; one-sided p=0.0002), with early and sustained separation of the curves. This represents the first trial to demonstrate an OS benefit in cisplatin-ineligible MIBC. Subsequent therapy for recurrent/metastatic disease was received by 4.7% of patients in the EV + pembrolizumab arm versus 26.4% in the control arm.
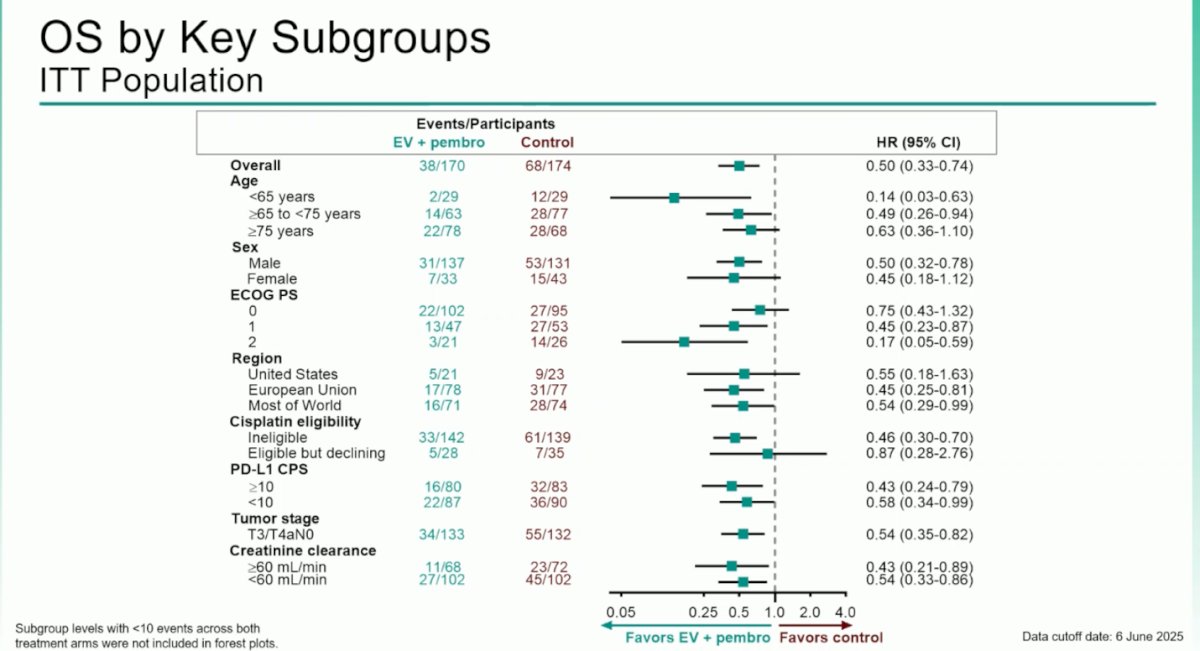
The OS benefit with EV + pembrolizumab was consistent across all predefined subgroups, including age, sex, ECOG status, PD-L1 CPS, and tumor stage, with all hazard ratios favoring the experimental group over control.
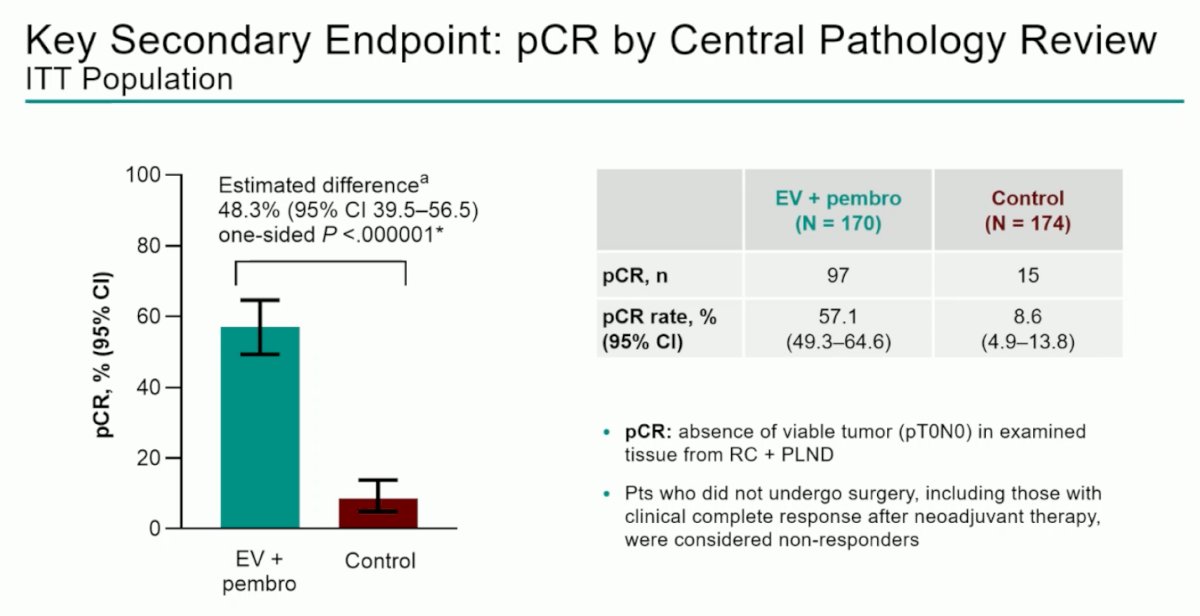
Pathological complete response (pCR), defined as the absence of viable tumor (pT0N0) in RC + PLND specimens, was a key secondary endpoint of the study. The pCR rate was 57.1% with EV + pembrolizumab versus 8.6% with control (estimated difference 48.3%, one-sided p < 0.000001). All ITT patients were included in the denominator, and those not undergoing surgery were considered non-responders. This represents the highest pCR rate ever reported in a phase 3 MIBC trial.
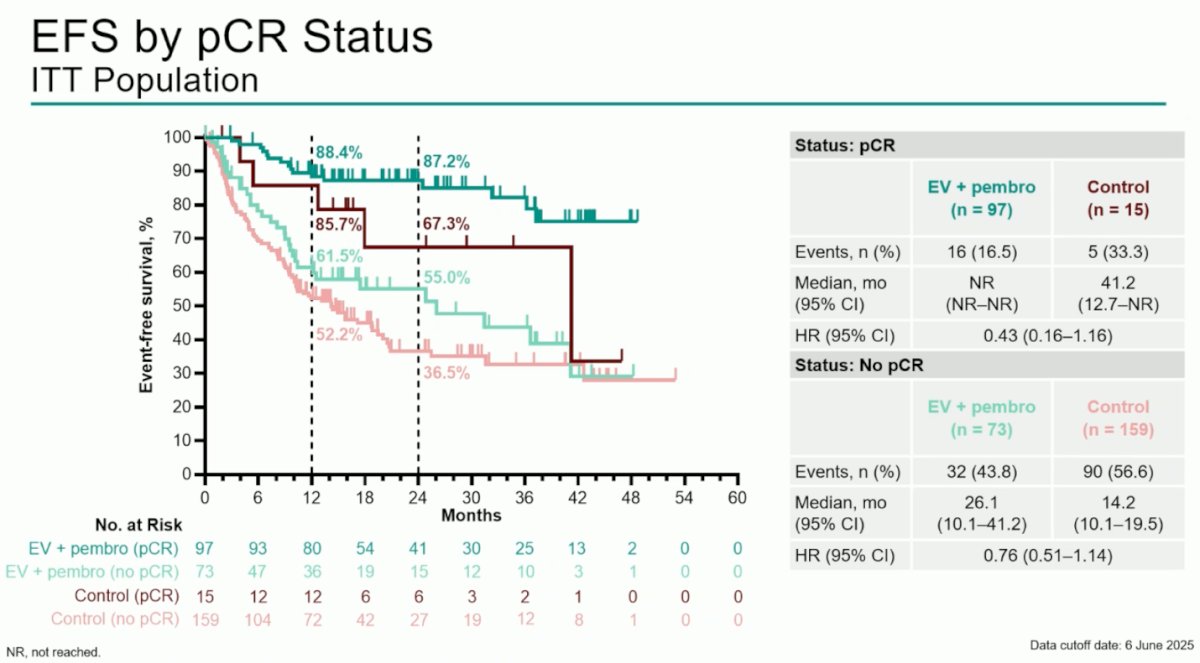
In the exploratory analysis of EFS by pCR status, patients achieving pCR with EV + pembrolizumab had a durable benefit, with median EFS not reached versus 41.2 months in the control arm (HR 0.43). Among those without pCR, median EFS was 26.1 versus 14.2 months (HR 0.76). Interestingly, even patients with pCR in the control arm appeared at higher risk for recurrence compared to those achieving pCR with EV + pembrolizumab.
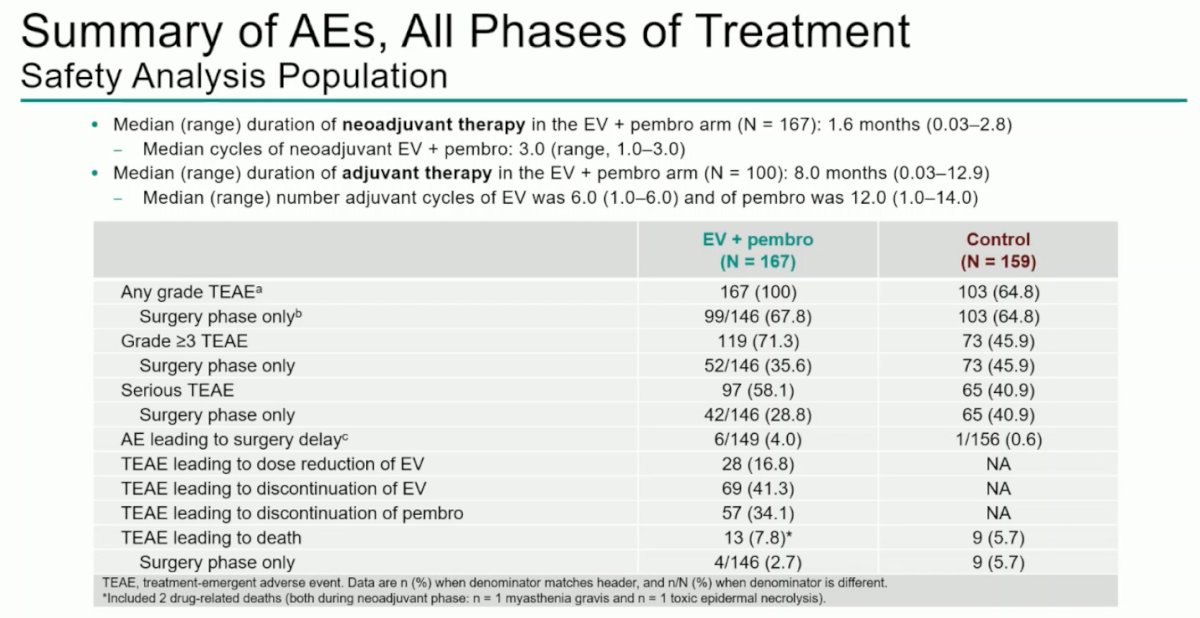
The median duration of neoadjuvant therapy with EV + pembrolizumab was 1.6 months (range, 0.03–2.8) with a median of three cycles. Median adjuvant therapy duration was 8.0 months (range, 0.03–12.9), with six EV and twelve pembrolizumab cycles. The safety profile was consistent with prior experience, with low rates of AEs leading to surgical delay and no apparent increase in surgical complications, despite the frailty and comorbidities of this cisplatin-ineligible population.
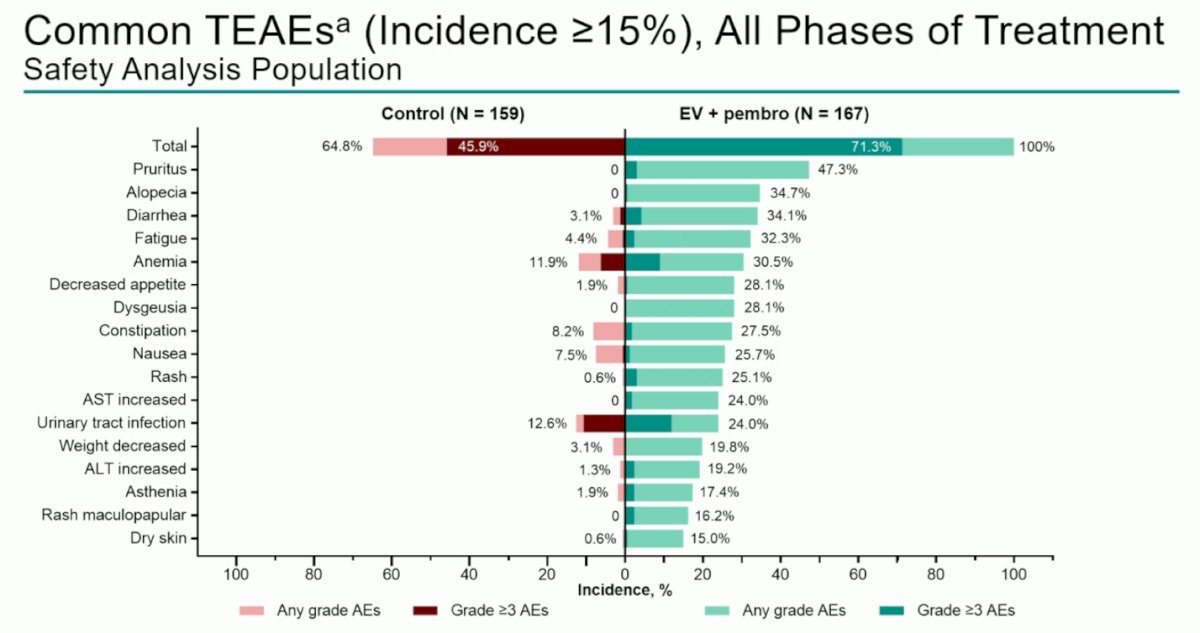
Dr. Vulsteke noted that pruritus and alopecia were among the most common TEAEs observed with EV + pembrolizumab in all phases of treatment, followed by diarrhea, fatigue, and anemia. Most adverse events were low grade and manageable, aligning with the known safety profiles of both agents.
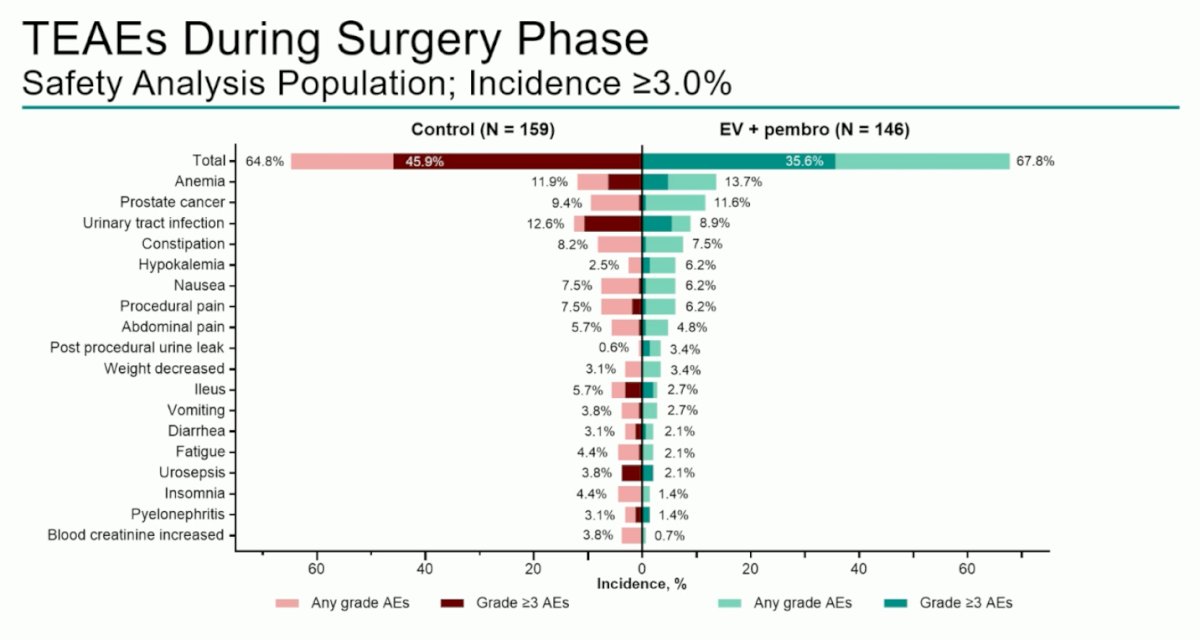
During the surgery phase, anemia and incidental prostate cancer were the most frequently reported TEAEs, with comparable incidence between the EV + pembrolizumab and control arms. No excess perioperative complications or new safety signals were observed with the combination.
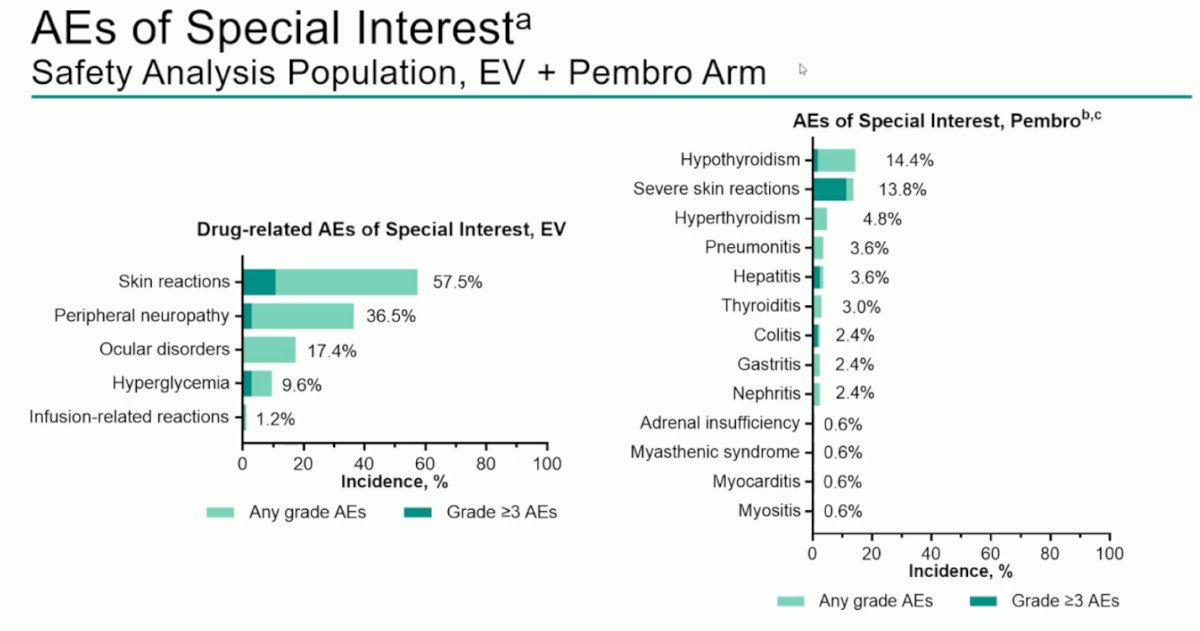
In the EV + pembrolizumab arm, drug-related AEs of special interest included skin reactions (57.5%), peripheral neuropathy (36.5%), and ocular disorders (17.4%). Immune-related AEs associated with pembrolizumab included hypothyroidism (14.4%), severe skin reactions (13.8%), and pneumonitis (3.6%), consistent with known safety profiles.
Dr. Vulsteke concluded his presentation with the following key takeaways:
- Neoadjuvant EV + pembrolizumab followed by RC + PLND and adjuvant EV + pembrolizumab significantly improved EFS, OS, and pCR in cisplatin-ineligible or cisplatin-declining patients with MIBC.
- EFS and OS benefits were consistent across key subgroups.
- Perioperative EV + pembrolizumab did not compromise the ability to undergo curative-intent surgery.
- The safety profile was manageable and consistent with prior experience, with no new safety signals observed.
- Perioperative EV + pembrolizumab may represent a new standard of care for this high-need population.
Presented by: Christof Vulsteke, MD, PhD, Head of the medical oncology clinical trial service of the Integrated Cancer Centre Ghent (IKG), Gent, Belgium.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.
Related content: Phase 3 KEYNOTE-905 Trial Investigates Enfortumab Vedotin Plus Pembrolizumab in Cisplatin-Ineligible Bladder Cancer - Christof Vulsteke
References:
- Powles T, Valderrama BP, Gupta S, Bedke J, Kikuchi E, Hoffman-Censits J, Iyer G, Vulsteke C, Park SH, Shin SJ, Castellano D, Fornarini G, Li JR, Gümüş M, Mar N, Loriot Y, Fléchon A, Duran I, Drakaki A, Narayanan S, Yu X, Gorla S, Homet Moreno B, van der Heijden MS; EV-302 Trial Investigators. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024 Mar 7;390(10):875-888. doi: 10.1056/NEJMoa2312117. PMID: 38446675.
- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, Vu TQ, Antonuzzo L, Wiechno P, Atduev V, Kann AG, Kim TH, Suárez C, Chang CH, Roghmann F, Özgüroğlu M, Eigl BJ, Oliveira N, Buchler T, Gadot M, Zakharia Y, Armstrong J, Gupta A, Hois S, van der Heijden MS; NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):1773-1786. doi: 10.1056/NEJMoa2408154. Epub 2024 Sep 15. PMID: 39282910.
- Galsky MD, Witjes JA, Gschwend JE, Milowsky MI, Schenker M, Valderrama BP, Tomita Y, Bamias A, Lebret T, Shariat SF, Park SH, Agerbaek M, Jha G, Stenner F, Ye D, Giudici F, Dutta S, Askelson M, Nasroulah F, Zhang J, Brophy L, Bajorin DF. Adjuvant Nivolumab in High-Risk Muscle-Invasive Urothelial Carcinoma: Expanded Efficacy From CheckMate 274. J Clin Oncol. 2025 Jan;43(1):15-21. doi: 10.1200/JCO.24.00340. Epub 2024 Oct 11. PMID: 39393026; PMCID: PMC11687940.
- Galsky MD, Hahn NM, Rosenberg J, Sonpavde G, Hutson T, Oh WK, Dreicer R, Vogelzang N, Sternberg CN, Bajorin DF, Bellmunt J. Treatment of patients with metastatic urothelial cancer "unfit" for Cisplatin-based chemotherapy. J Clin Oncol. 2011 Jun 10;29(17):2432-8. doi: 10.1200/JCO.2011.34.8433. Epub 2011 May 9. PMID: 21555688.