(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma mini oral session and a presentation by Dr. Andrea Necchi discussing the SunRISe-4 primary analysis and biomarker results assessing neoadjuvant TAR-200 + cetrelimab or cetrelimab alone in patients with muscle-invasive bladder cancer. The standard of care for muscle-invasive bladder cancer (T2-T4aN0M0) is radical cystectomy + neoadjuvant chemotherapy, or chemoradiation for select patients.
However, many patients are ineligible (up to 50%) or refuse cisplatin, thus for these patients, the standard of care is immediate radical cystectomy. In patients with muscle-invasive bladder cancer undergoing radical cystectomy, pathologic stage is a prognostic factor for survival. Moreover, pathological complete response in patients who have received neoadjuvant chemotherapy is associated with a 55% lower risk of death and an 81% lower risk of recurrence compared to patients with residual disease. There is a need for effective and more tolerable treatment options for patients with muscle-invasive bladder cancer who are candidates for radical cystectomy, but not candidates for neoadjuvant chemotherapy.
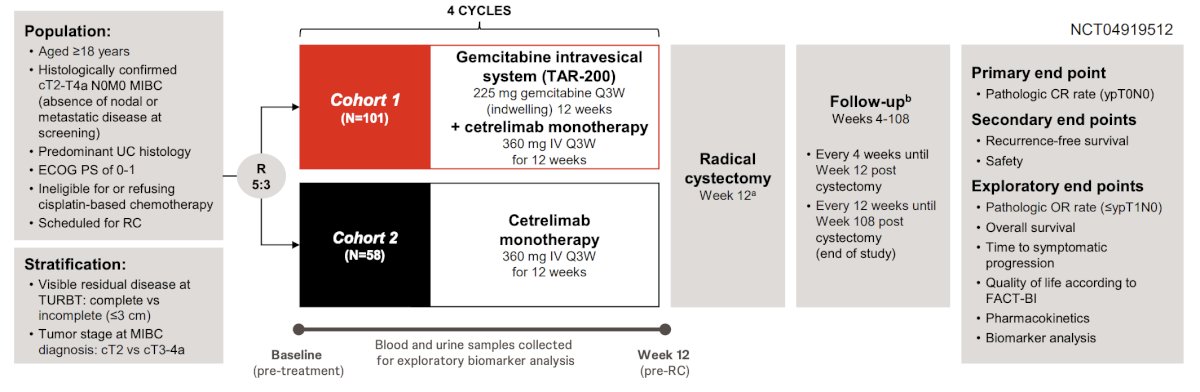
SunRISe-4 is an open-label, multicenter, parallel cohort phase 2 study assessing neoadjuvant TAR-200 + cetrelimab (cohort 1) or cetrelimab alone (cohort 2) in patients with muscle-invasive bladder cancer scheduled for radical cystectomy and ineligible/refusing neoadjuvant platinum-based chemotherapy. At the ESMO 2025 annual meeting, Dr. Necchi and colleagues reported the efficacy and safety from the primary analysis of SunRISe-4, and urinary (utDNA) and circulating tumor DNA (ctDNA) minimal residual disease as biomarkers of outcomes agnostic to treatment.
Eligible patients planned for radical cystectomy had an age ≥18 years, ECOG performance status 0-1, cT2-T4a N0M0 muscle-invasive bladder cancer and were ineligible/refusing neoadjuvant platinum-based chemotherapy. Patients were randomized 5:3, stratified by TURBT completeness (residual tumor ≤3 cm permitted) and T stage, to receive TAR-200 + cetrelimab (cohort 1) or cetrelimab alone (cohort 2). The primary endpoint was the pathologic complete response rate at radical cystectomy. Additional end points included pathologic overall response (defined as ≤ypT1) rate, recurrence-free survival, safety, and utDNA/ctDNA:
Of 159 patients enrolled, the median age was 73 years, 83% were male, 83% had visibly complete TURBT, 24% had variant histology, and 81% had cT2 disease:

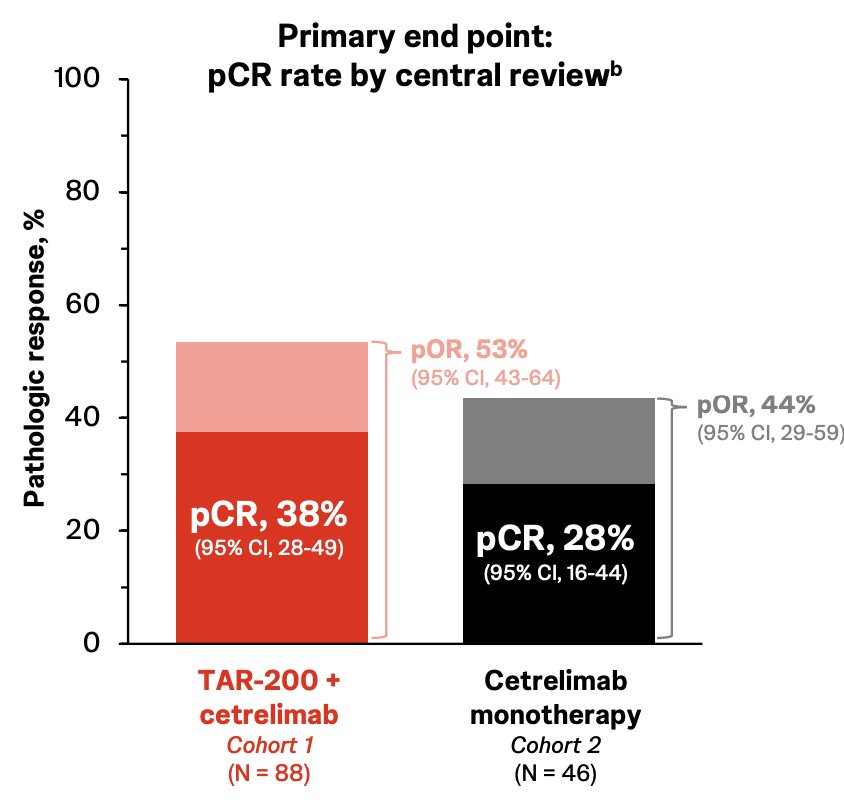
Overall, 87% (88/101) of patients in cohort 1 and 79% (46/58) in cohort 2 underwent radical cystectomy. Pathologic complete response was 38% in cohort 1 versus 28% in cohort 2, which was also associated with an improved pathologic overall response in cohort 1 (53%) versus cohort 2 (44%):
The 1-year recurrence-free survival rate was higher in cohort 1 (77%, 95% CI 67-85) than in cohort 2 (64%, 95% CI 47-77): 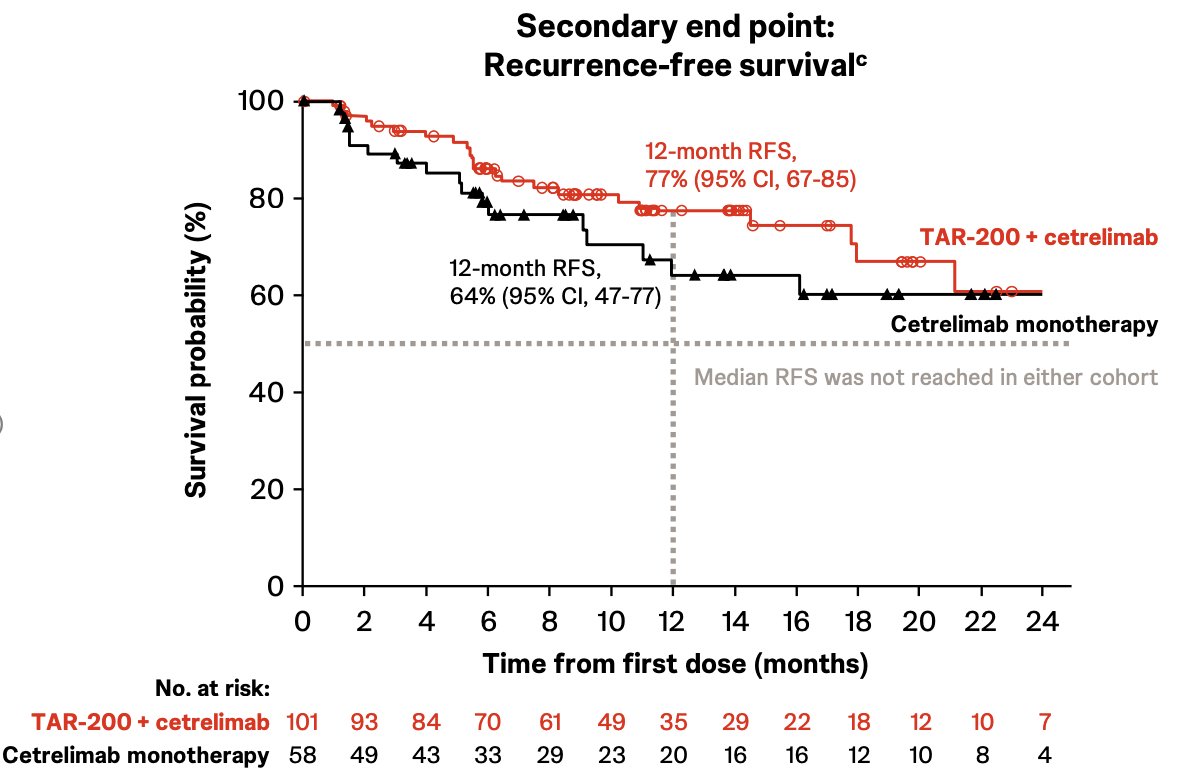
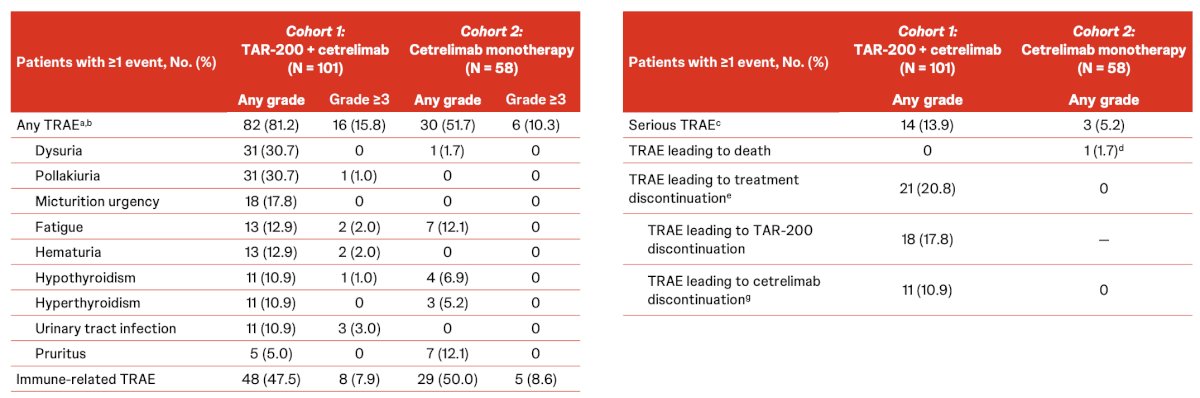
No new safety signals for TAR-200, cetrelimab, or the combination were observed:
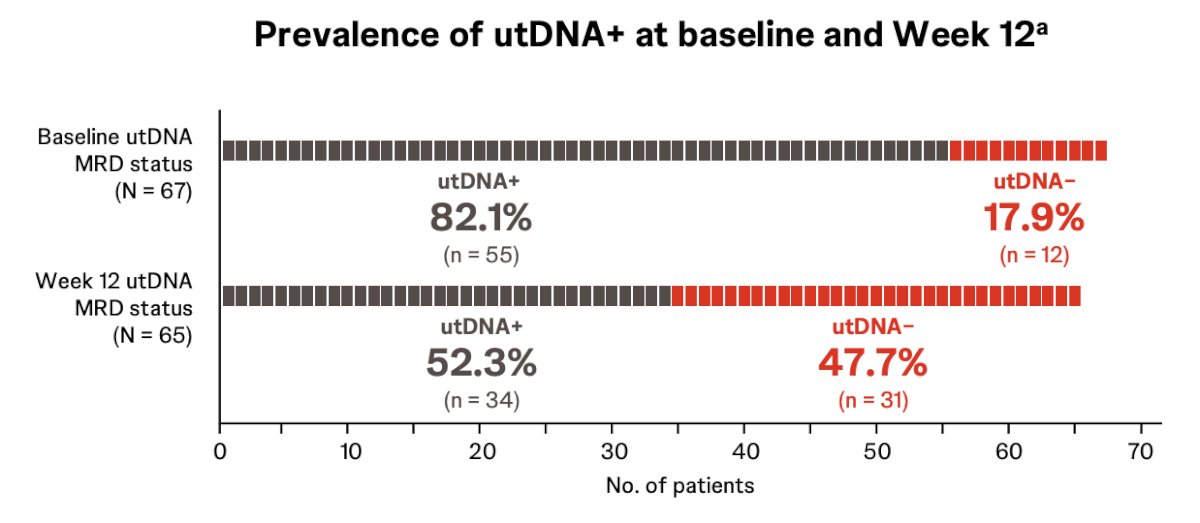
The proportion of patients who were utDNA positive was reduced from baseline to week 12, irrespective of treatment. In cohort 1, 77.8% and 50.0% of patients were utDNA positive at baseline and week 12, respectively. In cohort 2, 90.9% and 55.6% of patients were utDNA positive at baseline and week 12, respectively. There were no meaningful differences observed between the cohorts, though the sample sizes were limited:
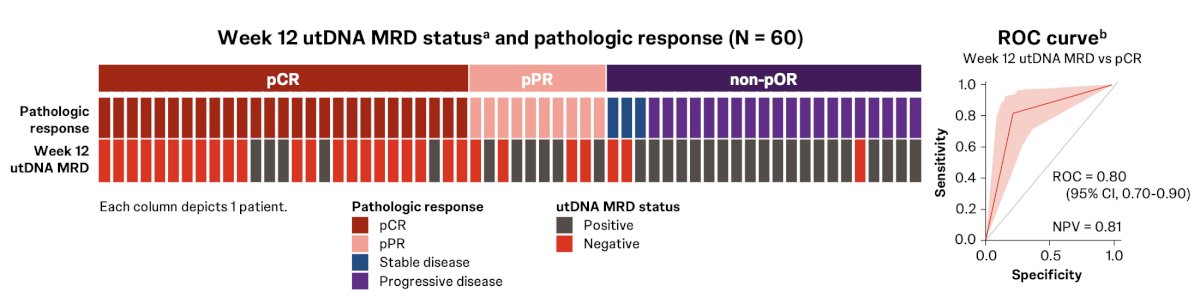
Overall, 22 of 27 patients (81.5%) who achieved a pathologic complete response were utDNA negative at week 12, compared with 7 of 33 (21.2%) who did not achieve pathologic complete response (p < 0.00001):
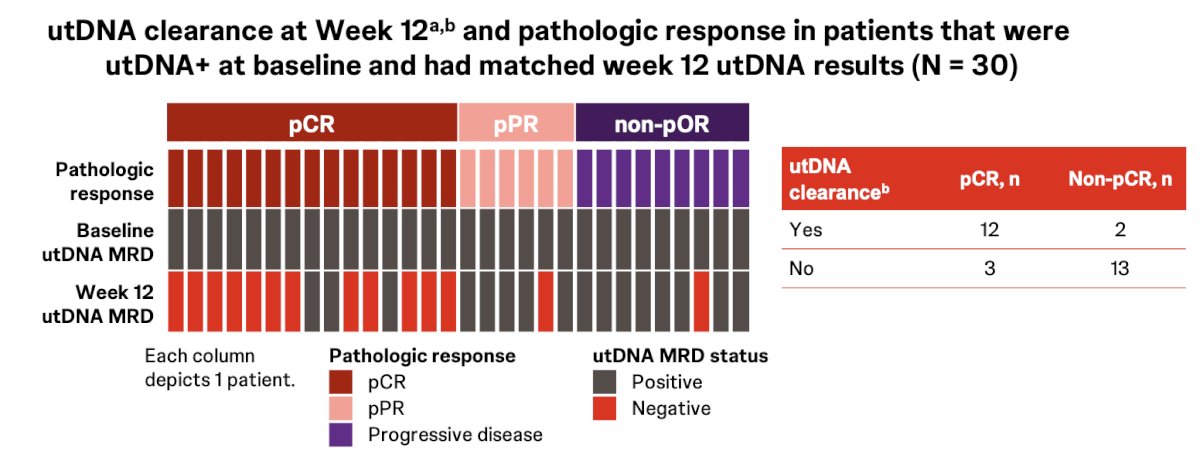
Of 30 patients who were utDNA positive at baseline and had matched week 12 utDNA results, 14 (46.7%) had utDNA clearance at week 12. Moreover, 12 of 15 patients (80%) who were utDNA positive at baseline and achieved a pathological complete response had utDNA clearance at week 12, compared with 2 of 15 (13.3%) who did not achieve a pathologic complete response (p = 0.0006):
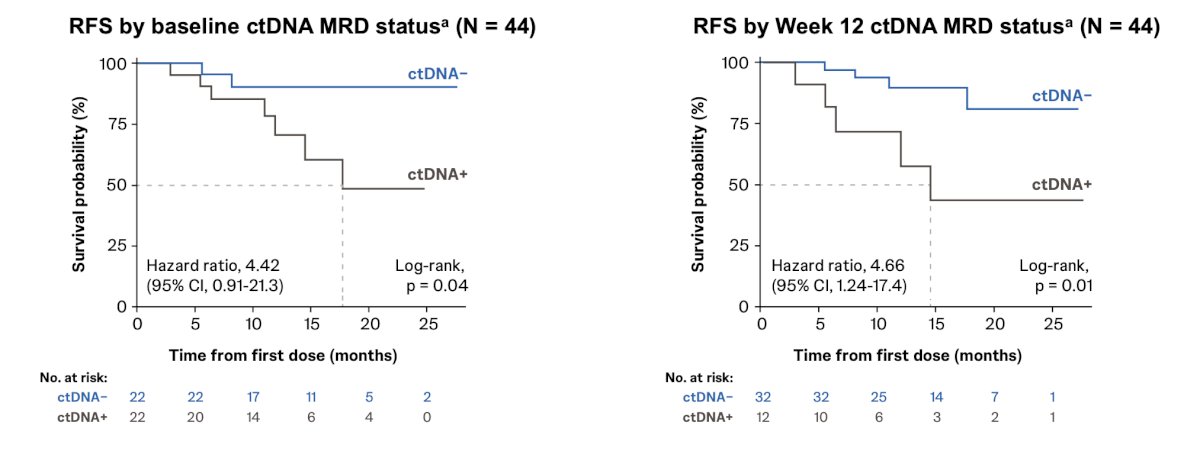
ctDNA negative status at baseline and week 12 was associated with longer recurrence-free survival:
However, week 12 ctDNA minimal residual disease status (p = 0.12) and ctDNA clearance at week 12 (p = 0.15) were not statistically associated with pathologic complete response.
Dr. Necchi concluded his presentation discussing the SunRISe-4 primary analysis and biomarker results with the following take-home points:
- At the primary analysis of SunRIse-4, neoadjuvant gemcitabine intravesical system + cetrelimab showed a high pathologic complete response rate (38%) and 12-month recurrence-free survival rate (77%), supporting further investigation of the combination in muscle-invasive bladder cancer
- Cetrelimab monotherapy showed a pathologic complete response rate (28%) and 12-month recurrence-free survival rate (64%), consistent with previous studies of neoadjuvant checkpoint inhibitor monotherapy
- No new safety signals were observed in either treatment cohort
- Exploratory utDNA/ctDNA minimal residual disease results support further investigation as predictive biomarkers for residual disease after neoadjuvant therapy in muscle-invasive bladder cancer:
- At baseline, 82% of patients with visibly complete TURBT were utDNA positive
- utDNA negative status at week 12, as a potential marker of local disease, was strongly associated with pathologic complete response
- ctDNA negative status, as a potential marker of non-local disease, was strongly associated with longer recurrence-free survival, but not associated with pathologic complete response
Presented by: Andrea Necchi, MD, Chief of Genitourinary Medical Oncology, IRCCS San Raffaele Hospital and Scientific Institute, Professor of Oncology, Vita-Salute San Raffaele University, Milan, Italy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.