(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma mini oral session and a presentation by Dr. Nicholas D. James discussing final survival analysis results from the BladderPath trial assessing upfront MRI versus transurethral resection for staging new bladder cancers. TURBT has been the mainstay of bladder cancer staging for more than 60 years. However, staging inaccuracies are commonplace, leading to delayed treatment of muscle-invasive bladder cancer (often >100 days). Multiparametric MRI offers rapid, accurate and non-invasive staging of muscle-invasive bladder cancer. Dr. James and colleagues previously reported that upfront MRI speeds time to definitive treatment for muscle-invasive bladder cancer (98 days (95% CI 72-125) versus 53 days (95% CI 20-89)). At the ESMO 2025 annual meeting, they reported mature 2 year outcomes from the BladderPath trial.
BladderPath was an open-label, multistage randomized controlled study in 15 sites in three parts: feasibility (percentage of patients completing the MRI pathway as planned), intermediate (reduction of at least 30 days in time to correct treatment for muscle invasive bladder cancer), and final (progression free and overall survival) clinical stages. The final stage was cut short by the COVID pandemic.
Newly presenting patients with bladder mass at flexible cystoscopy referred for TURBT were randomized to Pathway 1 TURBT or Pathway 2, which added initial MRI for patients with possible muscle-invasive bladder cancer (about 50% of total). Subsequent therapy could include TURBT, which occurred in approximately 85% Pathway 2 patients (main reasons: staging uncertainty, debulking, assess variant histology). Data collected during the trial were merged with NHS Digital records to provide death and progression information, and cause of death was reviewed using a Likert scale for all patients.
Between May 31, 2018, and December 31, 2021, 143 participants were randomized. Overall, there were 25% of patients who died, with the causes listed in the following table:

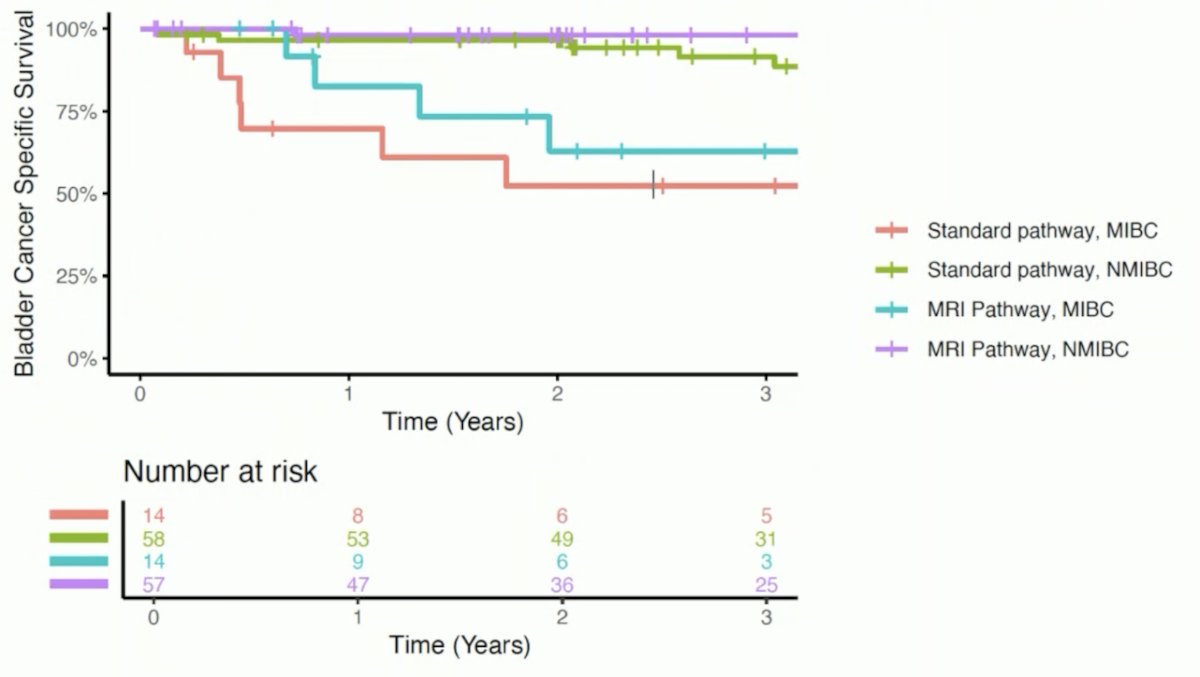
Progression free survival split between the standard versus MRI pathway showed no difference; however, there appeared to be a clinically meaningful benefit for the MRI pathway among non muscle invasive bladder cancer patients:

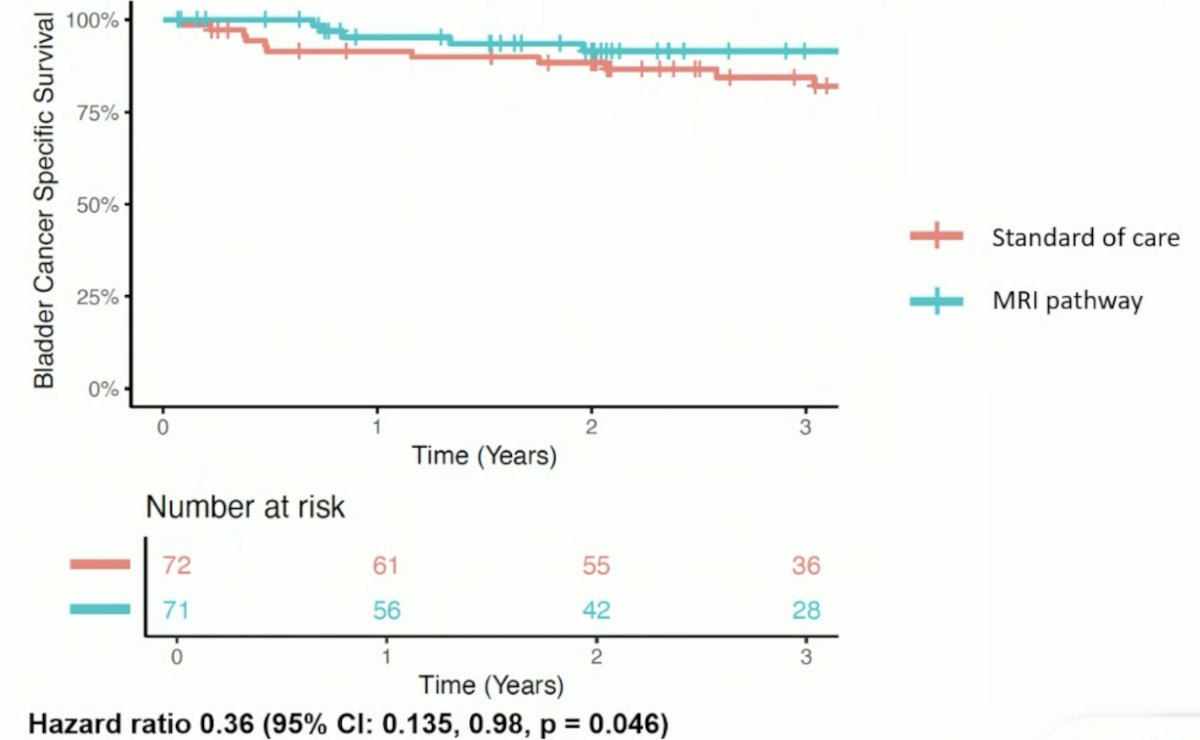
Bladder cancer specific deaths included 18% in the standard pathway, and 10% in the MRI pathway, with a bladder cancer specific survival HR 0.36 (95% CI 0.12, 0.98, p = 0.046):
There also appeared to be a clinically meaningful benefit for the MRI pathway among muscle invasive bladder cancer patients:
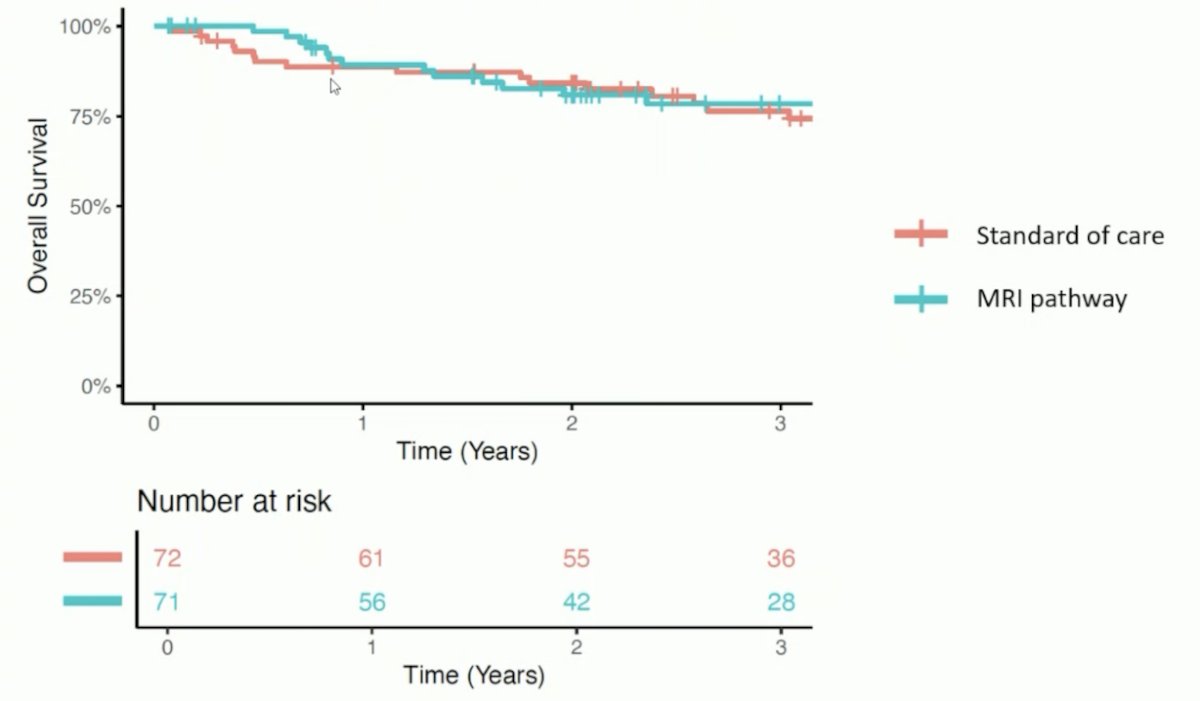
There were 28% of patients that died in the standard pathway and 23% in the MRI pathway, with an overall survival of HR 0.67 (95% CI 0.34, 1.33, p = 0.25):
Dr. James concluded his presentation discussing final survival analysis results from the BladderPath trial with the following take home points:
- There were strong trends for improvement in all key trial metrics
- There was no evidence of detriment on outcomes from the MRI based pathway
- There was a statistically significant improvement in bladder cancer specific survival for the MRI guided pathway
Presented by: Nicholas D. James, MBBS, PhD, The Royal Marsden NHS Foundation Trust, London, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between September 17th and 21st.
Related Content:
Analysis of MRI Use in the Diagnostic Pathway for Bladder Cancer - Nicholas James