(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma proffered paper session and a presentation by Dr. Andrea Necchi discussing primary results of the GDFather-NEO trial, a blinded, exploratory phase 2 trial of nivolumab and the GDF-15 neutralizing antibody visugromab or placebo as neoadjuvant treatment of patients with muscle-invasive bladder cancer. Approximately 50% of patients with muscle invasive bladder cancer are unfit for neoadjuvant chemotherapy, and a further proportion of them refuse to receive neoadjuvant chemotherapy. With radical cystectomy alone, the 5-year survival rate for muscle invasive bladder cancer is ~30–50%, and ~50% with neoadjuvant chemotherapy and radical cystectomy. The development of effective and safe neoadjuvant treatments in “window-of-opportunity” trials remains critical for patients with muscle invasive bladder cancer. Several neoadjuvant strategies with anti–PD-(L)1 inhibitors have been leveraged with positive signals of pathological response, at or around the chemotherapy response level. Adding anti–PD-(L)1 therapy to neoadjuvant chemotherapy often had a limited, non-additive effect on pathological response rates in several phase 2 trials. Patients’ concerns about undergoing radical cystectomy increase after achieving a clinical complete response to treatment, and response-adapted bladder-saving strategies have been conceptualized.
Growth and Differentiation Factor 15 (GDF-15) is a remote TGF-b superfamily member linked to feto-maternal tolerance and tissue stress response, and was recently identified as a key mediator of resistance to PD-(L)1 blockade in metastatic solid tumors.1 Visugromab is a GDF-15 neutralizing IgG4 antibody with initial safety and efficacy data in patients with anti-PD(L)1 relapsed/refractory solid tumors in combination with nivolumab, explored in the GDFATHER-01 trial. At the 2025 ESMO annual meeting, Dr. Necchi and colleagues reported the primary results of an exploratory, biomarker oriented, phase 2 trial of nivolumab + visugromab or placebo as neoadjuvant treatment in patients with muscle invasive bladder cancer.
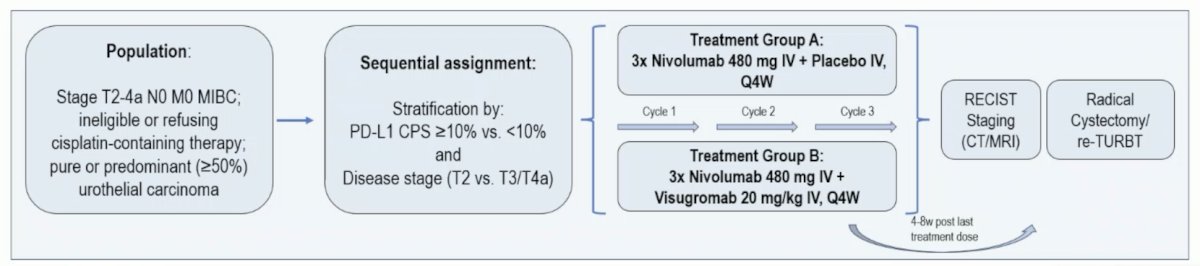
The multicenter GDFather-NEO trial investigated visugromab (aGDF-15; 20 mg/kg) in combination with nivolumab (480 mg) versus nivolumab + placebo, administered every 4 weeks for 3 cycles in cisplatin-ineligible/refusing participants with newly diagnosed clinical stage T2-T4aN0M0 muscle-invasive bladder cancer. Participants were centrally stratified for PD-L1 CPS and cT-stage. Radical cystectomy or re-TURBT was performed 4-8 weeks after last dose. Key endpoints were pathologic complete response (ypT0), major pathologic response (ypT<=1), and radiologic objective response rate (RECIST v1.1). The trial design is as follows:
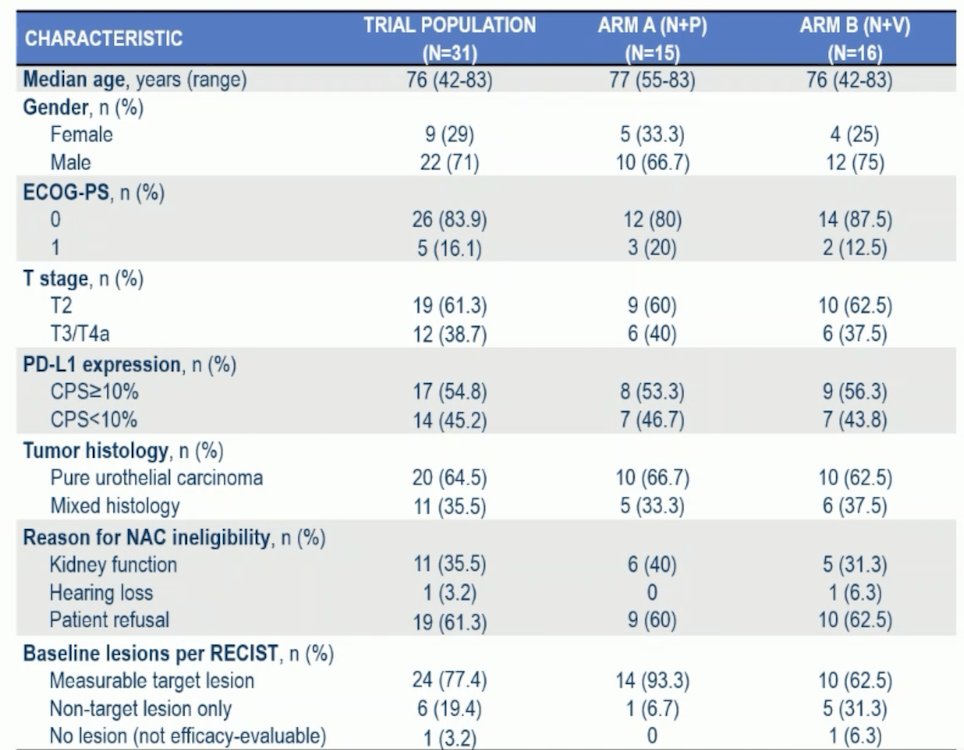
Of 31 participants enrolled between September 2023 and March 2025, the baseline characteristics are as follows:
At the data cutoff of September 29, 2025, the median time from cycle 1 day 1 to re-TURBT was in line with the protocol allowed window (15.1 weeks in Arm A, 16.0 weeks in Arm B). There were no grade 4/5 treatment related adverse events observed in any of the arms:
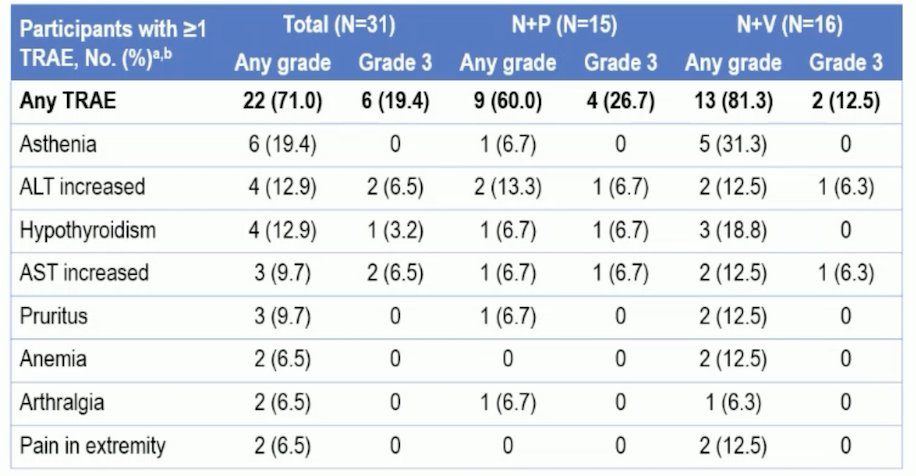
There were two serious adverse events in two participants judged to be related to visugromab + nivolumab (grade 3 immune-mediated liver injury; grade 2 interstitial pneumonia, both of which resolved without sequelae). One serious adverse event was considered related to nivolumab in the placebo arm (grade 3 hypothyroidism). Treatment was discontinued due to treatment related adverse events in two patients, both in the nivolumab + placebo arm.
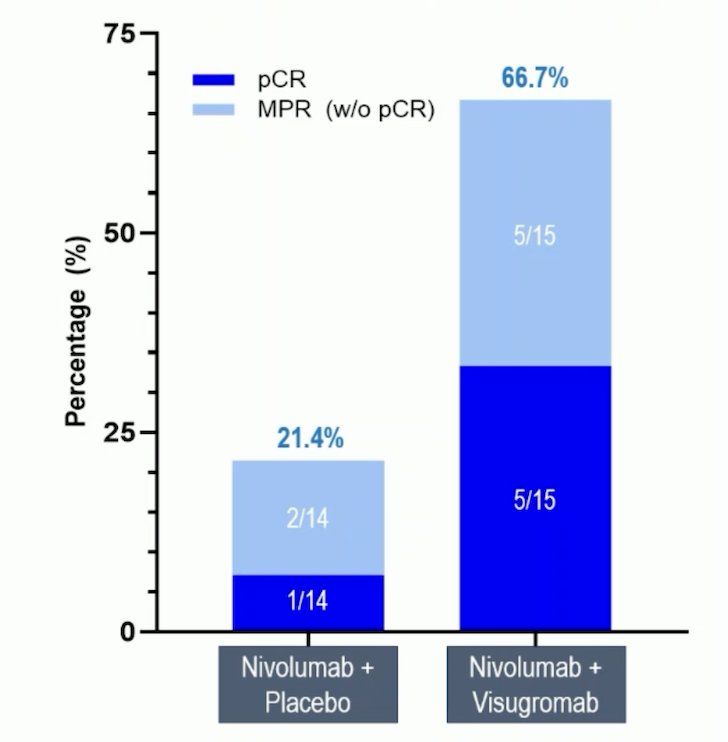
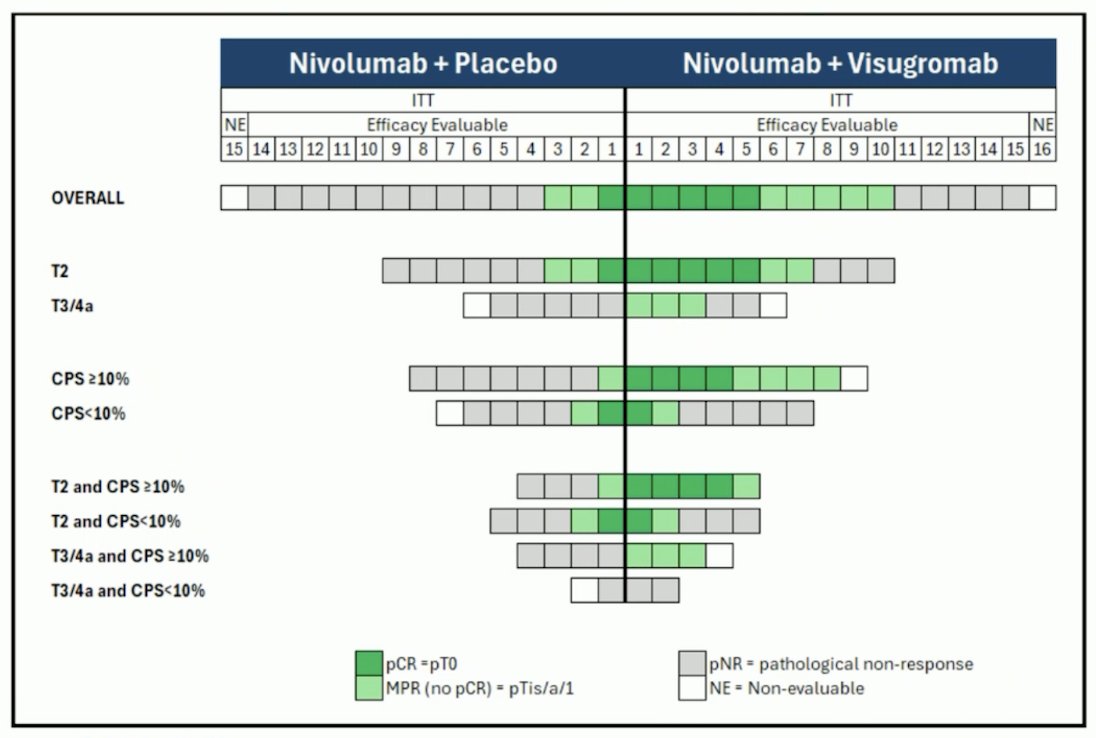
Regarding efficacy (29 of 31 evaluable), pathologic complete response (33.3% versus 7.1%) and major pathologic response (66.7% versus 21.4%) rates were substantially higher for nivolumab + visugromab versus nivolumab + placebo:
Nivolumab + visugromab was superior across all T stages and dominantly in CPS≥10%:
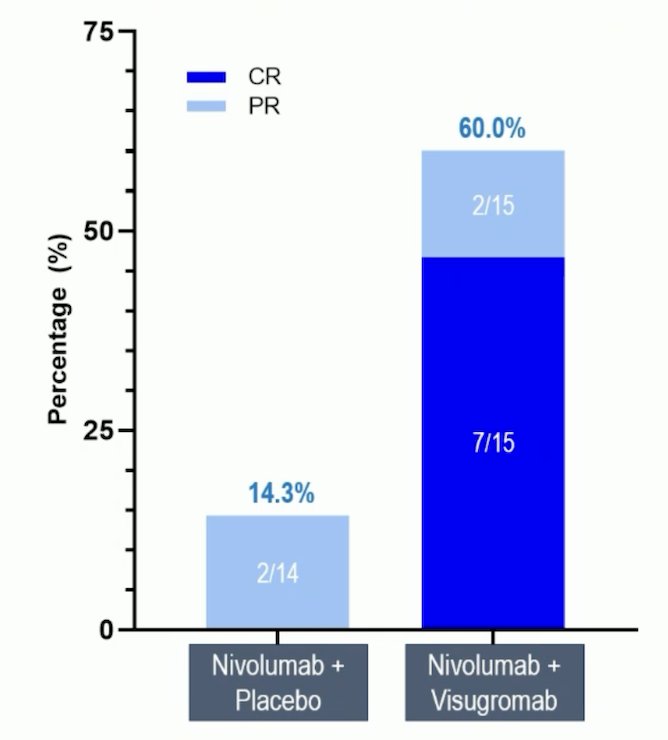
Objective response rate as per RECIST v1.1 was 60.0% (7 complete responses, 2 partial responses) versus 14.3% (no complete responses, 2 partial responses) for nivolumab + visugromab versus nivolumab + placebo:
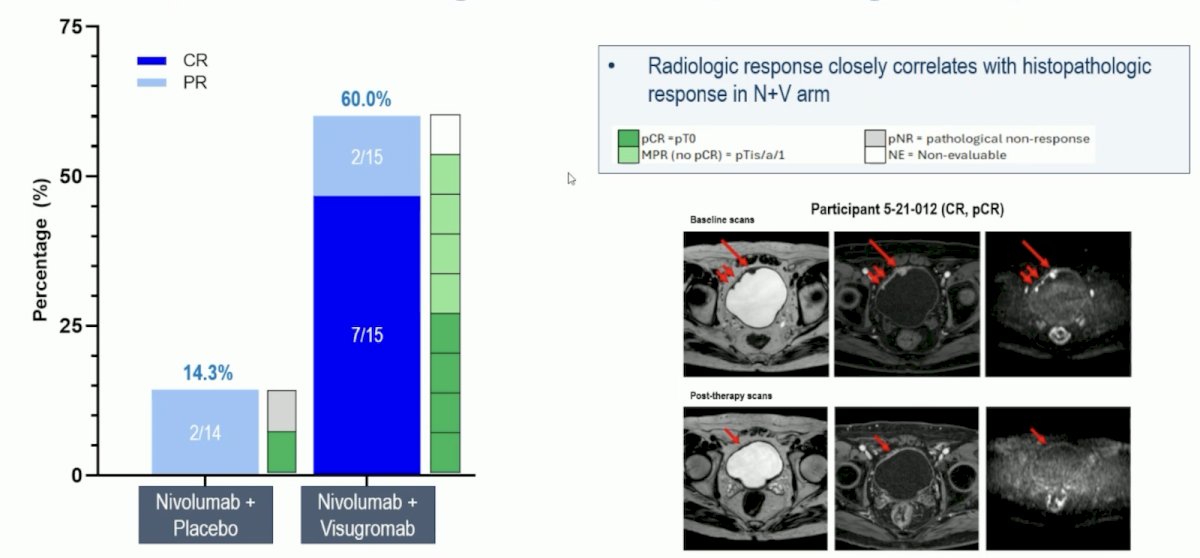
Radiologic responses correlated with histopathologic response in the nivolumab + visugromab arm:
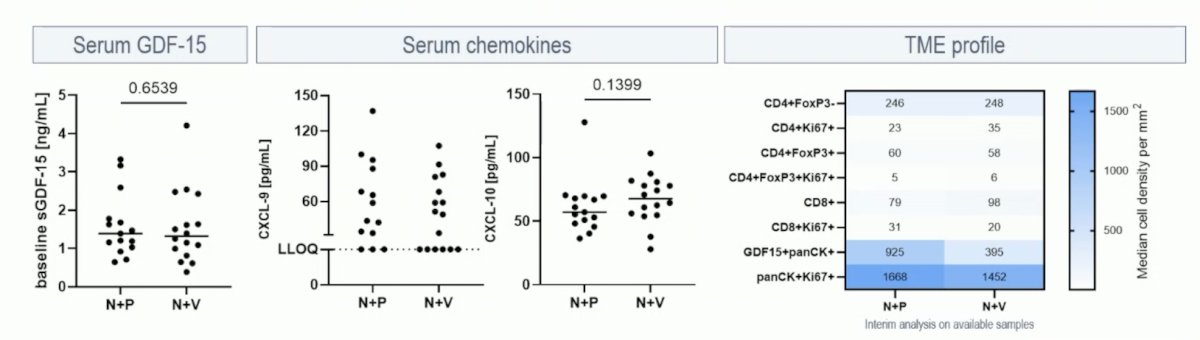
Comparative analysis of blood and tumor microenvironment characteristics between the treatment arms showed (i) elevated and comparable serum GDF-15 levels, (ii) no difference in serum CXCL-9 and CXCL-10 levels, and (iii) similar tumor microenvironment profile (immune cell density, proliferative status):
Dr. Necchi concluded his presentation discussing primary results of the GDFather-NEO trial with the following take home points:
- In anti–PD(L)-1 naïve muscle invasive bladder cancer, addition of GDF-15 blockade by visugromab tripled the effect size of nivolumab as neoadjuvant therapy before surgery
- The combination of nivolumab with visugromab showed good tolerability, with no apparent increase in toxicity versus the safety profile expected for checkpoint inhibitor monotherapy. Definitive safety assessment will only be possible after database lock and will require larger sample sizes in future trials
- Clinical and translational baseline characteristics show no difference between both treatment arms (further biomarker analyses with focus on treatment-induced changes are ongoing)
- The combination of visugromab with PD-1 blockade warrants further investigation in larger neoadjuvant trials with a tumor response-guided bladder preservation approach
- Limitations include: a small sample size, and a different percentage of re-TURBT between arms
- A phase 2b program with randomized trials in first line NSCLC (NCT07098988; recruiting), second line NSCLC, second line HCC, and cachexia is underway.
- Long-term follow-up data from the phase 1/2a GDFATHER trial (NCT04725474) evaluating visugromab in combination with nivolumab in anti–PD1/L1 relapsed/refractory metastatic solid tumors will also be presented by Dr. Melero at ESMO 2025, demonstrating deep and long-term remissions in various indications including urothelial carcinoma
Presented by: Andrea Necchi, MD, Vita-Salute San Raffaele University, Milan, Italy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between September 17th and 21st.
Related content: Phase 2 Trial of Neoadjuvant Nivolumab and Visugromab in Bladder Cancer Patients - Andrea Necchi
References:
- Melero I, de Miguel Luken M, de Velasco G, et al. Neutralizing GDF-15 can overcome anti-PD-1 and anti-PD-L1 resistance in solid tumours. Nature. 2025 Jan;637(8048):1218-1227.