(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma proffered paper session and a presentation by Dr. Maria De Santis discussing POTOMAC, a phase 3, randomized, open-label, trial of durvalumab in combination with BCG for BCG-naïve high-risk non muscle-invasive bladder cancer. Standard treatment for high-risk non muscle-invasive bladder cancer is TURBT followed by BCG induction + maintenance therapy, but early recurrence and progression are common (∼40% of patients within 2 years). Patients who experience early recurrence of high risk disease or who develop BCG-unresponsive disease have an increased risk of progression to muscle invasive bladder cancer or metastatic disease, and for most of the patients, the recommended treatment is radical cystectomy. Combining durvalumab with BCG may improve long term outcomes for patients with BCG-naïve, high risk non muscle invasive bladder cancer. BCG stimulates the immune system by initiating and/or expanding anti-tumor cells, while durvalumab extended the activity of cytotoxic T cells, for a more durable response. POTOMAC evaluated whether 1 year of durvalumab (anti–PD-L1 antibody) + BCG induction + maintenance therapy improved outcomes versus BCG (induction + maintenance) alone in patients with BCG-naïve, high-risk non muscle-invasive bladder cancer.
Eligible adult patients with BCG-naïve, local histologically confirmed high-risk non muscle-invasive bladder cancer who had TURBT (complete resection, including patients with residual CIS) were randomized 1:1:1 to receive durvalumab + BCG (induction + maintenance), durvalumab + BCG induction only, or BCG (induction + maintenance). Durvalumab was administered intravenously (1500 mg every 4 weeks for 13 cycles), and intravesical BCG was given weekly × 6 weeks (induction only) and as 3 weekly doses at 3, 6, 12, 18, and 24 months. Patients were stratified by higher risk papillary disease and CIS. The primary endpoint was investigator-assessed disease free survival with durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance). The trial design for POTOMAC is as follows:
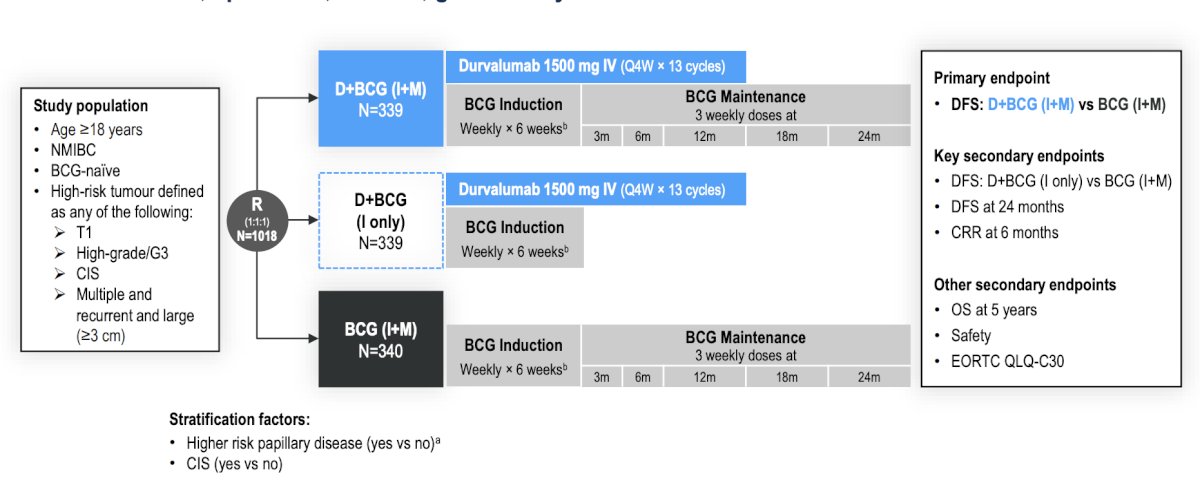
From a statistical standpoint, to control for the type I error at the 5% (2-sided) alpha level, a multiple testing procedure with a gatekeeping strategy was used across the key endpoints. In this planned final analysis (data cutoff of April 3, 2025), the estimated number of events across the durvalumab + BCG (induction + maintenance) and BCG (induction + maintenance) arms was 158 disease free survival (intention to treat). The actual number of events was 165. Disease free survival was defined as:
- Recurrence of high-risk non muscle invasive bladder cancer (T1, high-grade Ta, or CIS)
- Presentation with muscle invasive bladder cancer and/or metastatic disease
- Persistent CIS at 6 months
- Death by any cause in the absence of recurrence
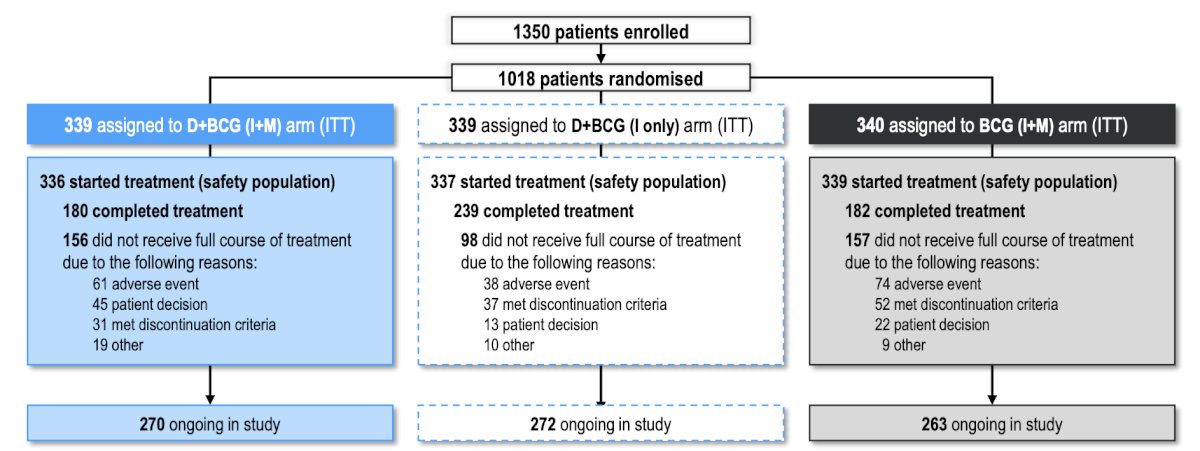
There were 1,018 patients randomized: 339 to durvalumab + BCG (induction + maintenance), 339 to durvalumab + BCG (induction only), and 340 to BCG (induction + maintenance). The complete patient disposition is as follows:
Demographic and disease characteristics were generally well balanced between the three arms:

BCG treatment exposure was similar between durvalumab + BCG (induction + maintenance) and BCG (induction + maintenance) arms, and BCG compliance was high, with a median number of BCG maintenance instillation of 14.0 in both arms:

The median follow-up was 60.7 months. The primary endpoint of disease free survival was met with a 32% reduction in risk of recurrence of high-risk disease or death by any cause for durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance) (HR 0.68, 95% CI 0.50–0.93; log-rank p = 0.0154), and 24-month disease free survival rates were 86.5% (95% CI 82.2–89.8) for durvalumab + BCG (induction + maintenance) and 81.6% (95% CI 76.9–85.3) for BCG (induction + maintenance):

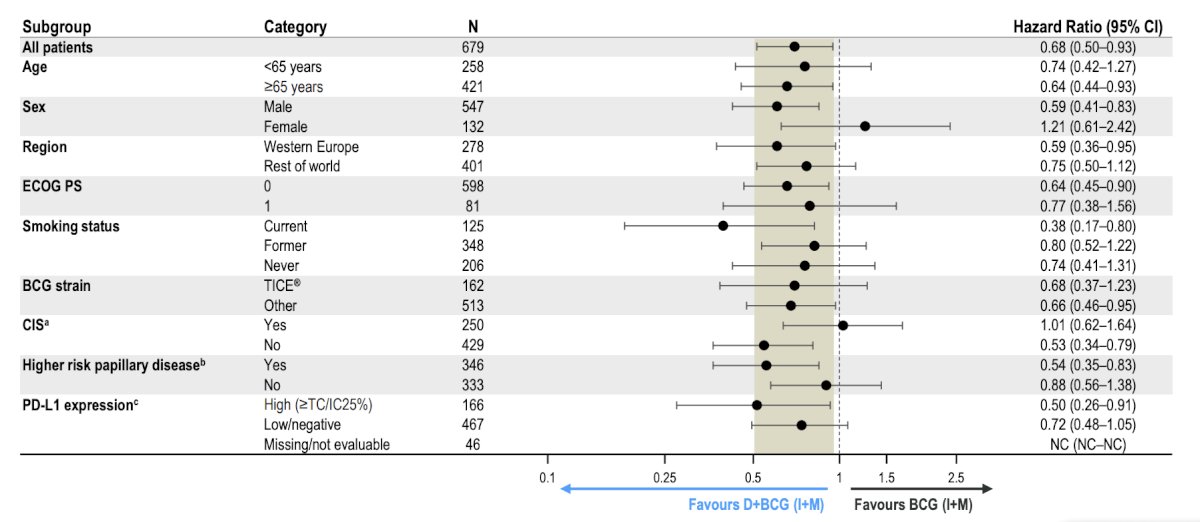
In the disease free survival subgroup analyses, there was a generally consistent treatment effect across subgroups for durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance) arms:
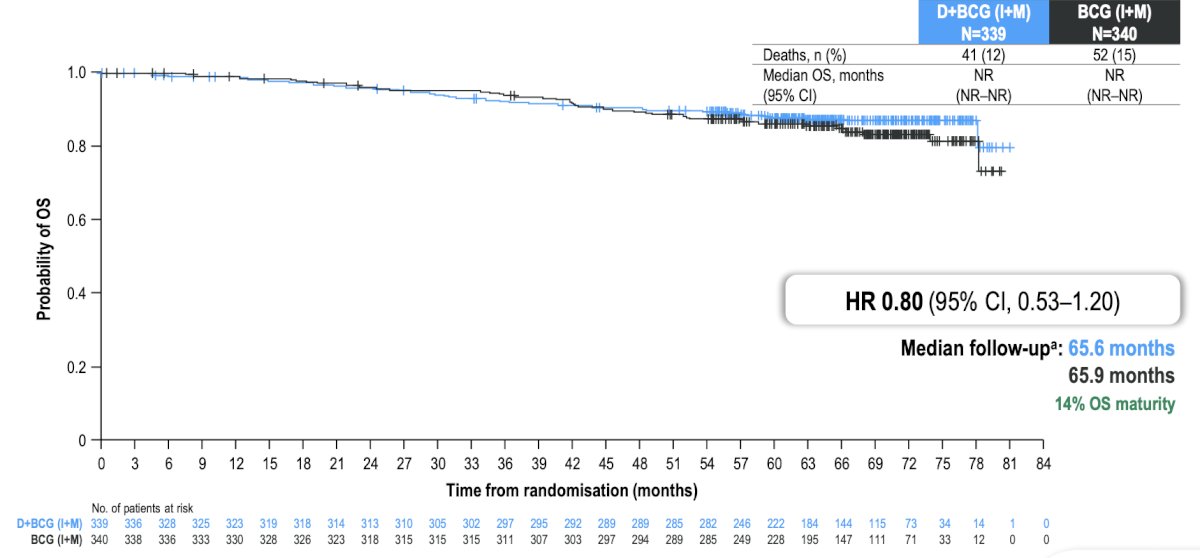
No evidence of overall survival detriment was seen with durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance) (descriptive analysis: HR 0.80, 95% CI 0.53–1.20):
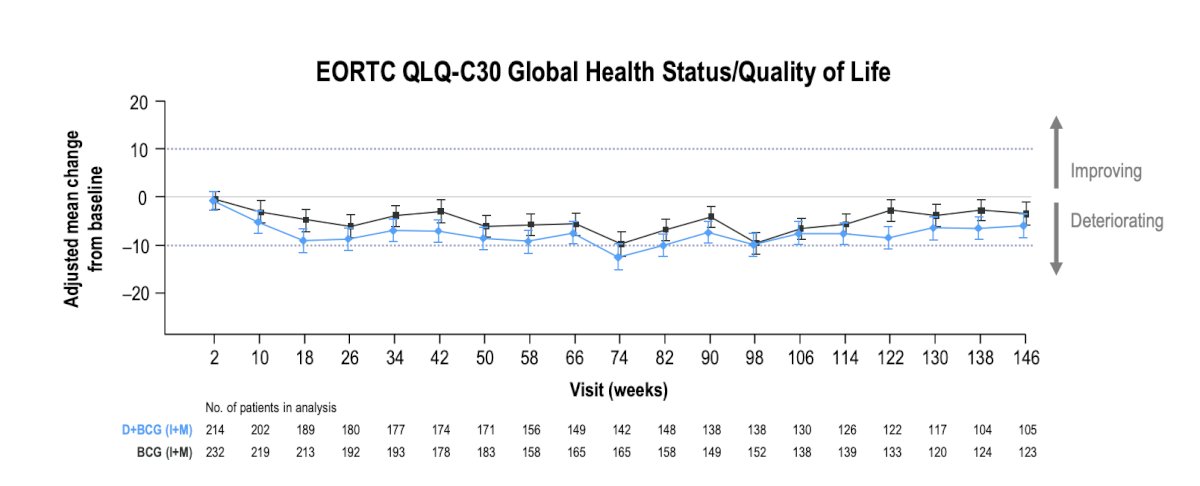
Adding durvalumab to BCG (induction + maintenance) therapy had no major impact on patient reported quality of life:
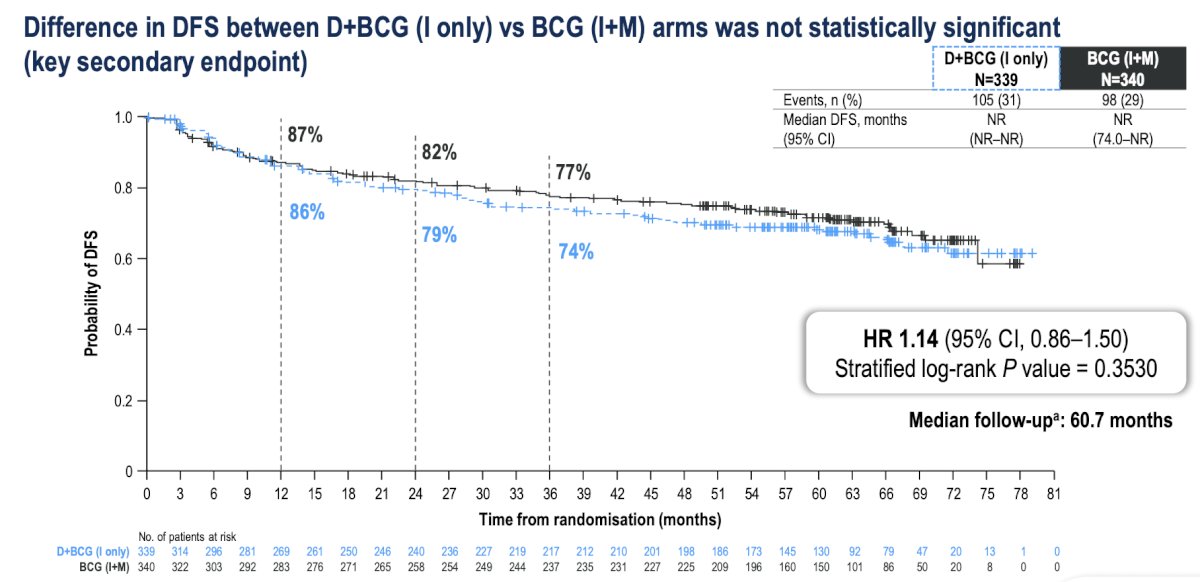
The secondary endpoint of disease free survival with durvalumab + BCG (induction only) versus BCG (induction + maintenance) was not statistically significant (HR 1.14, 95% CI 0.86–1.50):
Grade 3/4 treatment-related adverse events occurred in 21% of patients with durvalumab + BCG (induction + maintenance), in 15% with durvalumab + BCG (induction only), and in 4% with BCG (induction + maintenance). No treatment-related adverse events led to death:
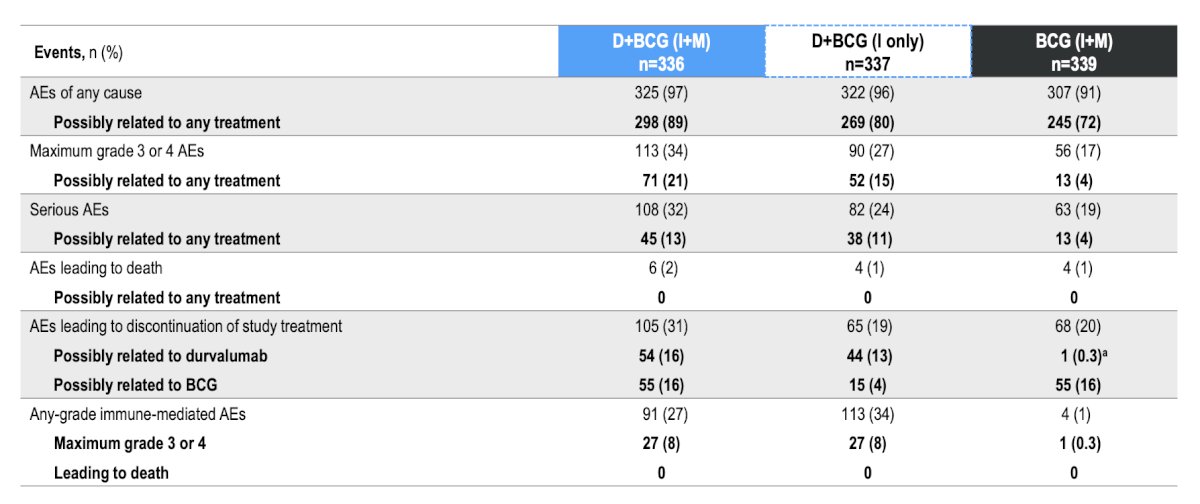
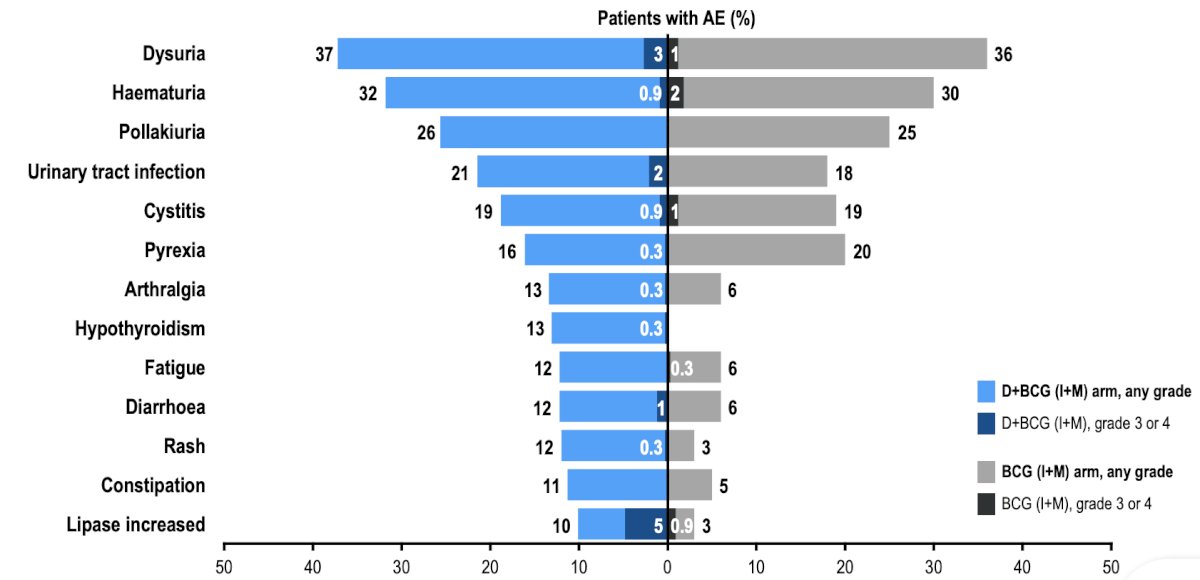
Overall, the safety profile was consistent with those of the individual therapies:
Dr. De Santis concluded her presentation discussing POTOMAC with the following take home points:
- Durvalumab in combination with BCG (induction + maintenance) resulted in a statistically significant and clinically meaningful improvement in disease free survival versus BCG (induction + maintenance) alone in patients with BCG-naive, high-risk non muscle invasive bladder cancer at a median of 5 years of follow-up
- 32% reduction in risk of a disease free survival event (HR 0.68; 95% CI, 0.50–0.93; p = 0.0154)
- Early and sustained disease free survival benefit with durvalumab (starting at <4 months)
- After a median follow-up of >5 years (14% maturity), a descriptive analysis showed an overall survival HR of 0.80 (95% CI, 0.53–1.20), demonstrating no detriment to overall survival with the addition of durvalumab
- Durvalumab + BCG (induction + maintenance) had a tolerable and manageable safety profile that was consistent with the known safety profiles of the individual agents, with no deaths due to treatment-related adverse events
- POTOMAC supports 1 year of durvalumab in combination with BCG induction and maintenance as a potential new treatment for patients with BCG-naive, high-risk non muscle invasive bladder cancer
The study was concomitantly published in The Lancet.
Presented by: Maria De Santis, MD, Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
Related Content:
Final Analysis of Phase 3 POTOMAC Study in High-Risk NMIBC - Maria De Santis
De Santis M, Palou Redorta J, Nishiyama H, et al; POTOMAC Investigators. Durvalumab in combination with BCG for BCG-naive, high-risk, non-muscle-invasive bladder cancer (POTOMAC): final analysis of a randomized, open-label, phase 3 trial. Lancet Oncol. Published online October 17, 2025. Online First
Durvalumab in Combination with BCG for BCG-naive, High-Risk, Non-Muscle-Invasive Bladder cancer (POTOMAC): Final Analysis of a Randomised, Open-Label, Phase 3 Trial.