(UroToday.com) The 2024 ESMO annual meeting included a session on expanding bladder preservation by optimal use of systemic therapy and biomarkers, featuring a presentation by Dr. Leslie Ballas discussing whether clinical responders have an option for chemoradiation. Dr. Ballas started by highlighting that based on the SWOG 8710 trial of neoadjuvant chemotherapy + cystectomy,1 we know that achieving a pT0 response leads to increased survival. Patients that received neoadjuvant chemotherapy had a pT0 rate of 38% versus 15% for pT0 among patients without neoadjuvant chemotherapy.
So, Dr. Ballas asks: Shouldn’t we do the same for trimodality therapy? Based on an ABC Meta-Analysis Collaboration systematic review published in The Lancet,2 we know that neoadjuvant chemotherapy improves survival regardless of local therapy: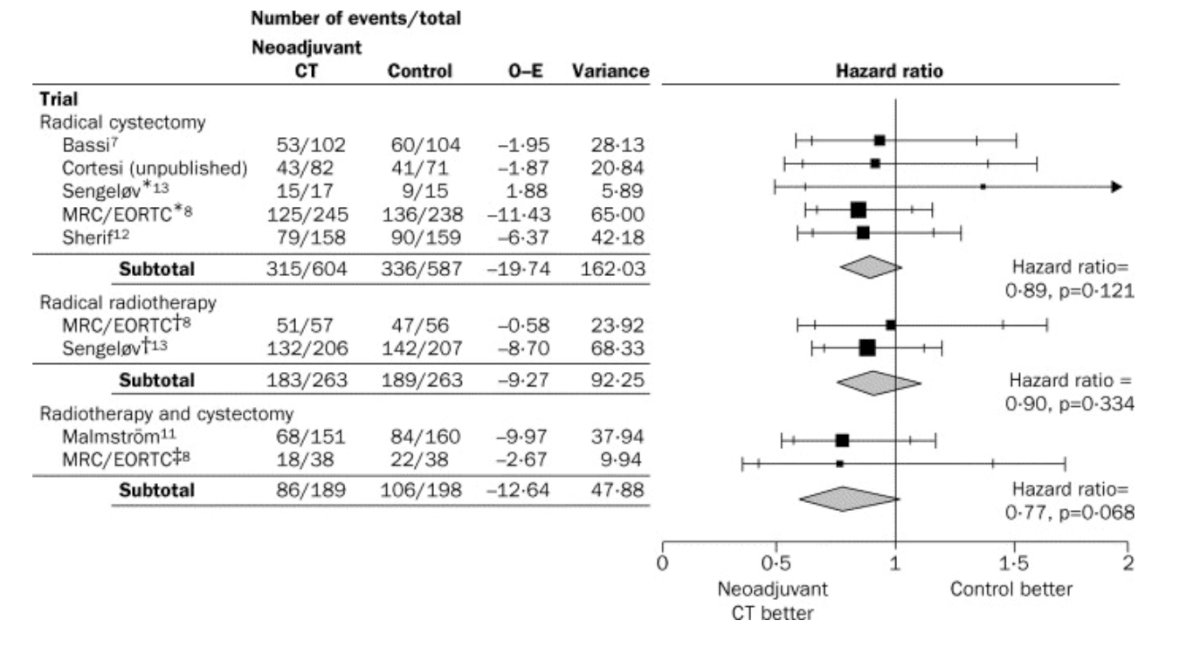
In 1998, Shipley et al. published results of the RTOG 89-03 trial,3 which randomized 123 T2-T4aNxM0 bladder cancer patients to two cycles of MCV chemotherapy before 39.6-Gy pelvic radiation with concurrent cisplatin 100 mg/m2 for two courses 3 weeks apart (arm 1) versus not receiving MCV chemotherapy before concurrent cisplatin and radiation therapy (arm 2). The actuarial 5-year overall survival rate was 49%: 48% in arm 1 and 49% in arm 2. Overall, 35% of the patients had evidence of distant metastases at 5 years: 33% in arm 1 and 39% in arm 2. Finally, the 5-year survival rate with a functioning bladder was 38%: 36% in arm 1 and 40% in arm 2.
The BA06 3084 trial assessed the use of neoadjuvant CMV chemotherapy in patients with muscle-invasive urothelial cancer of the bladder treated by cystectomy and/or radiotherapy.4 Overall, there was a CMV chemotherapy survival advantage of 5%, with 16% reduction in the risk of death (HR 0.84, 0.72-0.99) with a median follow-up of 8.0 years. Dr. Ballas notes that a subset analysis showed no difference between radiotherapy (n = 306) versus radical cystectomy (n = 422), specifically highlighting that this was radiotherapy alone and trimodality therapy: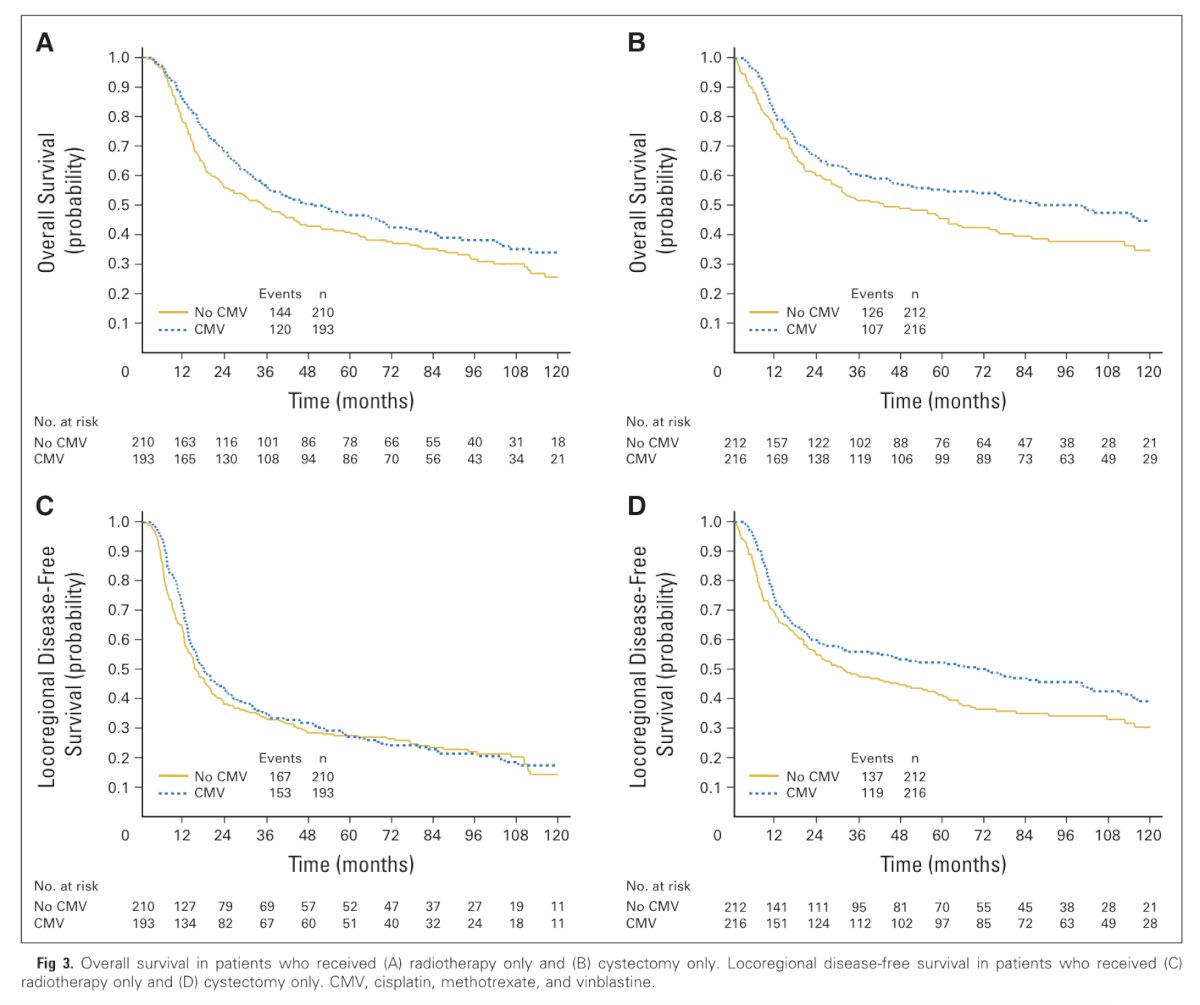
Dr. Ballas summarized neoadjuvant chemotherapy + trimodality therapy with the following:
- RTOG 89-03 showed no difference in survival between neoadjuvant chemotherapy and no neoadjuvant chemotherapy
- BA06 3084 trial of CMV versus no neoadjuvant CMV showed increased 10-year survival of 6%: CMV had a greater impact of locoregional disease-free survival in those that had a cystectomy versus those that received radiotherapy (no chemoradiotherapy)
- Pool analysis of the MGH data in which neoadjuvant chemotherapy was tested in a multivariable regression and had no effect on bladder intact disease-specific survival, cancer-specific survival, or overall survival (25% of patients treated with trimodality therapy received neoadjuvant chemotherapy)
- Pooled analysis of RTOG studies showed no benefit of neoadjuvant chemotherapy prior to trimodality therapy (32% of patients treated with trimodality therapy received neoadjuvant chemotherapy)
- Population-based analysis of the NCDB showed no difference in 5-year overall survival between neoadjuvant chemotherapy and no neoadjuvant chemotherapy (different chemotherapy regimens and radiotherapy regimens were not accounted for)
Dr. Ballas then discussed a neoadjuvant chemotherapy + trimodality therapy multi-institutional study from Jiang et al. assessing outcomes in 57 patients from 2008-2017.5 Most patients completed planned neoadjuvant chemotherapy (95%), all patients completed external-beam radiotherapy, and 84% completed at least 60% of the planned concurrent weekly cisplatin doses. The median overall survival was not reached, and the 2-year overall survival rates and disease-specific survival rates were 74% (95% CI 57.7-84.9) and 88% (95% CI 78.5-98.1), respectively. The two-year bladder-intact disease-free survival was 64%, and salvage cystectomy was performed in 14% of patients. Distant relapse occurred in 11%, and 9% died of metastatic disease.
Arguably, the best data outside of a randomized clinical trial comes from a high-level propensity-matched score-matched multi-institutional (Toronto, MGH, USC) study assessing radical cystectomy versus trimodality therapy in highly selected patients.6 This retrospective analysis included 703 patients with muscle-invasive bladder cancer clinical stage T2-T3/4aN0M0. Specifically, there were 421 radical cystectomy patients and 282 trimodality therapy patients who would have been eligible for both trimodality therapy and radical cystectomy (2005-2017). To compare homogeneous cohorts, all patients included in this analysis had solitary tumors <7 cm, no unilateral hydronephrosis, and no extensive carcinoma in situ. Treatment propensity scores were estimated using logistic regression, and patients were matched 3:1 with replacement and a caliper of 0.25. Covariates included age, sex, clinical T stage (cT2 vs cT3-4), hydronephrosis, (neo)adjuvant chemotherapy, body mass index, smoking history, and ECOG status. Neoadjuvant or adjuvant chemotherapy (n = 159) did not affect 5-year metastasis-free survival for patients treated by trimodality therapy (80%, 95% CI 73-87), with neoadjuvant or adjuvant chemotherapy versus without (73%, 95% CI 65-81; (p = 0.14):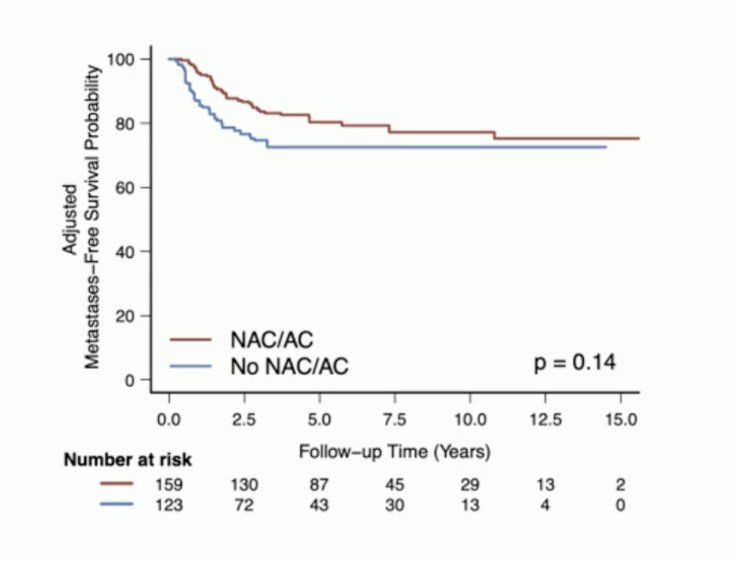
Kool et al. performed a multi-center analysis of 10 Canadian centers to assess the effect of neoadjuvant chemotherapy on patients with muscle-invasive bladder cancer treated with curative-intent radiotherapy in a real-world setting. Among 785 patients with muscle-invasive bladder cancer treated with radiotherapy, 586 patients were included in the analysis, of which 102 (17%) received neoadjuvant chemotherapy before radiotherapy.7 In this population of patients undergoing radiotherapy, neoadjuvant chemotherapy was significantly associated with improved cancer-specific survival (HR 0.28, 95% CI 0.14-0.56; p < 0.001) and overall survival (HR 0.56, 95% CI 0.38-0.84; p = 0.005):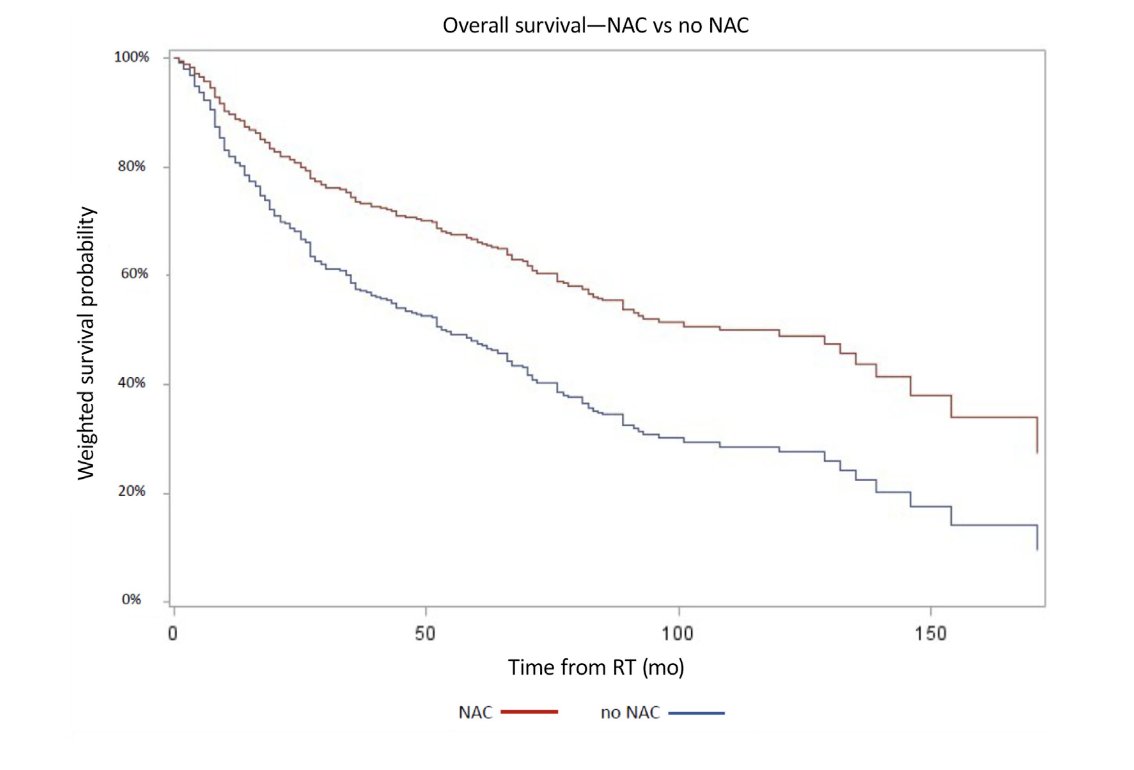
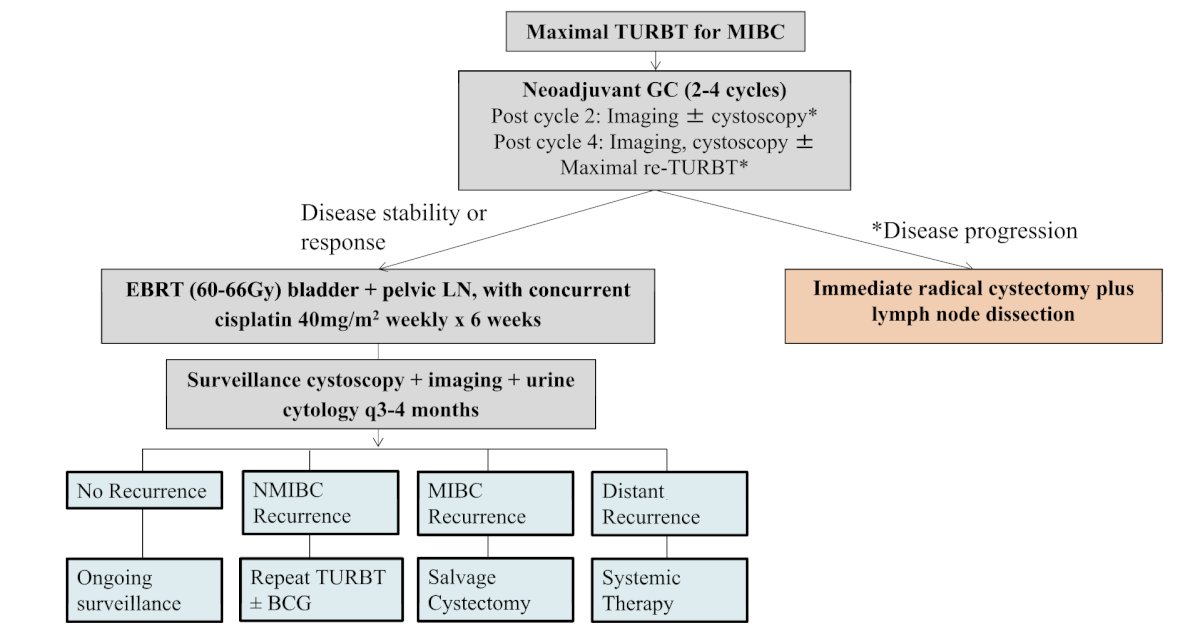
Jiang and colleagues have proposed the following response-adapted therapy algorithm for trimodal therapy with neoadjuvant chemotherapy:5
To highlight next steps, Dr. Ballas notes that a treatment algorithm needs to take into account other forms of neoadjuvant therapy (ie. neoadjuvant chemotherapy + IO, enfortumab vedotin + pembrolizumab), how best to assess clinical response/post-treatment clinical stage, and take into account hypofractionated radiotherapy regimens: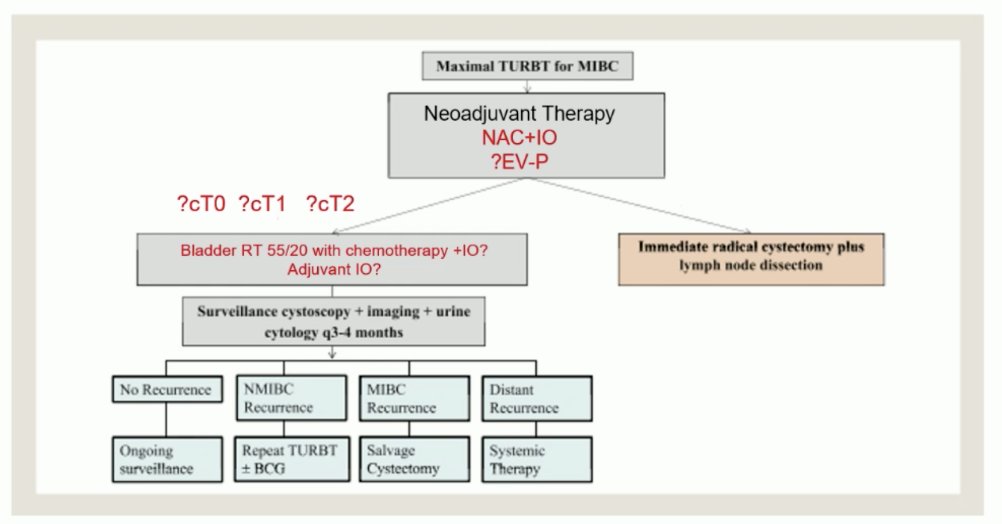
Dr. Ballas concluded her presentation discussing whether clinical responders have an option for chemoradiation with the following take-home points:
- There is interest in neoadjuvant chemotherapy prior to trimodality therapy, but there are many unanswered questions
- Perhaps response-based treatment will be the new therapy paradigm
Presented by: Leslie Ballas, MD, Director, Hematologic/Bone Marrow Transplant/Cellular Therapies Disease Research Group, Cedars Sinai Medical Center, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 European Society of Medical Oncology (ESMO) Annual Meeting, Barcelona, Spain, Fri, Sept 13 – Tues, Sept 17, 2024.
References:
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 2003;349(9):859-866.
- ABC Meta-Analysis Collaboration. Neoadjuvant chemotherapy in invasive bladder cancer: A systematic review and meta-analysis. Lancet. 2003 Jun 7;361(9373): 1927-1934.
- Shipley WU, Winter KA, Kaufman DS, et al. Phase III trial of neoadjuvant chemotherapy in patients with invasive bladder cancer treated with selective bladder preservation by combined radiation therapy and chemotherapy: initial results of Radiation Therapy Oncology Group 89-03. J Clin Oncol. 1998 Nov;16(11):3576-3583.
- Griffiths G, Hall R, Sylvester R, et al. International phase III trial assessing neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: long term results of the BA06 30894 trial. J Clin Oncol 2011;29(16):2171-2177.
- Jiang DM, Jiang H, Chung PWM, et al. Neoadjuvant chemotherapy before bladder-sparing chemoradiotherapy in patients with nonmetastatic muscle-invasive bladder cancer. Clin Genitourin Cancer. 2019 Feb;17(1):38-45.
- Zlotta AR, Ballas LK, Niemierko A, et al. Radical cystectomy versus trimodality therapy for muscle-invasive bladder cancer: A multi-institutional propensity score matched and weighted analysis. Lancet Oncol. 2023 Jun;24(6):669-681.
- Kool R, Dragomir A, Kulkarni GS, et al. Benefit of neoadjuvant cisplatin-based chemotherapy for invasive bladder cancer patients treated with radiation-based therapy in a real-world setting: An inverse probability treatment weighted analysis. Eur Urol Oncol. 2024 Feb 6;S2588-9311(24)00040-3.