(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured an advancements in upper tract urothelial carcinoma session and a presentation by Dr. Jiwei Huang discussing DISTINCT-I, a phase 2 trial assessing perioperative disitamab vedotin and tislelizumab followed by nephron-sparing surgery in high-risk upper tract urothelial carcinoma.
Radical nephroureterectomy is the standard treatment for localized high-risk upper tract urothelial carcinoma. However, functional nephron preservation has become a clinical priority to improve long-term outcomes. This phase II trial (DISTINCT-I) evaluated a kidney-sparing approach combining endoscopic Thulium laser ablation or ureteral segmental resection with perioperative HER2-targeted therapy (disitamab vedotin) and immune checkpoint inhibitors in high-risk upper tract urothelial carcinoma.
DISTINCT-I is a prospective, multicenter, phase II trial (NCT05912816) enrolling patients with high-risk upper tract urothelial carcinoma (T1-3N0–1, M0), which included patients with absolute or relative indications for renal preservation and those with normal renal function who actively chose a kidney-preserving strategy. The protocol included endoscopic biopsy followed by 2–4 cycles of induction therapy with disitamab vedotin (2.0 mg/kg) plus tislelizumab (200 mg) every 3 weeks, followed by kidney-sparing surgery. The primary endpoint was 1-year kidney-intact event-free survival (events: high-risk local recurrence, metastasis, death). Secondary endpoints included clinical complete response, renal function preservation, and safety.
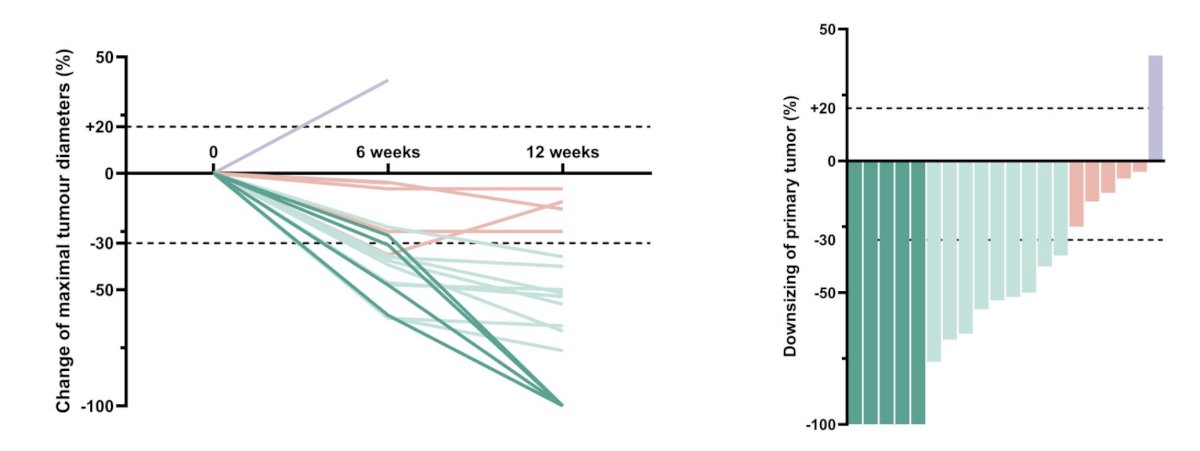
Among 20 enrolled patients (median follow-up: 16 months), HER2 status by immunohistochemistry (IHC) was: 3+ (n = 6), 2+ (n = 3), 1+ (n = 7), 0 (n = 4). Tumor responses were complete response (n = 5), partial response (n = 9), stable disease (n = 5), and progressive disease (n = 1). The following figure highlights radiographic treatment response to neoadjuvant therapy:
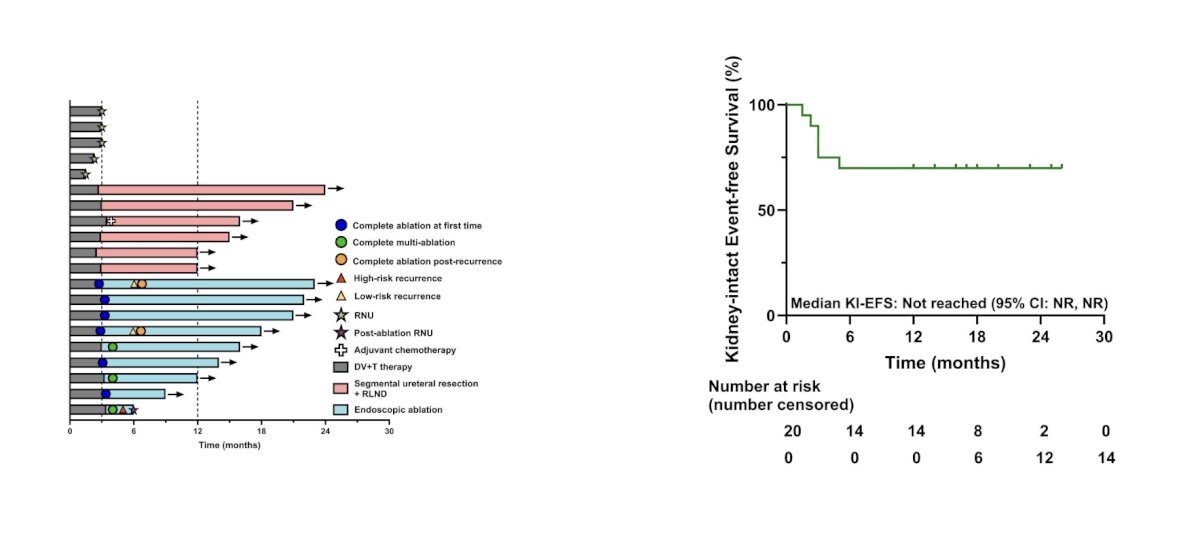
Kidney-sparing procedures included ureteral segmental resection (n = 6) and endoscopic ablation (n = 9), with 5 patients undergoing radical nephroureterectomy. One recurrence after ablation required salvage radical nephroureterectomy at 6 months. The 1-year kidney intact event-free survival was 70% (14/20), and the clinical complete response rate was 25.0% (5/20) after completion of induction therapy (3-month assessment), which increased to 75.0% (15/20) after the subsequent kidney-sparing surgical procedures (4-month assessment):
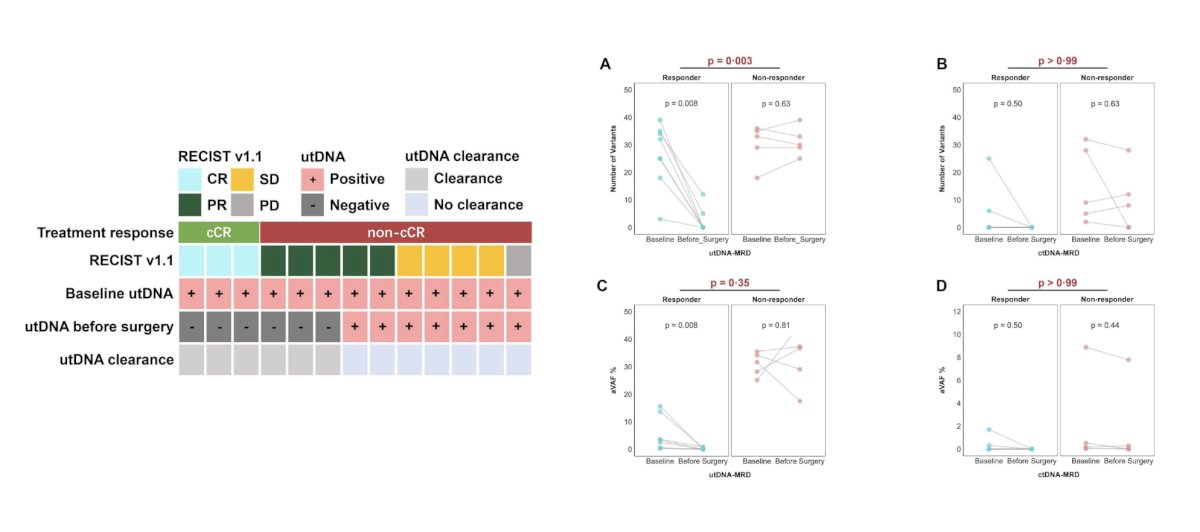
Seventeen patients (85%) completed all 4 planned cycles of induction therapy. Objective response rates correlated strongly with HER2 IHC expression: IHC 3+ (objective response rate 100%), 2+ (objective response rate 66.7%), 1+ (objective response rate 57.1%), and 0 (objective response rate 50.0%). Grade ≥3 systemic toxicities occurred in 10% of patients. Urinary tract DNA (utDNA) levels decreased significantly in responders (complete response/partial response) compared to non-responders (p < 0.05):
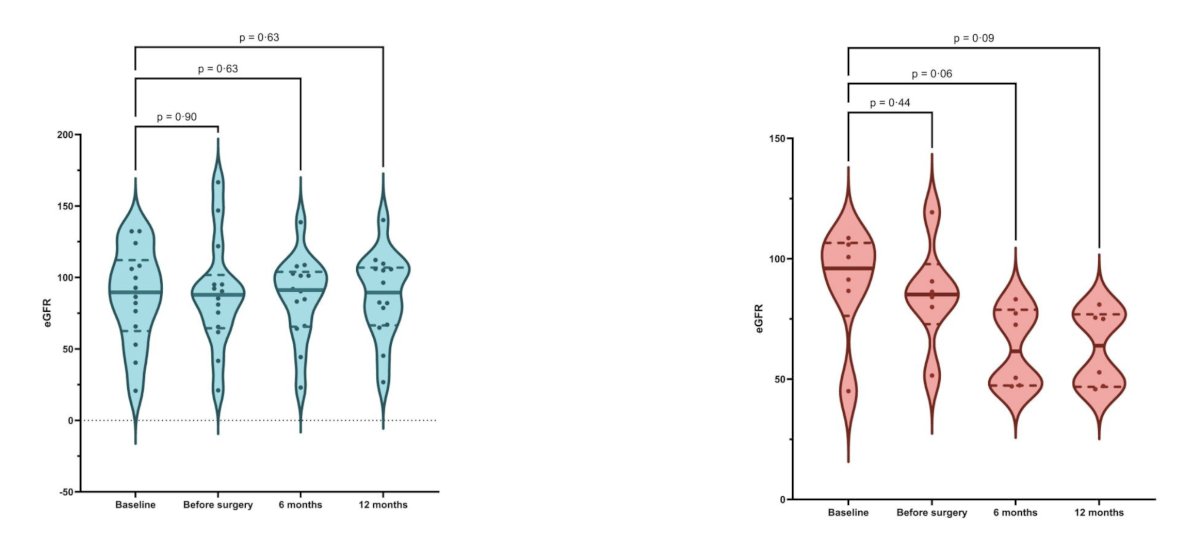
At 1 year, the kidney-sparing group (n= 14) exhibited a median improvement in eGFR from baseline (+3.6%), contrasting with a median decline of 29.8% in the radical nephroureterectomy group (n = 5):
Dr. Huang concluded this presentation discussing DISTINCT-I with the following take-home points:
- The combination of disitamab vedotin and immune checkpoint inhibitors with kidney-sparing surgery demonstrates promising tumor downstaging and nephron preservation in high-risk upper tract urothelial carcinoma, with a favorable safety profile
- HER2 overexpression may predict enhanced response, supporting further biomarker validation
- This organ-preservation paradigm challenges the historical dominance of radical nephroureterectomy and represents a promising therapeutic strategy for selected patients with high-risk upper tract urothelial carcinoma
Presented by: Jiwei Huang, Professor, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.