(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a session exploring the frontier of upper tract urothelial carcinoma and a presentation by Dr. Gu Liangyou discussing the efficacy and safety of disitamab vedotin combined with tislelizumab as adjuvant therapy after radical surgery for patients with HER2-expression upper tract urothelial carcinoma.
Upper tract urothelial carcinoma is a relatively rare yet highly aggressive malignancy, and despite definitive treatment with radical nephroureterectomy, the prognosis remains poor. Adjuvant chemotherapy, the current standard of care, provides limited benefit due to postoperative renal function issues. HER2 is an important biomarker for urothelial carcinoma, with an expression rate of HER2 (IHC 1+/2+/3+) as high as 80%. Of note, the higher the expression of HER2 in urothelial carcinoma, the worse the prognosis.
In the RC48-C016 study, disitamab vedotin combined with immune checkpoint inhibitors led to a significantly greater improvement in outcomes than chemotherapy among patients with untreated HER2-expressing locally advanced or metastatic urothelial cancer.1 This phase II study evaluated the efficacy and safety of adjuvant therapy combining disitamab vedotin with tislelizumab in patients with HER2-expression upper tract urothelial carcinoma.
In this prospective phaseⅡtrial, patients with high-risk, non-metastatic, and HER2-expressing upper tract urothelial carcinoma were enrolled. The experimental group received disitamab vedotin (2 mg/kg IV every 3 weeks) + tislelizumab (200 mg IV every 3 weeks) for 6 cycles during the induction phase, followed by 11 cycles of tislelizumab (200 mg IV every 3 weeks) maintenance therapy. The control group received 4 cycles of gemcitabine at a dose of 1,000mg/m2 on days 1 and 8 plus cisplatin at a dose of 70mg/m2 on day 1 of each 3-week cycle. The primary endpoint was disease-free survival, and secondary endpoints included overall survival and safety profile:

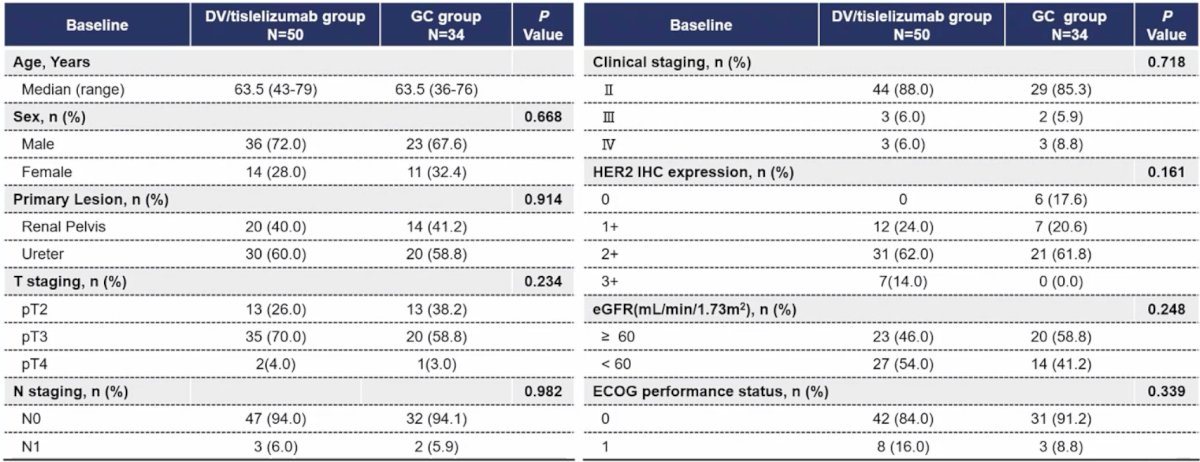
Between July 2023 and July 2025, 84 patients were enrolled to receive the disitamab vedotin + tislelizumab (n = 50) or chemotherapy (n = 34). In the chemotherapy group, 20 patients received cisplatin treatment, while 14 patients received carboplatin treatment. In the experimental group, 26% (13/50), 70% (35/50), 4% (2/50) patients were pT2, pT3, and pT4, respectively, and 6% (3/50) patients were N+. Among them, 38 (76.0%) had HER2 high expression (IHC 2+ or 3+), and 12 of them had HER2 low expression (IHC 1+). In the control group, 38.2% (13/34), 58.8% (20/34), 3.0% (1/34) patients were pT2, pT3, and pT4, respectively, and 5.9% (2/34) patients were N+. The baseline data were similar between the two groups:
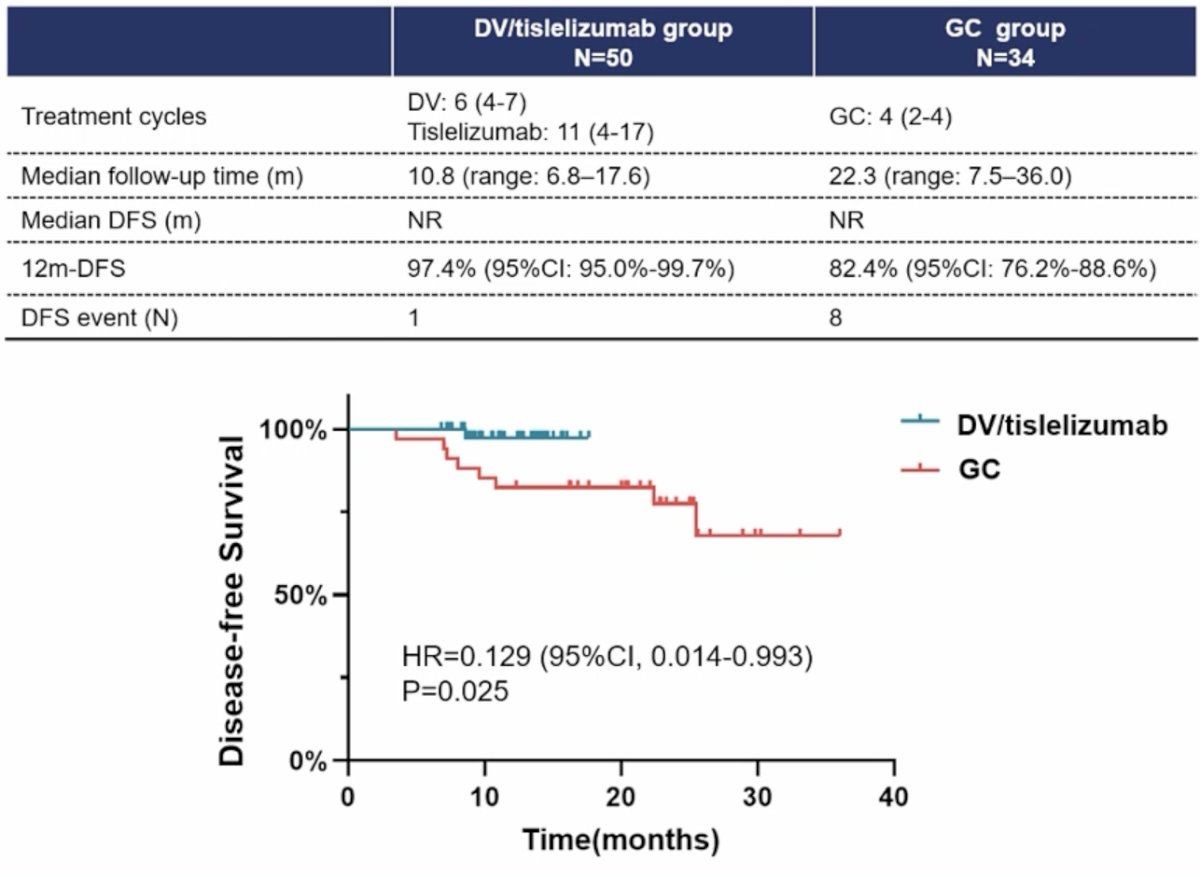
At the data cutoff of February 4, 2026, the median treatment cycles received for disitamab vedotin were 6 (range: 4-7), for tislelizumab were 11 (range: 4-17), and for chemotherapy were 4 (range: 2-4). The median follow-up in the disitamab vedotin + tislelizumab group was 10.8 months (range: 6.8-17.6), and for the chemotherapy group was 22.3 months (range: 7.5-36.0). During follow-up, 1 and 8 patients had recurrence or metastasis, respectively. The median disease-free survival was not reached in either the disitamab vedotin + tislelizumab group or the chemotherapy group (HR 0.129, 95% CI 0.014-0.993; p = 0.025). The 12-month disease-free survival rate was 97.4% (95% CI 95.0%-99.7%) for the disitamab vedotin + tislelizumab group and 82.4% (95% CI 76.2%-88.6%) for the chemotherapy group:
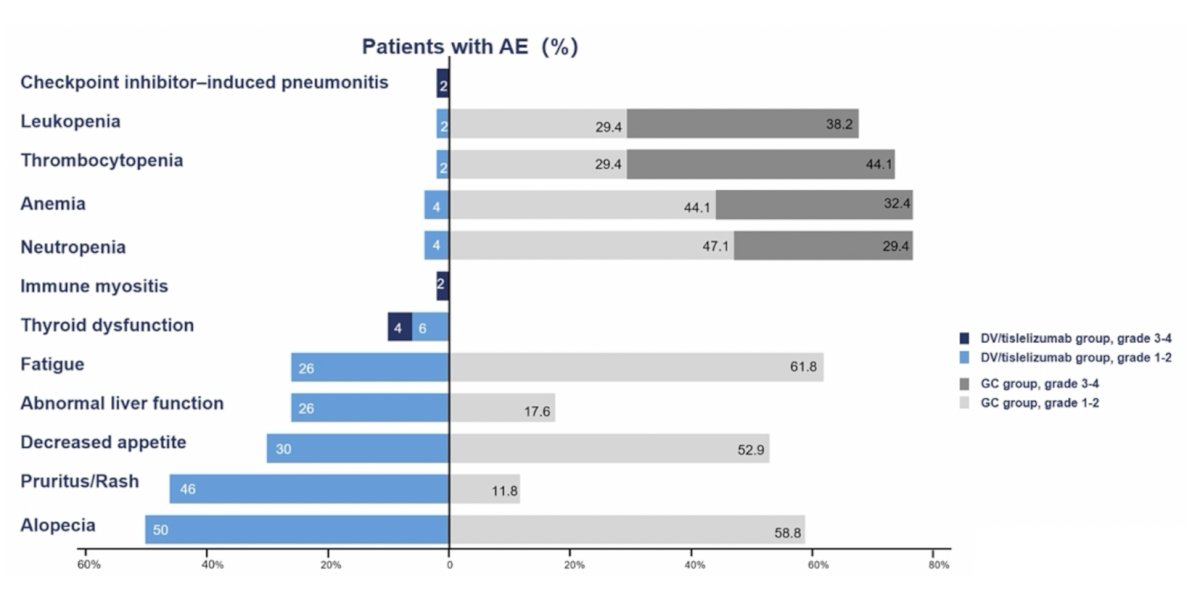
In the disitamab vedotin + tislelizumab group, treatment-related adverse events occurred in 92% (46/50) of patients, predominantly grade 1-2. The most common treatment-related adverse events included alopecia (n = 25, 50%) and rash (n = 22, 44.0%), with 2 grade 3 treatment-related adverse events: immune-mediated myositis (n = 1, 2%) and hyperthyroidism (n = 1, 2%). In the chemotherapy group, treatment-related adverse events occurred in 97.1% (33/34) of patients, with 47% (16/34) of grade 3-4. The most common treatment-related adverse events included anemia (n = 26, 76.5%) and decreased neutrophil count (n = 26, 76.5%). Grade 3-4 included thrombocytopenia (n = 15, 44.1%) and leukopenia (n = 13, 38.2%). There were no treatment-related deaths observed:
Dr. Liangyou concluded his presentation discussing the efficacy and safety of disitamab vedotin combined with tislelizumab as adjuvant therapy after radical surgery for patients with HER2-expression upper tract urothelial carcinoma with the following take-home points:
- The disitamab vedotin + tislelizumab combination demonstrated promising preliminary efficacy and a manageable safety profile as adjuvant therapy in patients with HER2-expression upper tract urothelial carcinoma
- These findings warrant validation through a phase 3 randomized controlled trial
Presented by: Gu Liangyou, Chinese PLA General Hospital, Beijing, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Reference:
- Sheng X, Zeng G, Zhang C, et al. Disitamab Vedotin plus Toripalimab in HER2-Expressing Advanced Urothelial Cancer. N Engl J Med. 2025 Dec 11;393(23):2324-2337.