(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a session exploring the frontier of upper tract urothelial carcinoma and a presentation by Dr. Jiwei Huang discussing CURATE-UTUC, a multicenter prospective longitudinal cohort study assessing ctDNA and utDNA dynamics for predicting minimal residual disease and recurrence risk in locally advanced upper tract urothelial carcinoma.
Locally advanced upper tract urothelial carcinoma (≥ pT2 or N+) exhibits high recurrence rates despite adjuvant therapy. Current biomarkers lack sufficient accuracy for risk-adapted management. The CURATE-UTUC study evaluated longitudinal ctDNA and utDNA dynamics for molecular residual disease detection and recurrence risk stratification.
This multicenter prospective cohort enrolled 84 patients with pT2-4/N+ M0 upper tract urothelial carcinoma from two Chinese referral centers (2022–2025). Patients underwent radical nephroureterectomy, initiated guideline-recommended adjuvant therapy (chemotherapy/immunotherapy) within 12 weeks, and provided serial plasma/urine samples preoperatively (T0), at 1 month postoperatively (T1), post-cycle 2 of adjuvant therapy (T2), end-of-treatment (T3), and quarterly/semi-annually until recurrence or 24 months (T4-T6). Tumor-informed molecular residual disease assays used whole-exome sequencing of surgical specimens. The primary endpoint was radiologically confirmed extravesical recurrence-free survival.
At a median 19.0-month follow-up (range 5.0–41.0), 46.4% (39/84) of patients developed recurrence (29 extravesical, 10 intravesical). Liquid biopsy detected molecular residual disease at a median lead time of 95.0 days (IQR 53.0–214.0) before clinical recurrence. T1 ctDNA positivity predicted an 8.7-fold higher extravesical recurrence risk (HR 8.7, 95% CI 3.7–20.6; p < 0.001):
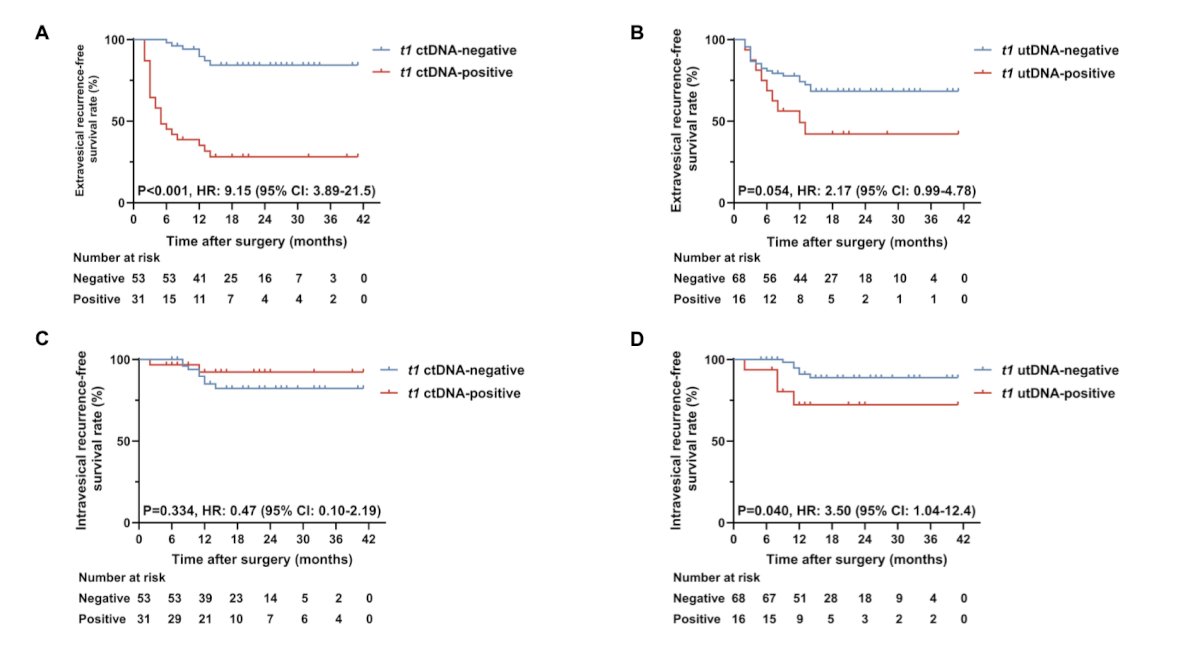
This escalated to 31.7-fold at T2 (HR 31.7, 9.5–106.1; p < 0.001), while T2 utDNA positivity predicted intravesical recurrence (HR 14.5, 3.7–56.5; p < 0.001). Site-specific recurrence associations and dynamic monitoring of ctDNA and utDNA are shown in the following figure:
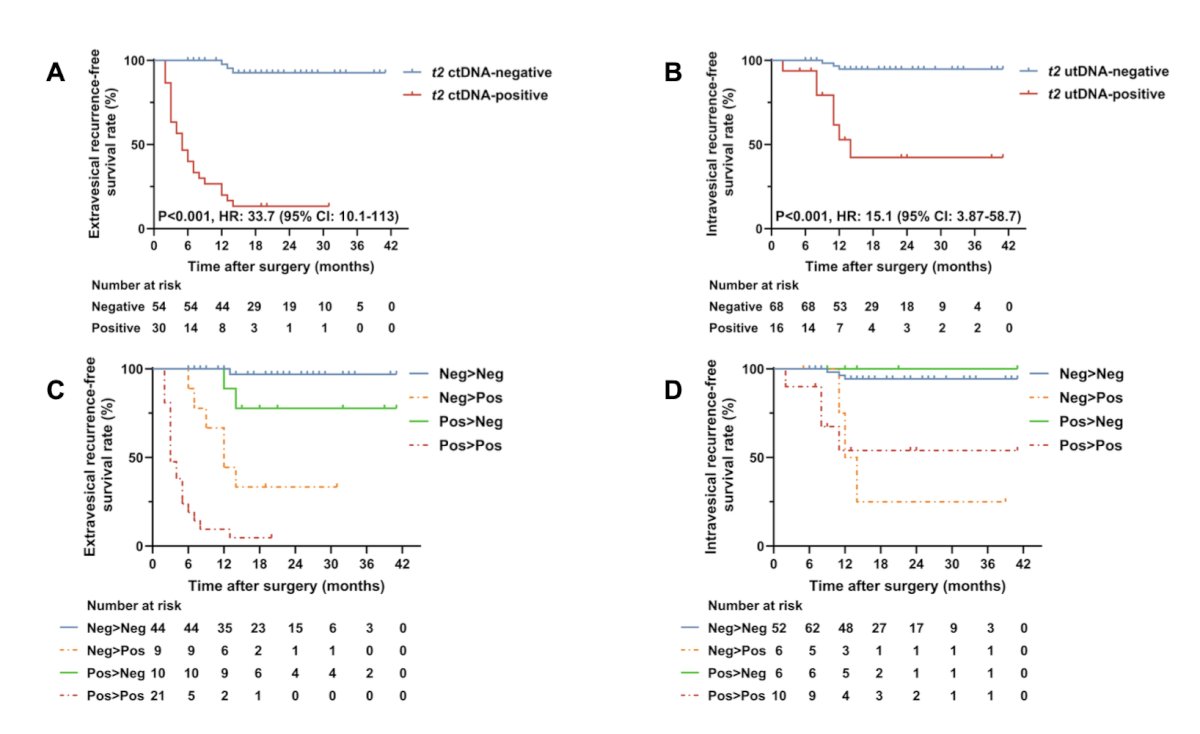
Multivariable analysis confirmed T1 ctDNA+ (HR 11.5, 95% CI 3.8–35.2), T2 ctDNA+ (HR 38.7, 95% CI 9.9–151.6), and pT3–4 stage (HR 8.7, 95% CI 2.1–35.7; all p ≤ 0.003) as independent predictors of extravesical recurrence, with T2 utDNA+ solely predicting intravesical recurrence (HR 14.5, p < 0.001). Biomarker performance remained robust regardless of adjuvant therapy (all p < 0.001). Finally, baseline mutational landscape and concordance across tumor tissue, plasma ctDNA, and urine utDNA in the CURATE-UTUC cohort are shown in the following figure:

Dr. Huang concluded this presentation discussing CURATE-UTUC with the following take-home points:
- Longitudinal ctDNA and utDNA monitoring enables early molecular residual disease detection and refined risk stratification in locally advanced upper tract urothelial carcinoma, identifying molecular relapse months before clinical progression
- This dual-liquid biopsy strategy holds promise for defining a critical window for therapeutic intervention and merits further investigation in prospective, interventional trials to validate its potential for guiding personalized adjuvant therapy strategies
Presented by: Jiwei Huang, MD, PhD, Professor, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.