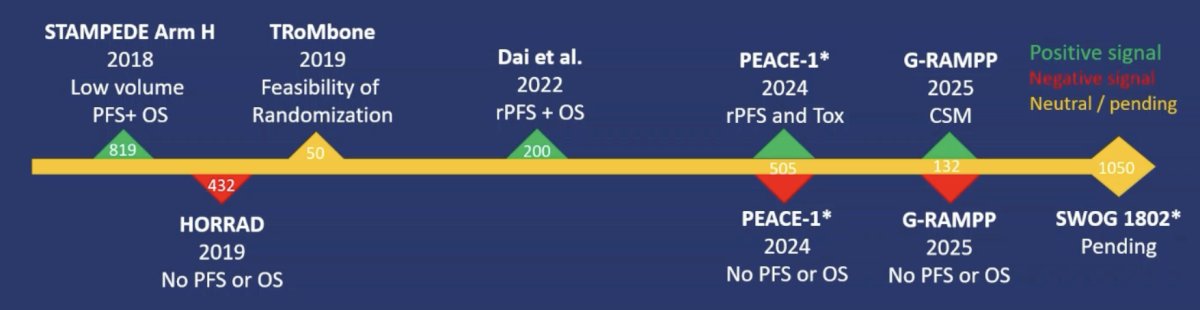
(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a game changer session and a presentation by Dr. Brian Chapin discussing results from a phase II, randomized, controlled trial of best systemic therapy versus best systemic therapy + definitive treatment of the primary tumor in metastatic prostate cancer. Local therapy in men with de novo metastatic (M1) prostate cancer is evolving and somewhat conflicting based on the current randomized clinical trials:
The aim of this study was to evaluate the effect of local therapy on the primary tumor on progression free survival in men with M1 prostate cancer.
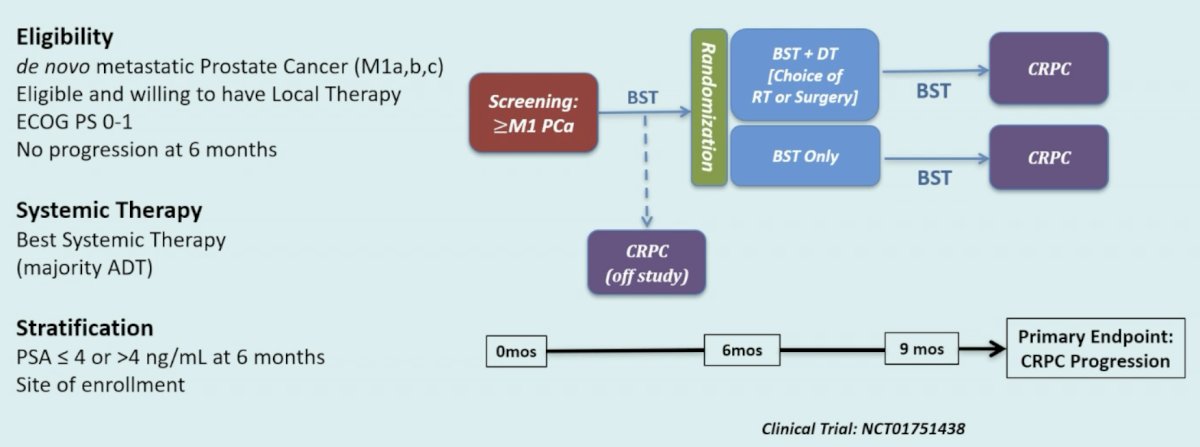
In a multi-center, randomized phase II trial, men with M1 prostate cancer, after receiving 6-months of best systemic therapy, were randomly assigned (1:1) to continue best systemic therapy alone or best systemic therapy with the addition of either radiotherapy or surgery to their primary tumor. The primary endpoint, progression free survival, was defined as the time from randomization to progression by PSA, radiographic or symptomatic progression, or per physician discretion and/or clinical decision to change systemic therapy, or death, whichever occurred first:
Secondary endpoints included overall survival, safety and toxicity, quality of life (EPIC), and biomarker evaluation (aggressive variant prostate cancer, p53, PTEN, Rb). Immunohistochemistry (IHC) for p53, RB1, and PTEN was performed on available prostate biopsies at baseline and at 6-months, and the aggressive variant prostate cancer molecular signature was assigned if ≥ 2 of these were abnormal. The study was designed with a Bayesian interim monitoring plan, with progression free survival for each arm assumed to follow an exponential distribution. After 60 patients, if the probability of one arm being better than the other is greater than 97.5%, the trial will be stopped early. In the current intent to treat analysis, Kaplan Meier product-limit method was used to estimate the median progression free survival.
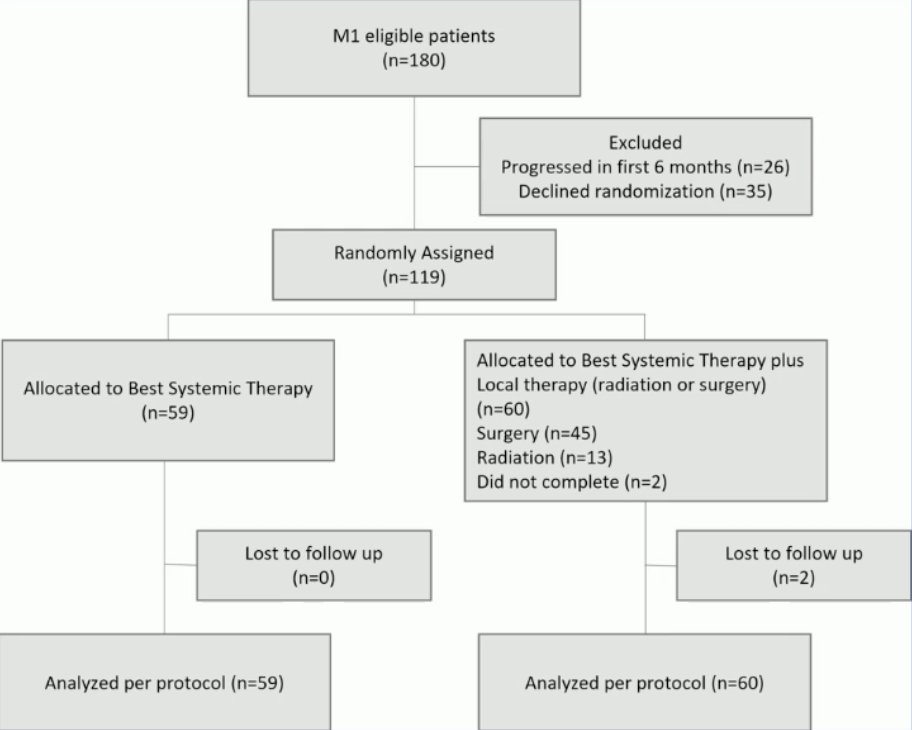
From March 2013 to April 2018, 119 patients were randomized (best systemic therapy: 59, best systemic therapy + local therapy: 60), with the following consort diagram:
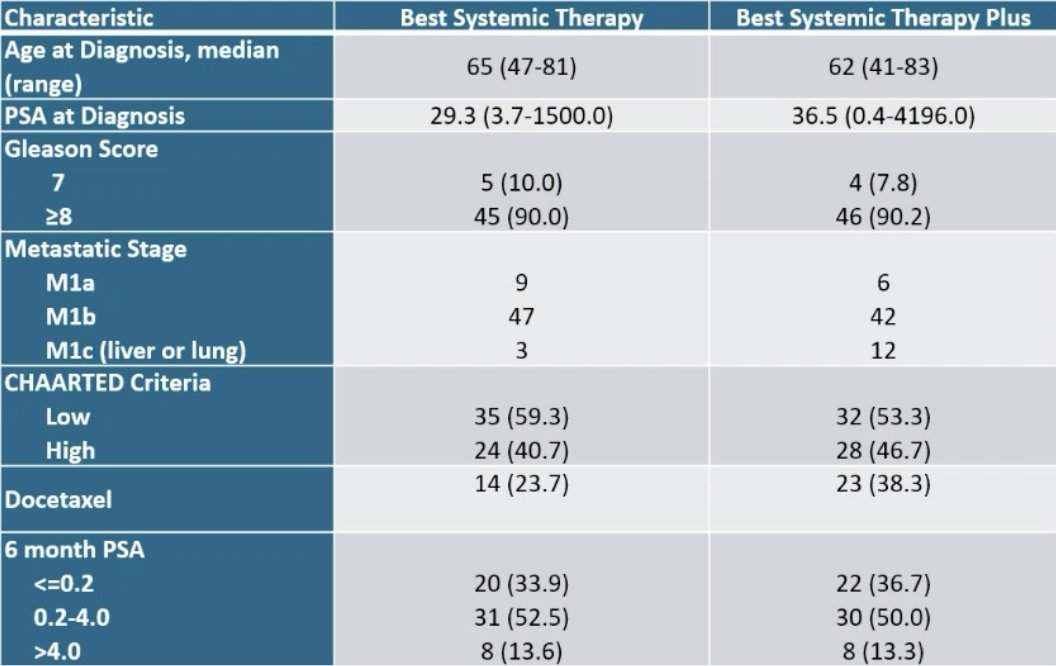
The median age for patients undergoing best systemic therapy was 65 years (range: 47-81) and 62 years (range: 41-83) for best systemic therapy + local therapy. The median PSA was higher in the best systemic therapy + local therapy group (36.5 versus 29.3 ng/mL):
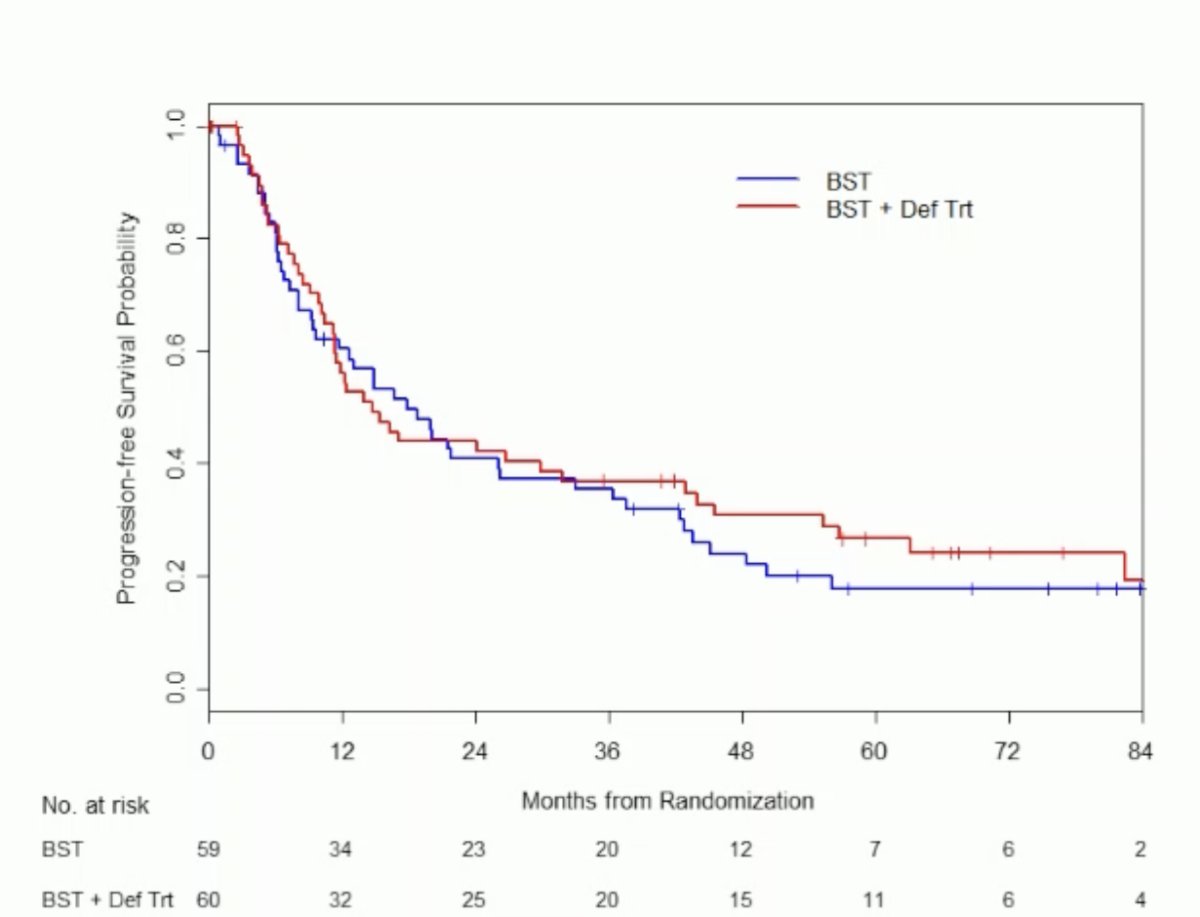
The median follow-up for patients who survived was 66 months. Best systemic therapy included ADT (n = 119), with docetaxel (n = 37) or with androgen receptor pathway inhibitor agents (n = 9). Local therapy included surgery (n = 45), radiation (n = 13), or none (n = 2). At data analysis, 88 patients met PCGW2 progression, and 53 patients had died. The median progression free survival was 17 months (95% CI 11.7-36.4) for patients undergoing best systemic therapy and 14.8 months (95% CI 11.4-42.9) for patients undergoing best systemic therapy + local therapy (HR 0.89, 95% CI 0.59-1.34; p = 0.57).
The median overall survival was 74.4 months (95% CI 66.4-NE) for patients undergoing best systemic therapy and 80 months (95% CI 55.8-NE) for patients undergoing best systemic therapy + local therapy (HR 1.07, 95% CI 0.62-1.83; p = 0.82):

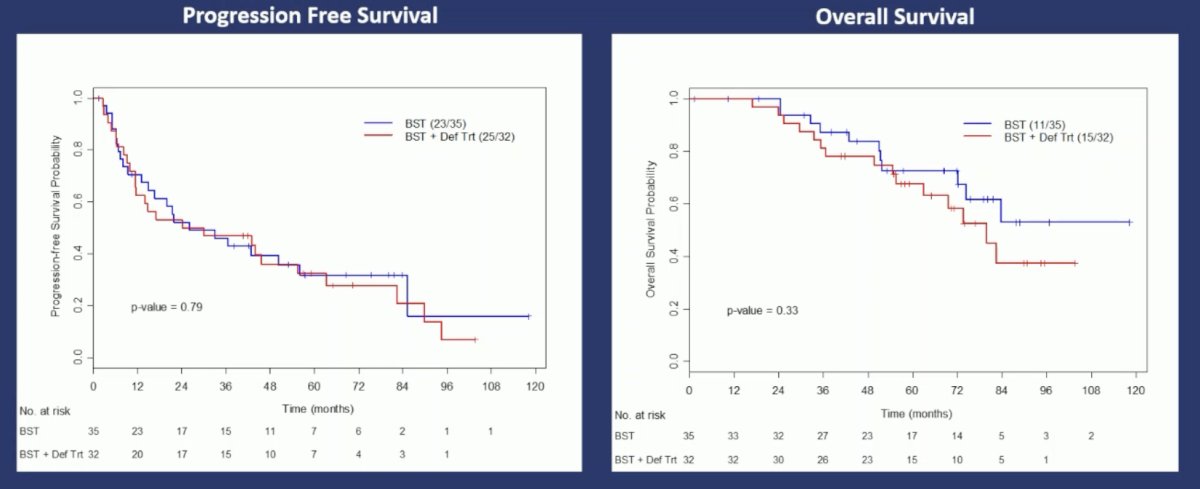
In the low volume cohort, there was no difference between the groups with regards to progression free survival (p = 0.79) and overall survival (p = 0.33):
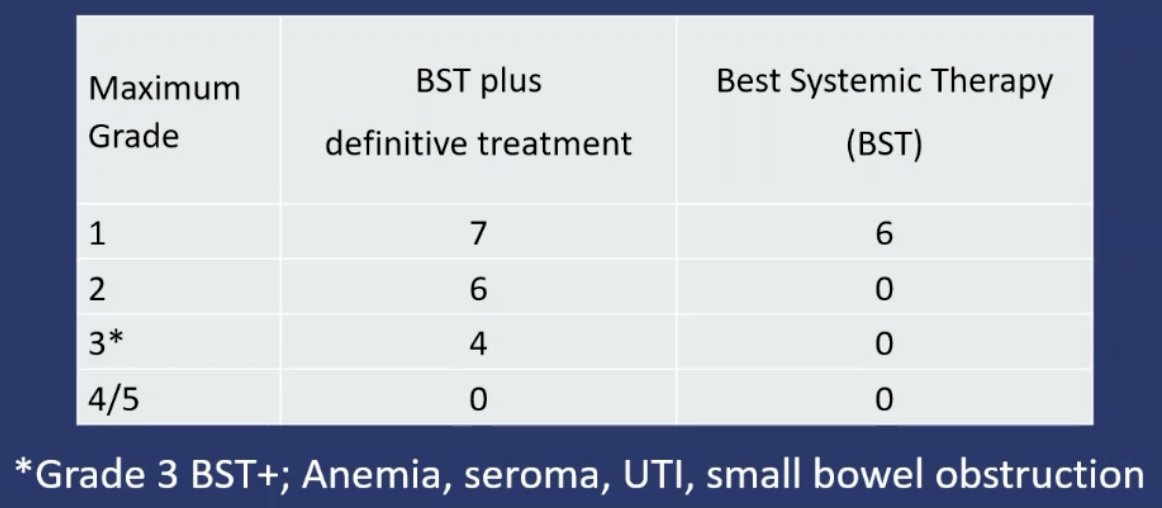
Toxicity was limited in both arms with Grade 3 toxicities in 4 patients (6.7%) for patients undergoing best systemic therapy + local therapy and 0 patients undergoing best systemic therapy:
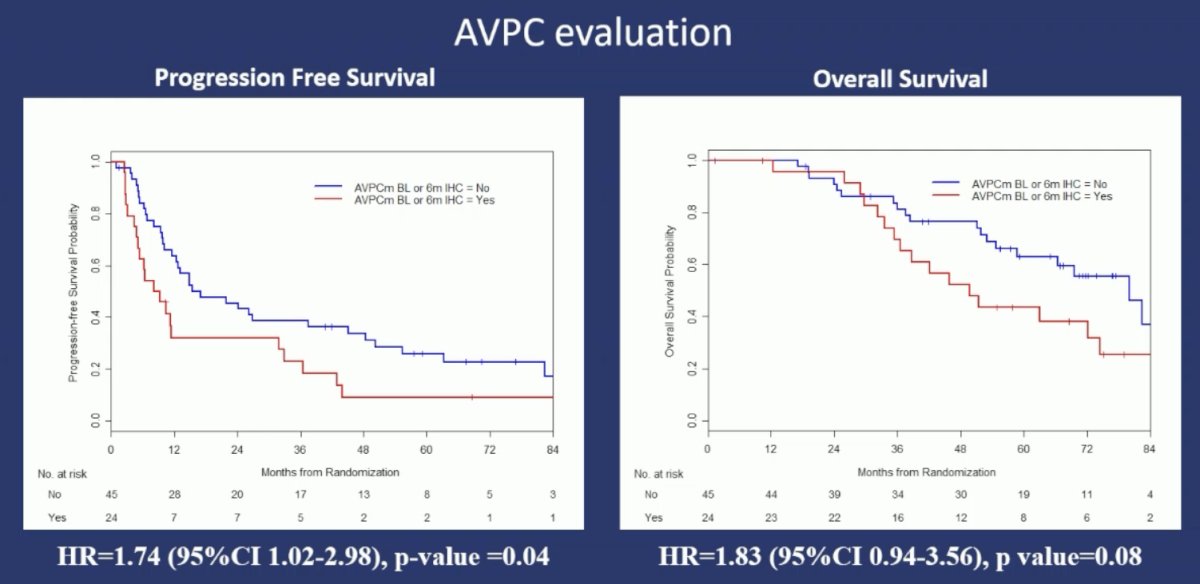
Three patients required palliative intervention for symptomatic local progression receiving best systemic therapy, while an additional 6 patients crossed over to receive local therapy after meeting CRPC progression. Having the aggressive variant prostate cancer molecular profile at baseline or 6 months was significantly associated with a worse progression free survival (HR 1.74, 95% CI 1.02-2.98; p-value = 0.04). However, there was no statistically significant association with overall survival (HR 1.83; 95% CI 0.94-3.56; p value = 0.08):
Dr. Chapin concluded his presentation discussing results from a phase II, randomized, controlled trial of best systemic therapy versus best systemic therapy with definitive treatment of the primary tumor in metastatic prostate cancer, with the following take-home points:
- This trial demonstrated feasibility and safety of randomizing men with de novo M1 prostate cancer treated with best systemic therapy, to the addition of surgery or radiation to their primary tumor
- There was no benefit in progression free survival or overall survival with the addition of local therapy, although this was underpowered
- This trial identified the aggressive variant prostate cancer signature as a potential biomarker of prognostic value in the metastatic population
- SWOG 1802 is still actively accruing
Presented by: Brian Chapin, MD, MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.