(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a game changer session and a discussant presentation by Dr. Jochen Walz discussing “PRIMARY2 – Impact of 68Ga-PSMA-11 PET/CT in the diagnosis of prostate cancer in men with equivocal or non-suspicious findings on mpMRI: A multi-center, phase III, randomized trial.” The current EAU guidelines recommend performing an MRI before prostate biopsy in men with suspected organ confined disease (Strength: Strong), with the following additional recommendations:
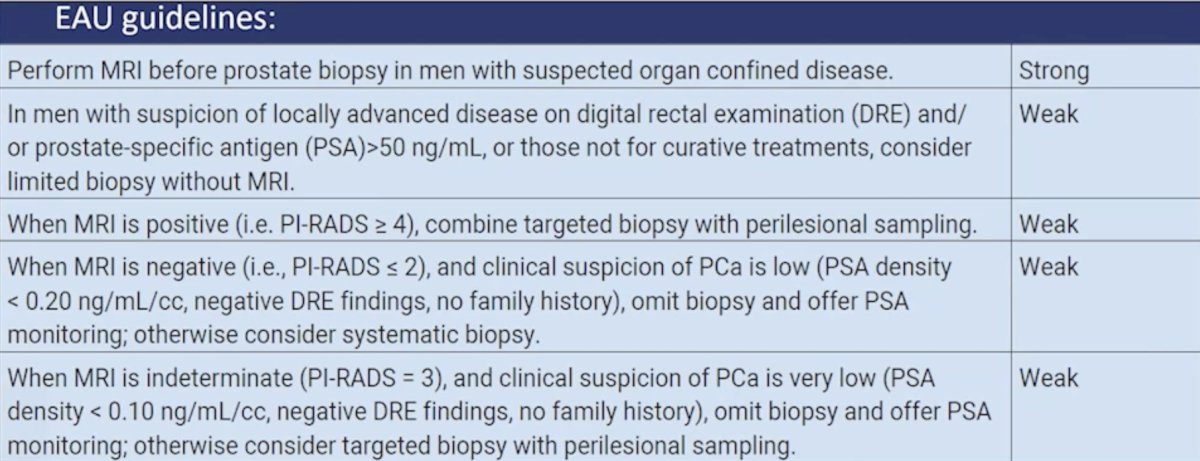
Notably, the guidelines mention that when an MRI is negative (ie. PI-RADS <=2), and clinical suspicion of prostate cancer is low (PSA density < 0.20 ng/mL, negative DRE findings, no family history), we may omit biopsy and offer PSA monitoring; otherwise consider systematic biopsy (Strength: Weak). In the setting of an indeterminate (PI-RADS 3) MRI lesions and clinical suspicion of prostate cancer is very low (PSA density < 0.10 ng/mL, negative DRE findings, no family history), we may omit biopsy and offer PSA monitoring; otherwise consider targeted biopsy with perilesional sampling (Strength: Weak).
PRIMARY2 focuses on these PI-RADS 3 challenging patients. We know that these patients are common based on rates of 29% in the PROMIS trial,1 24% in MRI-FIRST,2 and 20% in the PRECISION trial.3 Dr. Walz notes that there are several strengths of the PRIMARY2 trial:
- Appropriate design: phase 3, non-inferiority
- Early detection cohort (based on age, PSA, PSA density, etc)
- Biopsy naïve men: provides the clearest signal about diagnostic performance
- Appropriate reference: systematic biopsy with 12 cores (mean 25 cores)
- Use of a standardized risk stratification system – the PRIMARY score
The use of the PRIMARY score in PRIMARY2 improves standardization and reproducibility, with a high Cohen’s kappa (k = 0.81) between local versus central reading. This is notably higher than for mpMRI, with recent series ranging from k = 0.34 to k = 0.64. PRIMARY2 also has relevant co-primary endpoints, including the detection of clinically significant prostate cancer (Gleason score 3+4, >10%) and the number of biopsies avoided. PRIMARY2 found that PSMA PET +/- biopsy (12% clinically significant prostate cancer) was non-inferior to systematic biopsy (16% clinically significant prostate cancer), and that 49% of biopsies could be avoided in the PSMA PET arm. This trial also had a relevant secondary endpoint of the diagnosis of clinically insignificant prostate cancer, which was 32% in the control arm versus 14% in the PSMA PET arm.
Dr. Walz also highlighted several limitations of the PRIMARY2 trial. Is a 10% non inferiority margin for clinically significant prostate cancer acceptable? In the trial, there was a low rate of clinically significant prostate cancer (12% in the PSMA PET arm versus 16% in the control arm) in this PI-RADS 2-3 patient cohort, with a very low rate of highly significant prostate cancer (ISUP 4-5 = 2%; ISUP 3 = 4-5%), which confirms the favorable negative predictive value of MRI. Is this potentially an expensive pathway justified in view of such a low “miss rate” with MRI?
PSMA PET remains an important resource and is a major benefit in the initial staging of prostate cancer, assessing biochemical recurrence, documenting metastatic disease, and who may be a candidate for radioligand therapy. However, PSMA PET is expensive, with the following prices for a PSMA PET scan in the following countries:
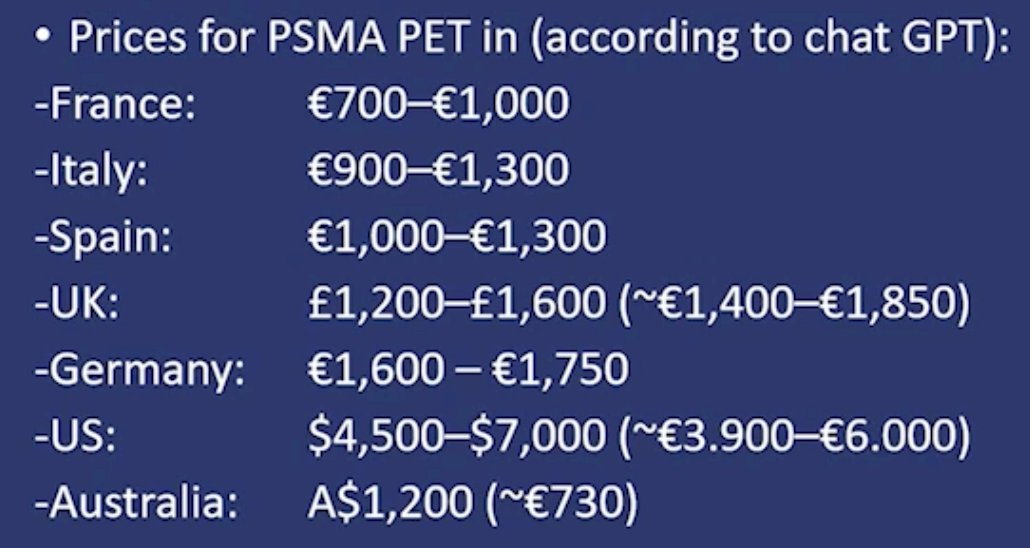
Thus, there is a need for a detailed cost effectiveness analysis taking all aspects into account, not only the upfront costs, but also the “follow-up” costs.
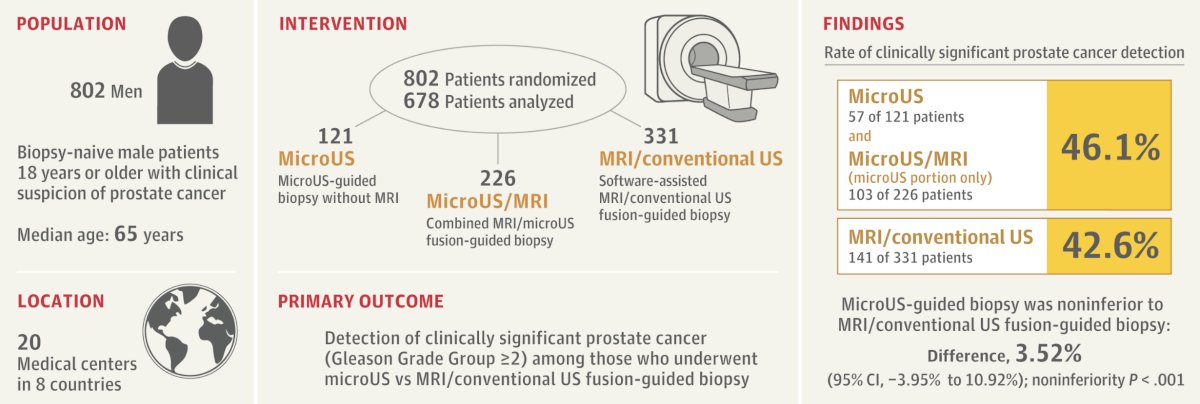
Are there alternatives to PSMA PET? In 2025, the OPTIMUM trial was published,4 a randomized trial assessing micro-ultrasonography versus MRI-guided biopsy for prostate cancer diagnosis. This was a multicenter, international, open-label, randomized noninferiority trial of biopsy-naive men from 20 centers (678 men underwent biopsy). The primary endpoint was the detection of grade group 2 or higher cancers using micro-ultrasonography + systematic biopsy versus MRI + conventional ultrasonography + systematic biopsy, with a non-inferiority margin set at 10%. This trial found that grade group 2 or higher cancer was detected in 47.1% of micro-ultrasonography group, 42.6% in the MRI + conventional ultrasound group, and 46.9% in the experimental group. Ultimately, micro-ultrasonography guided biopsy was noninferior to MRI fusion biopsy with a difference of 3.52% (p < 0.001):
Dr. Walz concluded his presentation discussing the PRIMARY2 phase 3 trial by emphasizing that the addition of Ga-PSMA-11 PET/CT to MRI in these men halves the number of men requiring a prostate biopsy without compromising the detection of clinically significant cancer. But can we afford it?
Presented by: Jochen Walz, MD, Institut Paoli-Calmettes Cancer Centre, Marseille, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017;389(10071):815-822.
- Rouviere O, Renard-Penna R, Claudon M, et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naïve patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol 2019 Jan;20(1):100-109.
- Kasivisvanathan V, Rannikko AS, Borghi M, et al. MRI-targeted or standard biopsy for prostate cancer diagnosis. N Engl J Med 2018;378(19):1767-1777.
- Kinnaird A, Luger F, Cash H, et al. Microultrasonography-Guided vs MRI-Guided Biopsy for Prostate Cancer Diagnosis: The OPTIMUM Randomized Clinical Trial. JAMA. 2025 May 20;333(19):1679-1687.