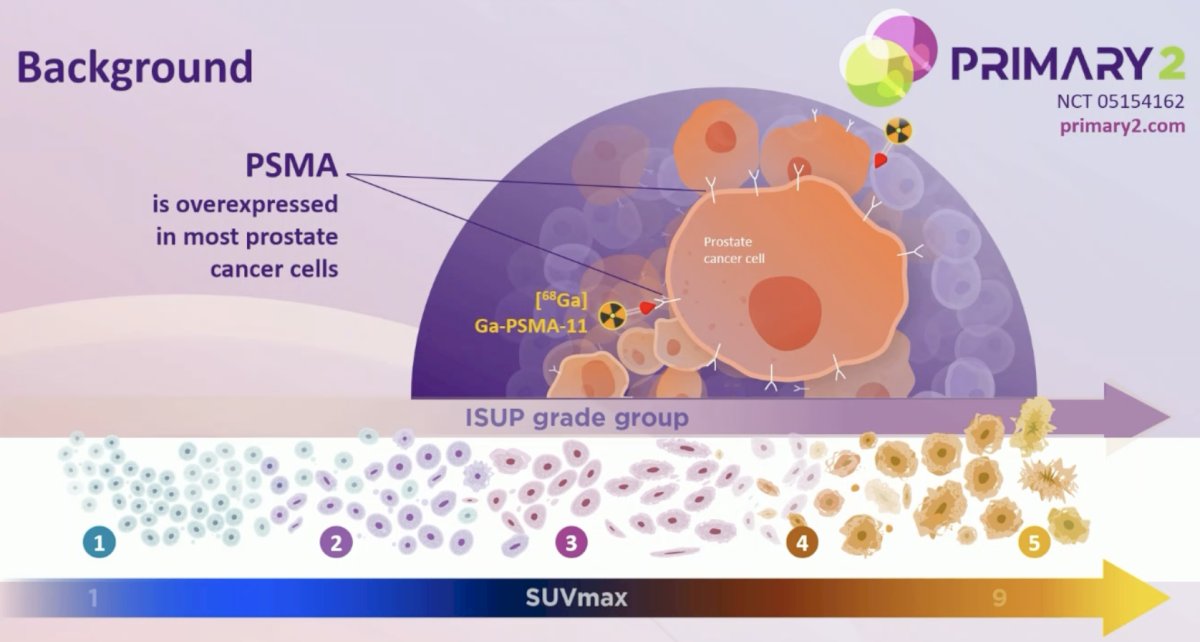
(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a game changer session and a presentation by Dr. James Buteau discussing results from the PRIMARY2 phase 3 trial assessing the impact of 68Ga-PSMA-11 PET/CT in the diagnosis of prostate cancer in men with equivocal or non-suspicious findings on mpMRI. Across guidelines, multi-parametric MRI is recommended for men with clinical suspicion of significant prostate cancer. Those with PIRADS 2 or 3 lesions often undergo prostate biopsy for high clinical suspicion, but have a low likelihood of significant prostate cancer on biopsy, and high likelihood of insignificant prostate cancer. Previously, the PRIMARY trial demonstrated that 68Ga-PSMA-11 PET/CT pre-biopsy improved negative predictive value for significant prostate cancer compared to MRI alone:1
At EAU 2026, Dr. Buteau and colleagues aimed to demonstrate that 68Ga-PSMA-11 PET/CT could reduce patients requiring biopsy and limit biopsy to targeted cores, without significantly decreasing significant prostate cancer diagnosis.
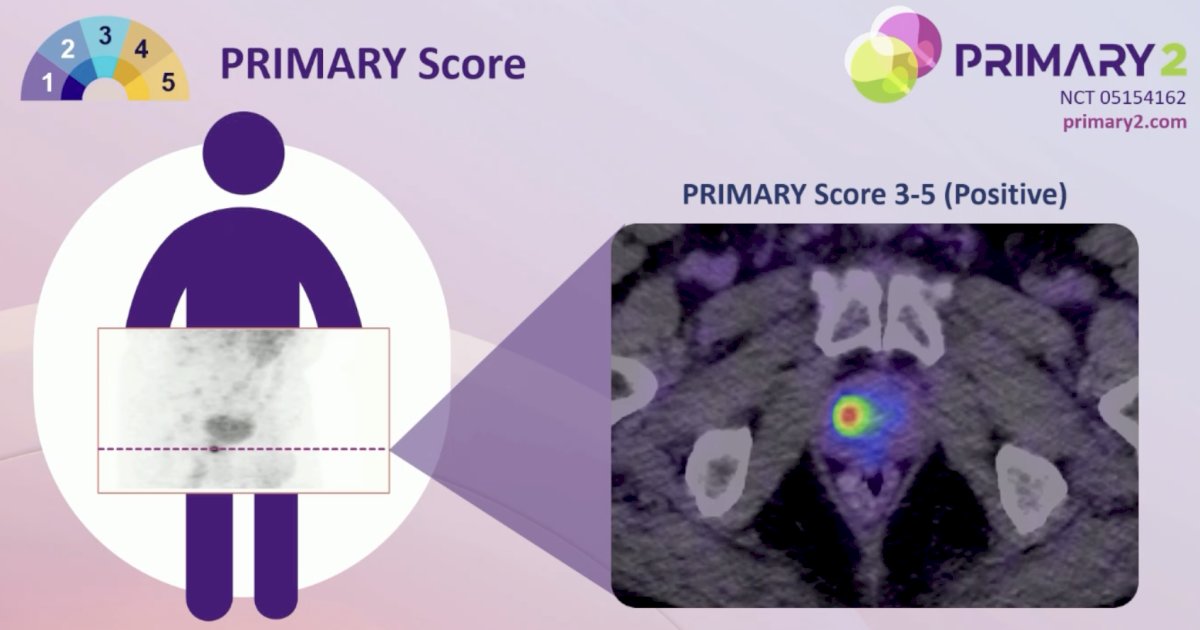
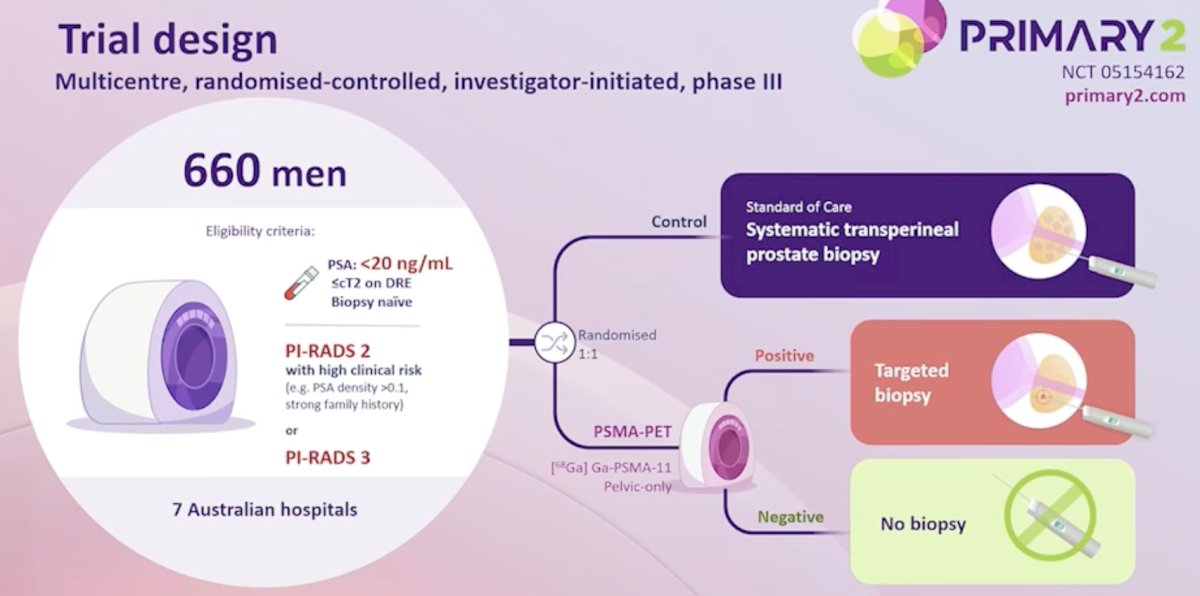
This investigator-initiated, multicenter (7 Australian sites), randomized controlled, phase III trial enrolled biopsy-naive participants with clinical suspicion of significant prostate cancer, PI-RADS 3 or PI-RADS 2 on MRI with risk factors (ie. PSA density >0.1, strong family history), PSA ≤20 ng/mL, and ≤cT2. Participants were randomized (1:1) and stratified by center. In the control arm, participants were assigned to undergo systematic transperineal prostate biopsies. In the experimental arm, participants were assigned to pelvic 68Ga-PSMA-11 PET/CT, interpreted by local and central reviewers independently. Participants with PRIMARY score 3-5 (positive) had targeted transperineal prostate biopsies, while those with PRIMARY score 1-2 (negative) had PSA monitoring without biopsy:
Significant prostate cancer was defined as Gleason score 3+4 (≥10% pattern 4) = 7 or higher on transperineal prostate biopsy. Avoidance of prostate biopsy was measured at 6 months from randomization:
The primary endpoints were analyzed with intention to treat. A one-sided test with type I error of 2.5% was used to determine whether (i) the proportion of participants with significant prostate cancer in the experimental arm was non-inferior to the control arm at a non-inferiority margin of 10% and (ii) biopsy was avoided in >20% of participants in the experimental arm.
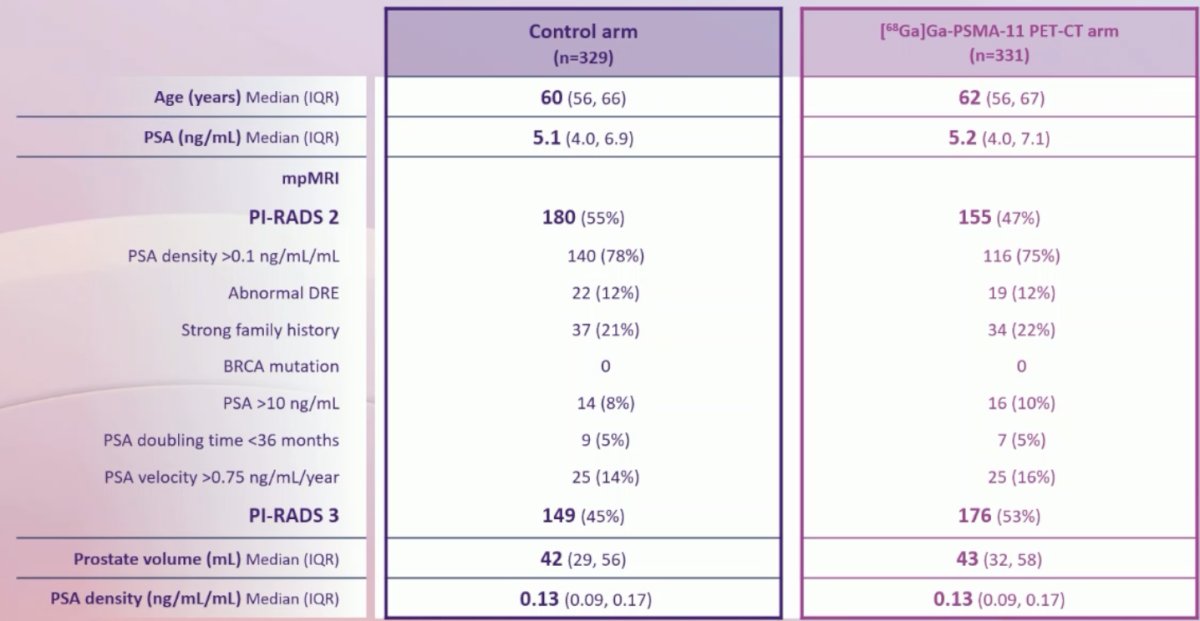
Between March 2, 2022, and August 24, 2025, 660 eligible participants had a median age of 61 years (IQR 56 - 66), median PSA 5.2 ng/mL (IQR 4.0 - 7.0), with PI-RADS 2 in 335 (51%) and 3 in 325 (49%) on MRI:
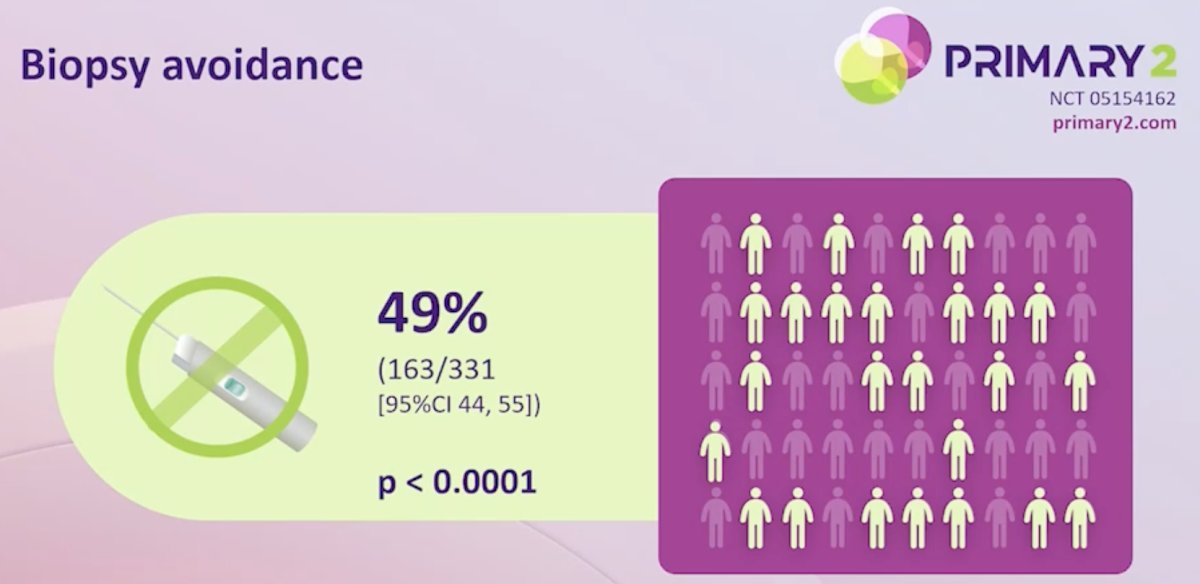
In the control arm, significant prostate cancer was diagnosed in 51/329 (16%). In the 68Ga-PSMA-11 PET/CT arm, prostate biopsy was avoided in 163/331 (49% [95% CI 44, 55%]; p < 0.001):
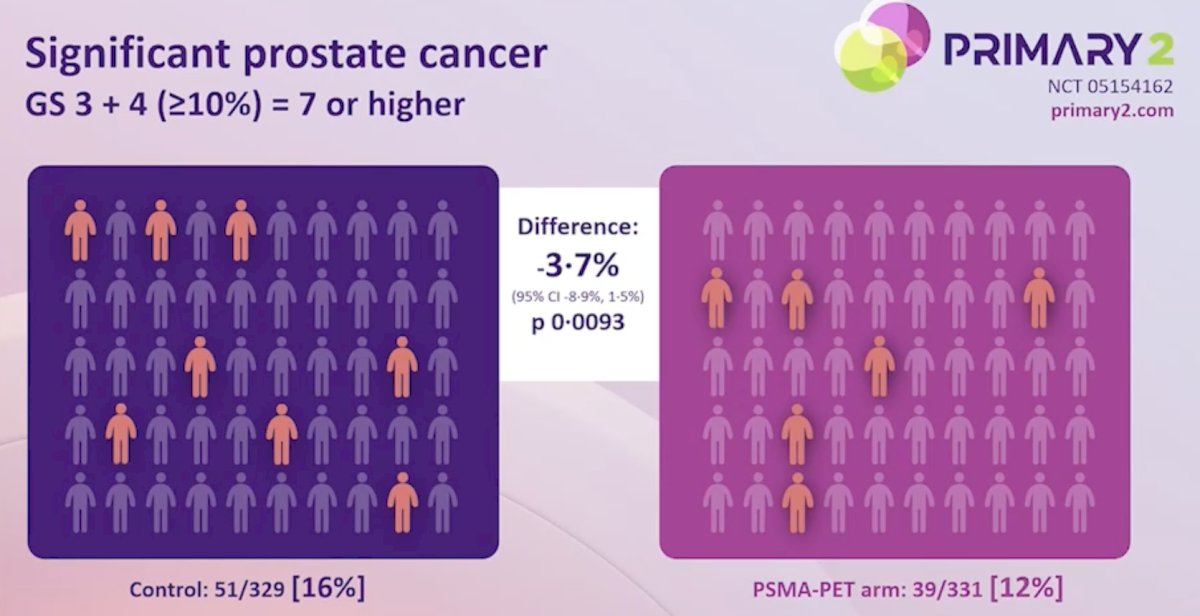
In the 68Ga-PSMA-11 PET/CT arm, significant prostate cancer diagnosis (39/331 [12%]) was non-inferior to the control arm; difference -3.7% (95% CI -8.9%, 1.5%; p = 0.009):
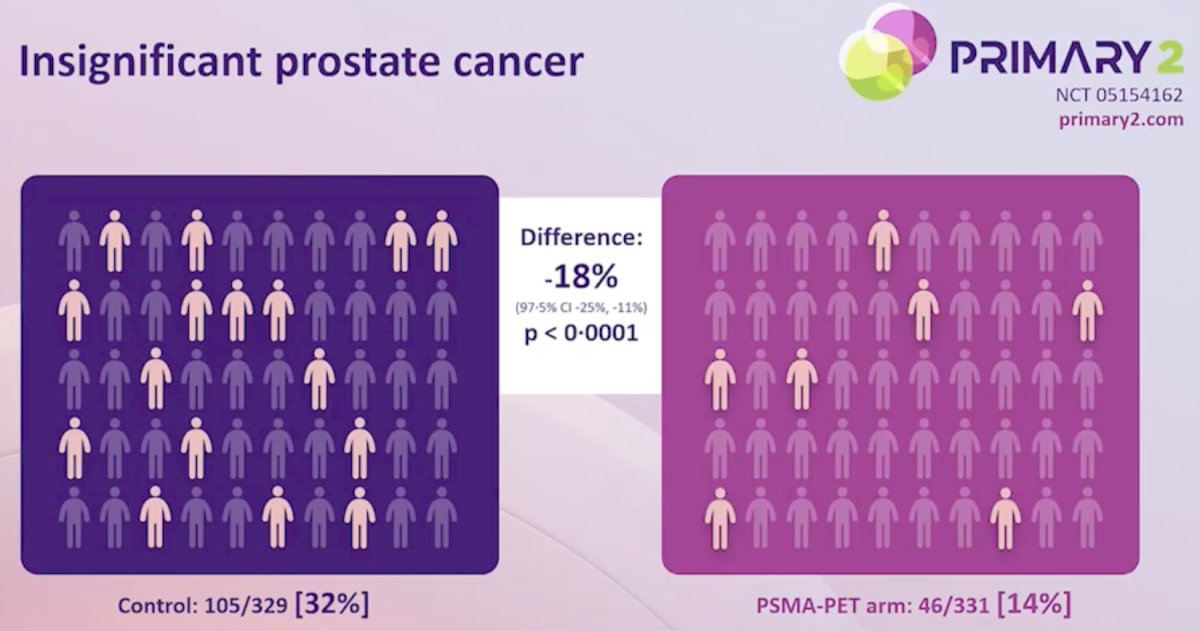
Use of 68Ga-PSMA-11 PET/CT reduced diagnosis of insignificant prostate cancer (46/331 [14%] versus 105/329 [32%]; difference -18% [97.5% CI -25%, -11%; p <0.001]):
The inter-reporter agreement for the PRIMARY score was 0.81:

Strengths of this study include (i) this being the first randomized trial, (ii) utilization of an established imaging modality, and (iii) use of the internationally validated PRIMARY score. Limitations include (i) the definition of clinically significant prostate cancer, (ii) the need for longer term follow-up, and (iii) the MRI images not being centrally reviewed.
Dr. Buteau concluded his presentation discussing results from the PRIMARY2 phase 3 trial with the following take-home points:
- Among men with PI-RADS 3 or PI-RADS 2 lesions on MRI with clinical risk, 68Ga-PSMA-11 PET/CT safely halved the number of biopsies, enabled targeted biopsies without compromising significant prostate cancer diagnosis, and reduced the diagnosis of insignificant prostate cancer
- 68Ga-PSMA-11 PET/CT should be incorporated in the diagnostic pathway of patients with a PI-RADS 3 or high clinical-suspicion PI-RADS 2 on MRI
- Future directions aim to assess anxiety and cancer worry, as well as cost effectiveness
Presented by: James P. Buteau, MD, Peter MacCallum Cancer Centre, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References: