(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to an advanced prostate cancer session hosted jointly by the Advanced Prostate Cancer Consensus Conference (APCCC) and the EAU. Dr. Fabio Turco presented results from the consensus expert voting on high volume, metastatic hormone-sensitive prostate cancer (mHSPC) during the 2024/2025 APCCC meeting and queried the audience regarding their preferred management options for select patient scenarios.1
In patients with high burden mHSPC who are chemotherapy fit, is triplet therapy with ADT + docetaxel + an androgen receptor pathway inhibitor (ARPI) the preferred option? Most of the audience members (68.3%) voted ‘yes, in the majority of patients’, with an additional 25% voting ‘yes, but only in selected patients’.
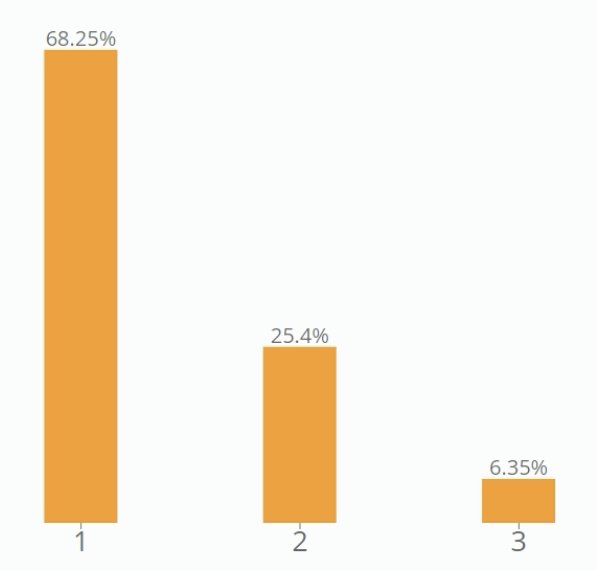
This was overall consistent with the experts’ recommendations, with 54% and 40% having voted in favor of triplet therapy ‘in the majority of patients’ and ‘only in selected patients’, respectively.
If reserving triplet therapy for select patients with high burden mHSPC, ‘what is the most important factor for your decision to use triplet therapy?’ Sixty-eight percent of the audience members voted that CHAARTED disease volume (high versus low) was the most important factor to decide for or against triplet therapy, followed by disease presentation (synchronous versus metachronous) at 23%.
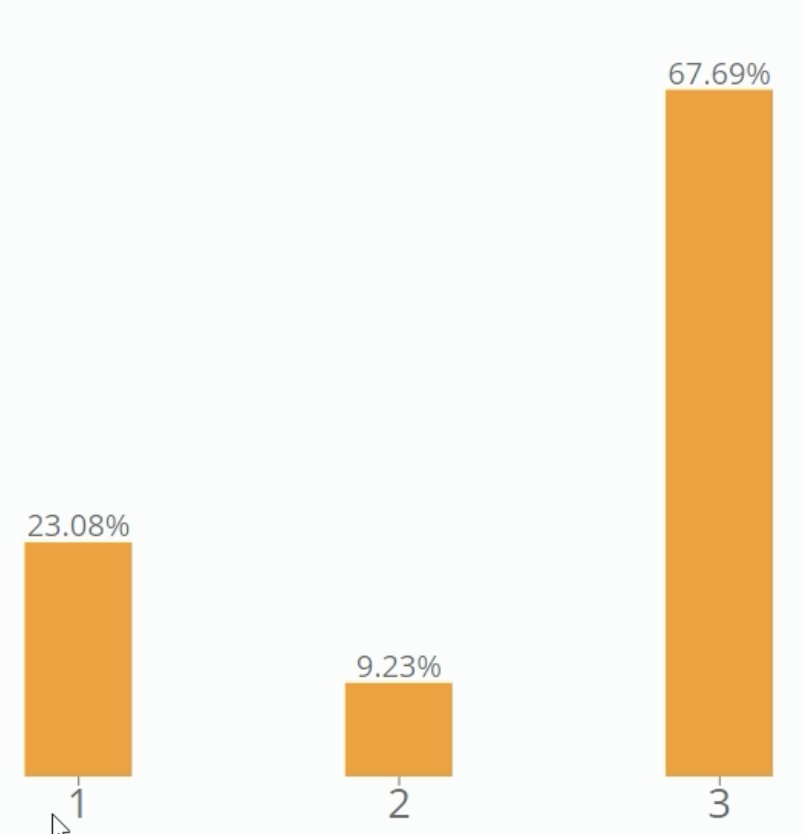
These voting results mirrored those of the experts from the APCCC conference, with 57% and 31% having previously voted in favor of high disease volume and synchronous disease presentation, respectively.

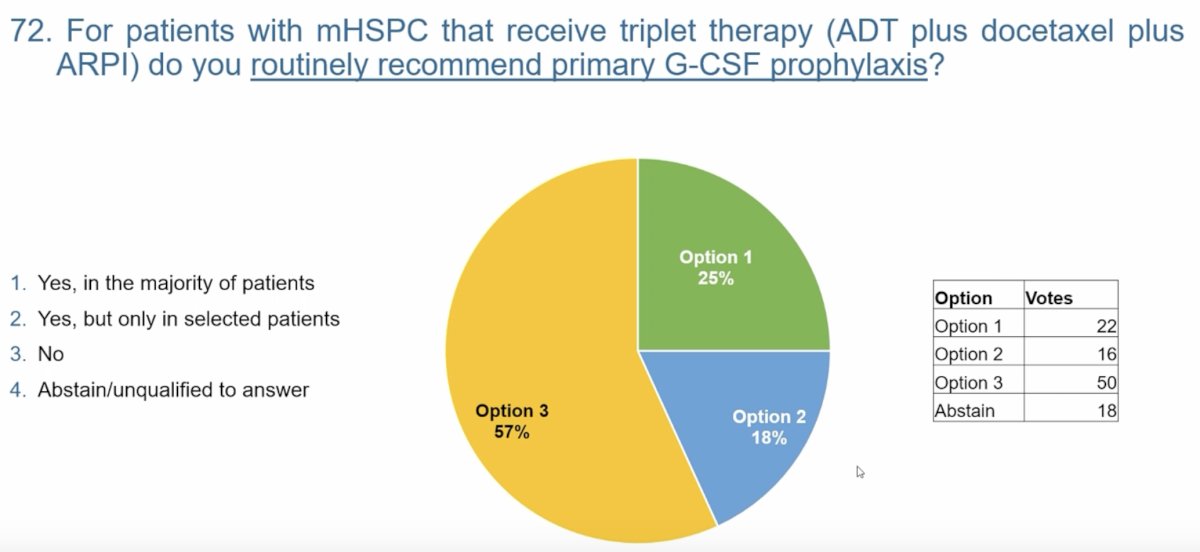
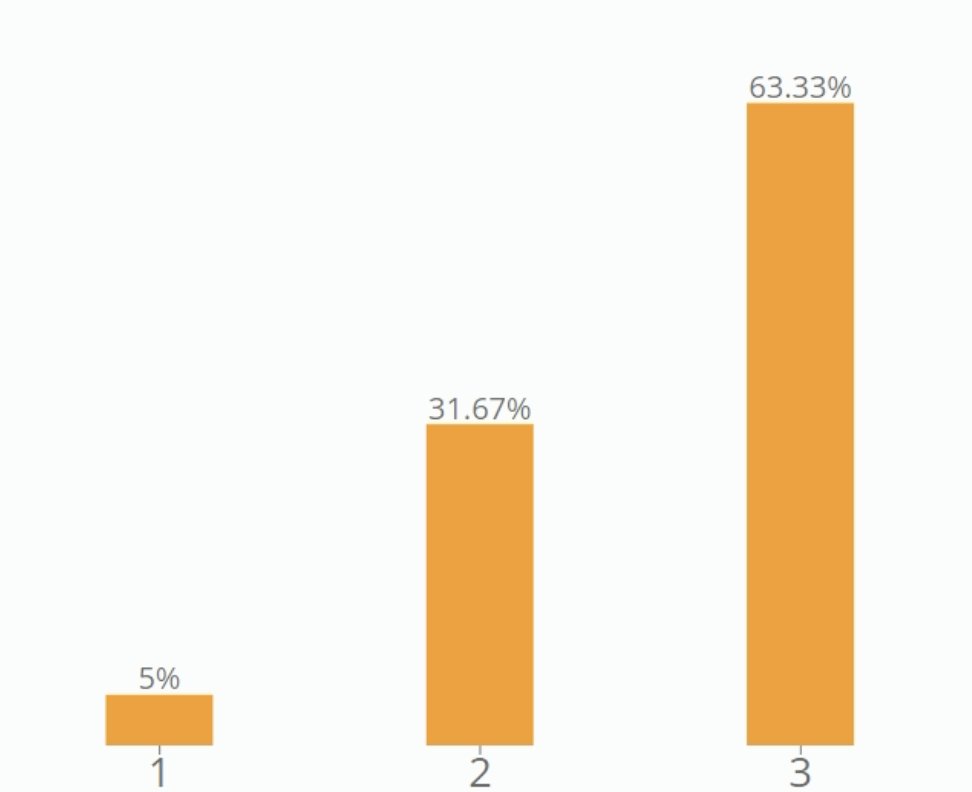
For patients with mHSPC that receive triplet therapy, is primary granulocyte colony-stimulating factor (G-CSF) prophylaxis recommended? The audience was almost evenly split between the three options:

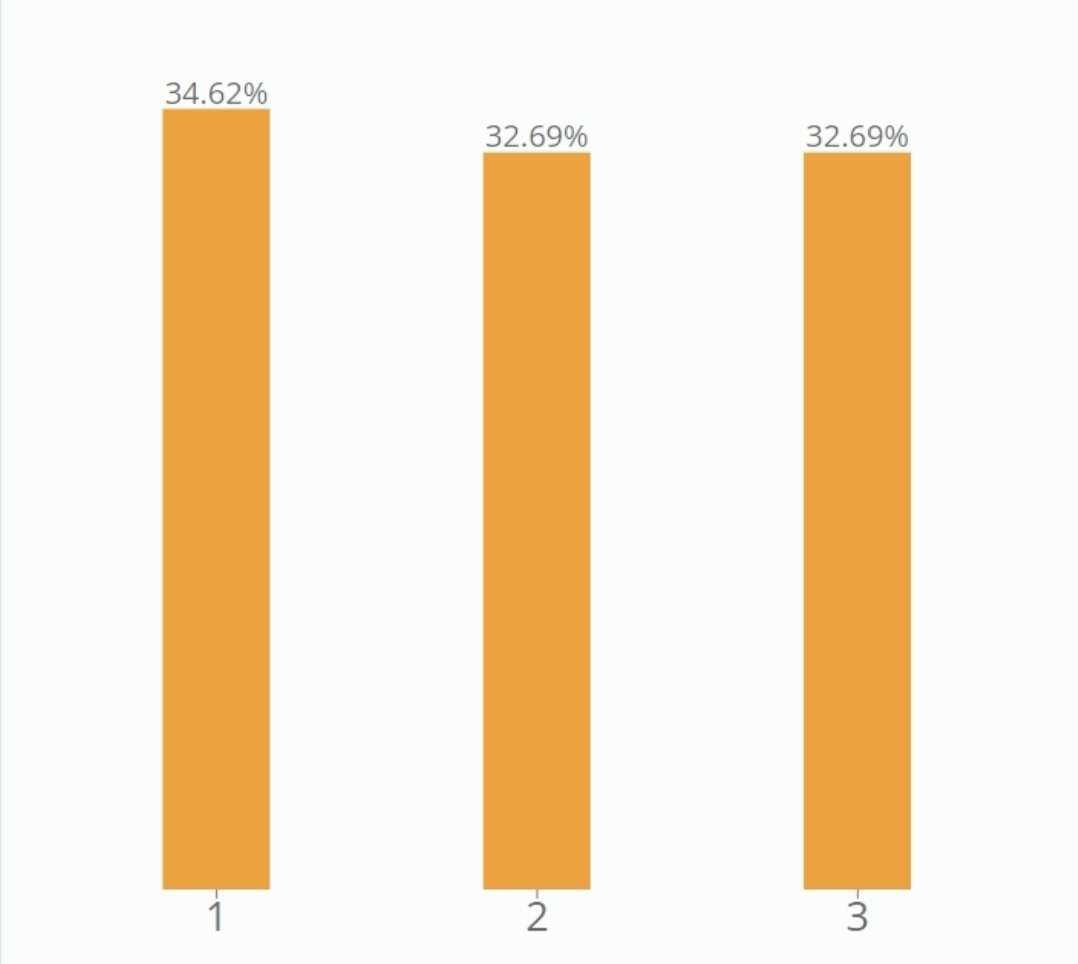
This voting pattern did not reflect the experts’ consensus with 57% having previously voted that ‘the majority of patients’ receiving triplet therapy should be recommended for primary G-CSF prophylaxis.
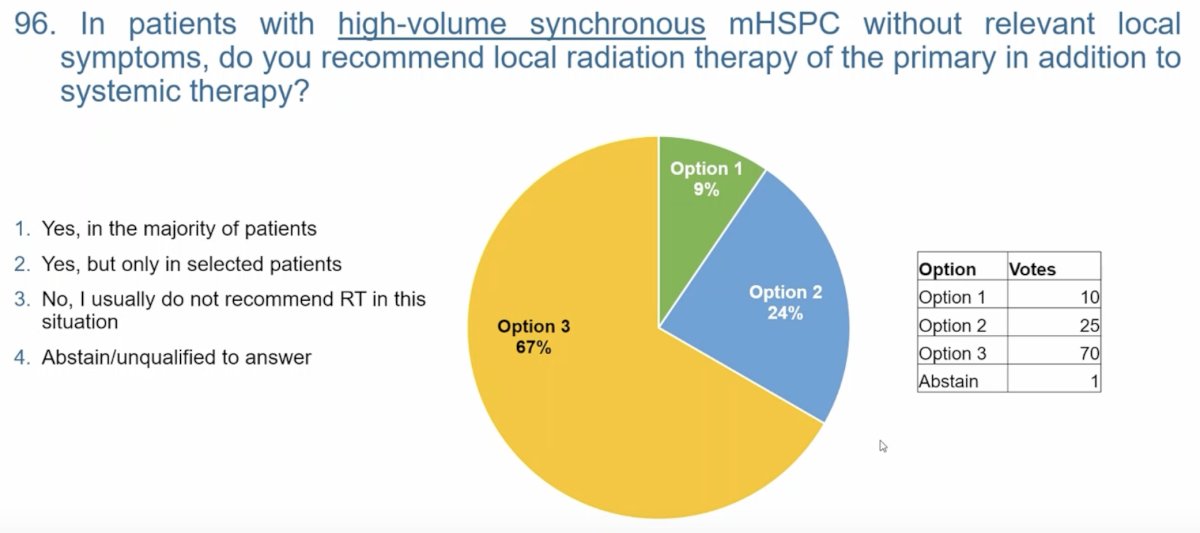
In patients with high-volume, synchronous mHSPC without relevant local symptoms, is local radiation therapy (RT) of the prostate recommended in addition to systemic therapy? The audience mostly (63.3%) voted ‘no, I usually do not recommend RT in this situation’.
These voting results mirrored those of the APCCC experts who had voted strongly (67%) in favor of ‘no, I usually do not recommend RT in this situation’.
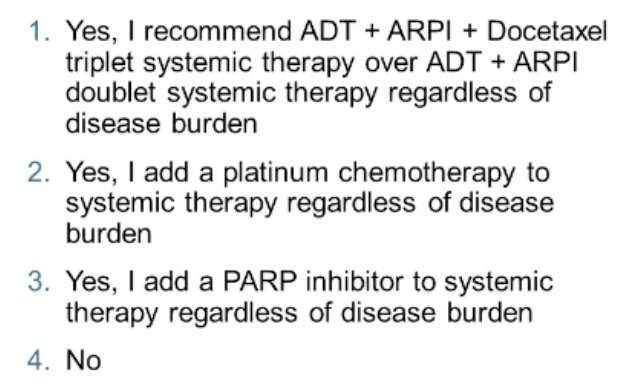
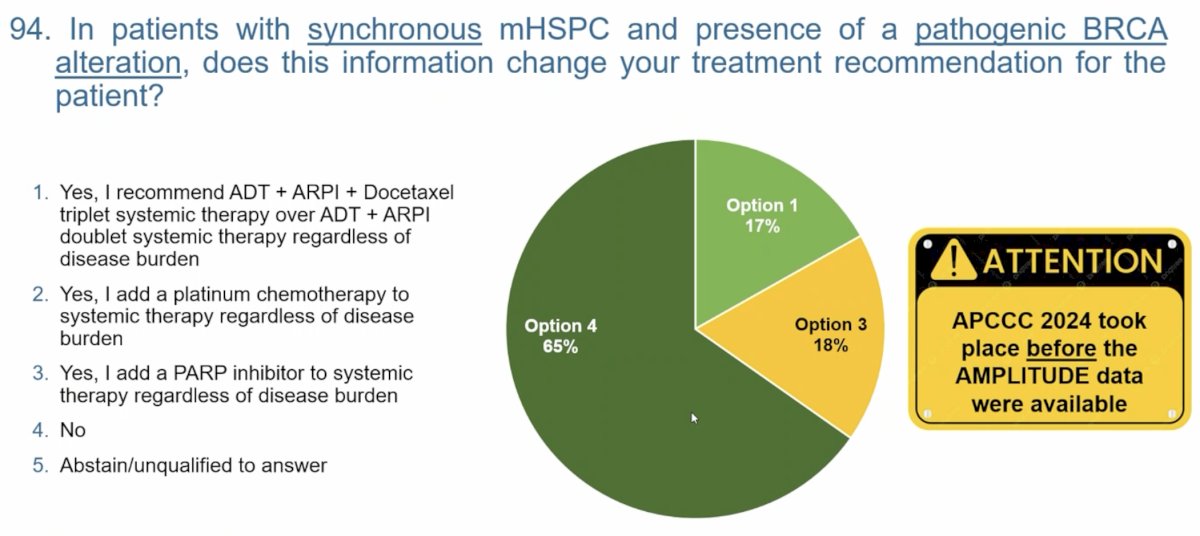
What about patients with homologous recombination repair (HRR) mutations? Dr. Turco asked the following: “In patients with synchronous mHSPC and presence of a pathogenic BRCA alteration, does this information change your treatment recommendation for this patient?” Seventy-one percent of the audience voted ‘yes, I add a PARP inhibitor to systemic therapy regardless of disease burden’. These voting results likely reflect the recently published AMPLITUDE trial, that demonstrated that the addition of niraparib to abiraterone acetate + prednisone in patients with germline or somatic HRR gene alterations significantly improved radiographic progression-free survival, versus placebo (median: not reached versus 29.5 months; HR: 0.63, 95% CI: 0.49-0.80, p=0.0001).2
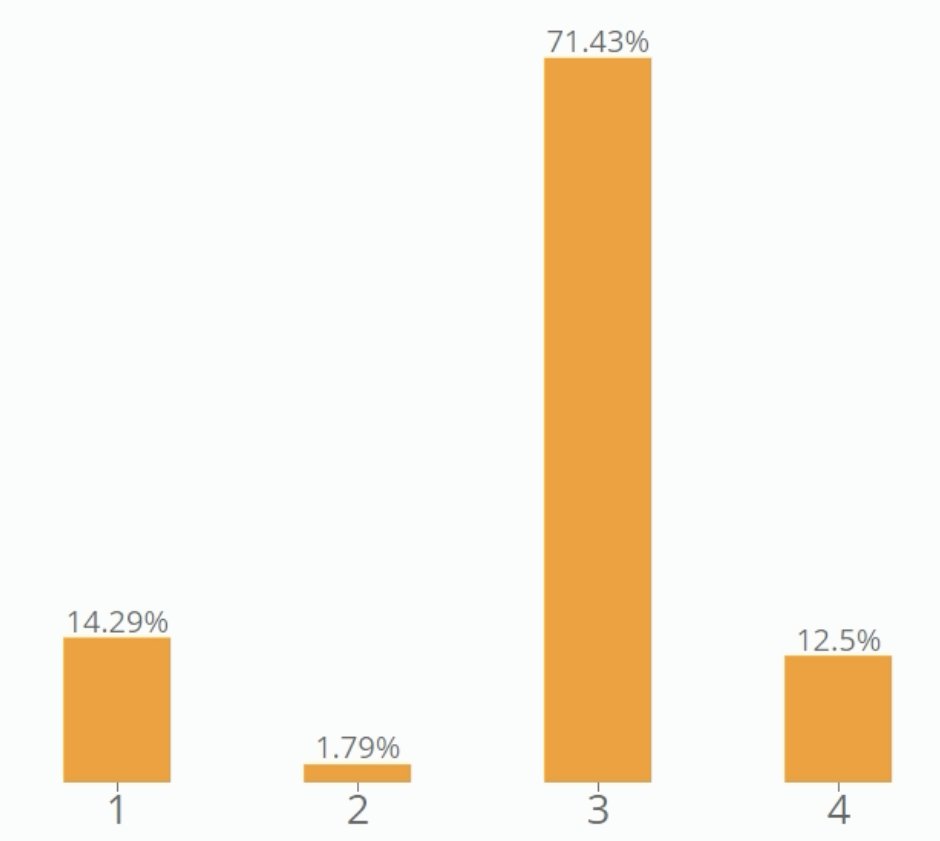
Notably, only 18% of the APCCC experts had voted in favor of adding a PARP inhibitor to systemic therapy regardless of disease burden in such patients with synchronous mHSPC and a pathogenic BRCA alteration. Importantly, this voting had been performed in 2024, prior to the presentation of AMPLITUDE at ASCO 2025.
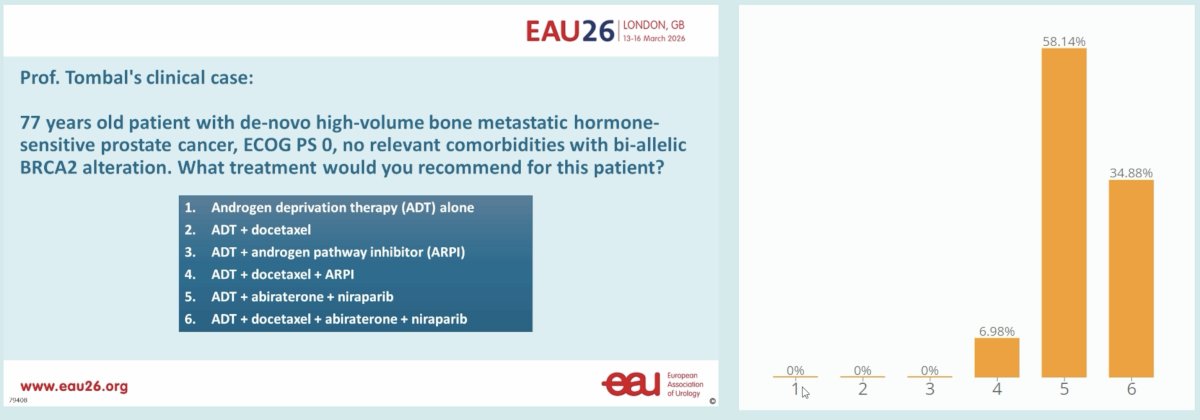
Dr. Turco concluded with a ‘provocative’ case presentation, as follows: “77 years old patient with de-novo, high-volume, bone metastatic hormone-sensitive prostate cancer, ECOG PS 0, no relevant comorbidities with bi-allelic BRCA2 alteration. What treatment would you recommend for this patient?” While clear guidance to address this question remains currently unavailable, 58% of the audience voted in favor of ADT + abiraterone + niraparib. Interestingly, 35% of patients voted in favor of ‘quadruplet’ therapy with ADT + docetaxel + abiraterone + niraparib, which has yet to be formally evaluated in the clinical setting.
Presented by: Fabio Turco, Medical Oncologist Consultant at Oncology Institute of Southern Switzerland, Bellinzona, Switzerland
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Gillessen S, Turco F, Davis ID, et al. Management of Patients with Advanced Prostate Cancer. Report from the 2024 Advanced Prostate Cancer Consensus Conference (APCCC). Eur Urol 2025; 87(2):157-216.
- Attard G, Agarwal N, Graff JN, et al. Niraparib and abiraterone acetate plus prednisone for HRR-deficient metastatic castration-sensitive prostate cancer: a randomized phase 3 trial. Nature. 2025; 31:4109-18.