(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a PARP inhibitors for prostate cancer session and a state of the art lecture by Dr. Gerhardt Attard discussing PARP inhibitors in metastatic hormone-sensitive prostate cancer (mHSPC) and metastatic castration resistant prostate cancer (mCRPC). Two important questions regarding PARP inhibitors for prostate cancer patients include: For whom (which molecular subgroup)? And when (in the treatment cycle)?
As far as when to use PARP inhibitors, the benefit is well established in mCRPC patients across several lines of therapy based on the PROfound,1 TRITON3,2 and PROpel,3 MAGNITUDE,4 and TALAPRO-25 trials:

PROfound was a randomized, open-label, phase III trial of olaparib 300 mg twice daily versus the physician’s choice of standard of care therapy in men with HRR-mutated mCRPC who had disease progression while receiving a novel hormonal agent (e.g., enzalutamide or abiraterone). Patients were assigned to one of two cohorts based on their HRR gene alteration. Cohort A included patients with BRCA1, BRCA2, or ATM alterations, irrespective of co-occurring alterations in any other HRR genes. Cohort B had patients with alterations in any of the other 12 HRR genes (BRIP1, BARD1, CDK12, CHEK 1/2, FANCL, PALB2, PPP2R2A, RAD51B, RAD51C, RAD51D, RAD54L). Patients within each cohort were randomized in a 2:1 fashion to olaparib versus standard of care. This trial found a 66% reduction in the risk of progression or death for olaparib versus a second androgen receptor pathway inhibitor (HR 0.34, 95% CI 0.25-0.47), with a confirmed objective response rate of 33.3% versus 2.3%:

Additionally, olaparib improved overall survival among patients with BRCA1/2 or ATM mutations, with a median overall survival of 19.1 months versus 14.7 months (HR 0.69, 95% CI 0.50-0.97):6

TRITON3 was a randomized phase 3 trial of mCRPC patients with a BRCA1, BRCA2, or ATM alteration who experienced disease progression following treatment with a second-generation androgen receptor pathway inhibitor. Patients underwent 2:1 randomization to receive oral rucaparib (600 mg twice daily) or a physician’s choice control (docetaxel or a second-generation androgen receptor pathway inhibitor [abiraterone acetate or enzalutamide]). The primary outcome was the median progression-free survival according to an independent review. In the BRCA mutation subgroup assessing rucaparib versus docetaxel, there was a progression-free survival benefit for rucaparib (HR 0.53, 95% CI 0.37-0.77), which was also seen when assessing rucaparib versus a second androgen receptor pathway inhibitor (HR 0.38, 95% CI 0.25-0.58):
![TRITON3 was a randomized phase 3 trial of mCRPC patients with a BRCA1, BRCA2, or ATM alteration who experienced disease progression following treatment with a second-generation androgen receptor pathway inhibitor. Patients underwent 2:1 randomization to receive oral rucaparib (600 mg twice daily) or a physician’s choice control (docetaxel or a second-generation androgen receptor pathway inhibitor [abiraterone acetate or enzalutamide]). The primary outcome was the median progression-free survival according to an independent review. In the BRCA mutation subgroup assessing rucaparib versus docetaxel, there was a progression-free survival benefit for rucaparib (HR 0.53, 95% CI 0.37-0.77), which was also seen when assessing rucaparib versus a second androgen receptor pathway inhibitor (HR 0.38, 95% CI 0.25-0.58):](/images/com-doc-importer/252-eau-2026/eau-2026-state-of-the-art-lecture-parp-inhibitors-in-mhspc-and-mcrpc/image-3.jpg)
TALAPRO-2 assessed talazoparib + enzalutamide versus placebo + enzalutamide in patients with androgen receptor pathway inhibitor naïve BRCA mutated mCRPC, noting a median radiographic progression of not reached versus 11.0 months, respectively (HR 0.26, 95% CI 0.16-0.42):
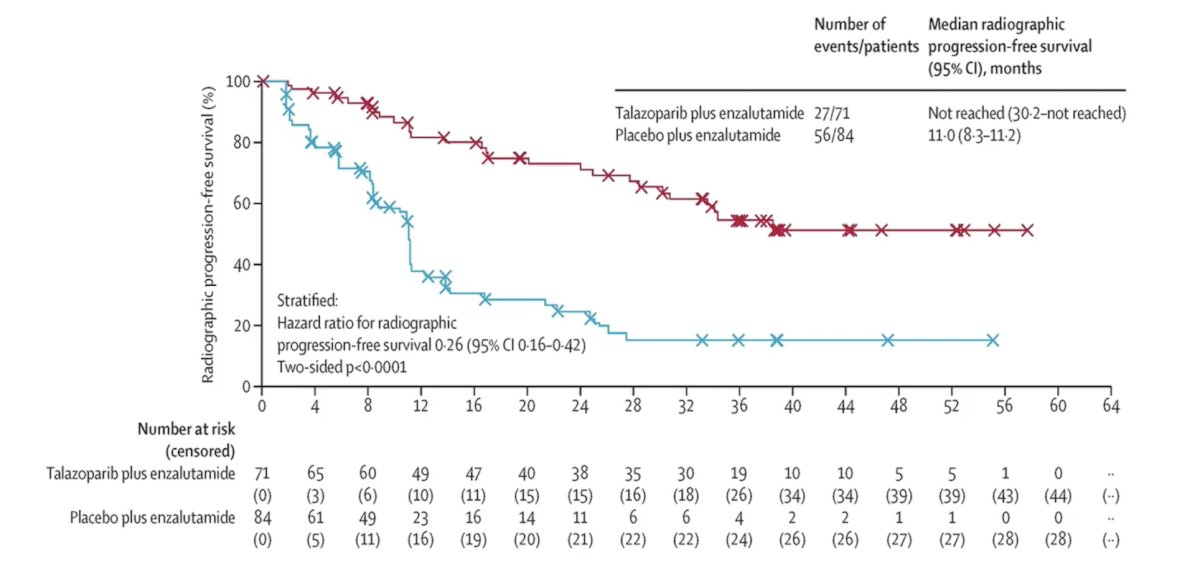
With additional follow-up, this also corresponded to a median overall survival of not reached in the talazoparib + enzalutamide arm versus 28.5 months in the placebo + enzalutamide (HR 0.50, 95% CI 0.32-0.78):7

Based on the aforementioned data, Dr. Attard emphasized that every BRCA-positive patient with mCRPC should receive a PARP inhibitor.
More recently, we have also seen PARP inhibitors move into the mHSPC disease space with the reporting of the AMPLITUDE study:8
![More recently, we have also seen PARP inhibitors move into the mHSPC disease space with the reporting of the AMPLITUDE [8] study:](/images/com-doc-importer/252-eau-2026/eau-2026-state-of-the-art-lecture-parp-inhibitors-in-mhspc-and-mcrpc/image-6.jpg)
The AMPLITUDE trial evaluated combining niraparib with abiraterone acetate + prednisone versus placebo and abiraterone acetate + prednisone in mHSPC with HRR gene alterations. The primary endpoint was met, with a significant improvement in radiographic progression-free survival observed in the BRCA subgroup: median not reached for niraparib and abiraterone acetate + prednisone group versus 26 months for the abiraterone acetate + prednisone group (HR 0.52, 95% CI 0.37-0.72; p < 0.0001). This was also noted in the intention to treat population (HR 0.63, 95% CI 0.49-0.80; p = 0.0001):
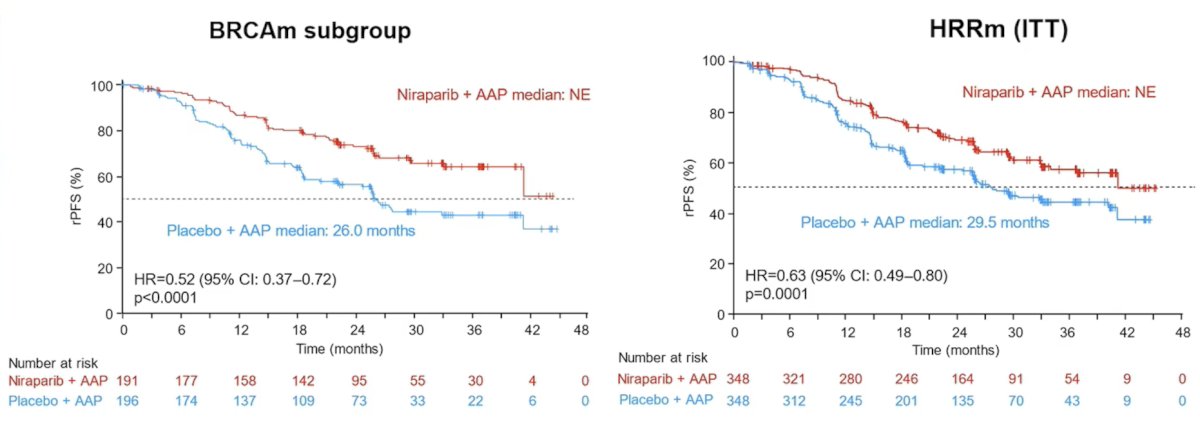
The data for overall survival are immature but favor niraparib and abiraterone acetate + prednisone in the BRCA subgroup (HR 0.75, 95% CI 0.51-1.11), as well as in the intention-to-treat population (HR 0.79, 95% CI 0.59-1.04):

Is earlier treatment with a PARP inhibitor better than later? Dr. Attard provided the following table from the AMPLITUDE trial, demonstrating that 33.3% of patients in the placebo + abiraterone acetate + prednisone group received a PARP inhibitor:

Taken together, patients with tumors harboring a BRCA1 or BRCA2 alteration derive the greatest overall survival benefit from a PARP inhibitor, which is highlighted in the PROfound exploratory gene-level analysis for olaparib and overall survival:

Finally, Dr. Attard emphasizes the toxicity cost of PARP inhibitors, most notably anemia of any grade, which occurs in 40-70% of patients, with up to 30% requiring blood transfusions. Neutropenia is also common, occurring in 35% of patients, as well as thrombocytopenia in 30% of patients. Moreover, gastrointestinal disturbances occur in 20-40% of patients, fatigue in 30% of patients, hypertension in 20-50% when combined with an androgen receptor pathway inhibitor, as well as 10% more cardiovascular events than with patients receiving an androgen receptor pathway inhibitor alone. Myelodysplastic syndrome and acute myeloid leukemia are also possible, with more data required in the mHSPC disease space to truly assess the inherent risk.
Dr. Attard concluded his presentation discussing PARP inhibitors in mHSPC and mCRPC by emphasizing his take-home message to not forget to test for BRCA mutations.
Presented by: Gerhardt Attard, MD, PhD, FRCP, John Black Charitable Foundation Endowed Chair in Urological Cancer Research, University College London, UCL Cancer Institute, London, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- de Bono J, Mateo J, Fizazi K, et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med 2020 May 28;382(22):2091-2102.
- Fizazi K, Piulats JM, Reaume MN, et al. Rucaparib or Physician’s Choice in Metastatic Prostate Cancer. N Engl J Med. 2023 Feb 23;388(8):719-732.
- Saad F, Clarke NW, Oya M, et al. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomized, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108.
- Chi KN, Rathkopf D, Smith MR, et al. Niraparib and abiraterone acetate for metastatic castration-resistant prostate cancer. J Clin Oncol. 2023 Jun 20;41(18):3339-3351.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.
- Hussain M, Mateo J, Fizazi K, et al. Survival with Olaparib in Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2020 Dec 10;383(24):2345-2357.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with metastatic-castration-resistant prostate cancer: final overall survival results from the randomized, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet. 2025 Aug 2;406(10502):447-460.
- Attard G, Agarwal N, Graff JN, et al. Niraparib and abiraterone acetate plus prednisone for HRR-deficient metastatic castration-sensitive prostate cancer: A randomized phase 3 trial. Nat Med. 2025 Dec;31(12):4109-4118.