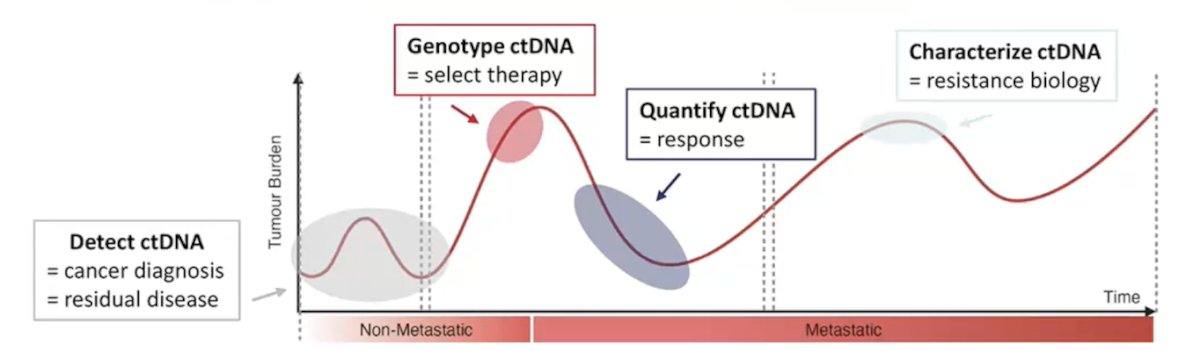
(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a PARP inhibitors for prostate cancer session and a presentation by Dr. Alexander Wyatt discussing when to use ctDNA in prostate cancer. Cells undergoing apoptosis shed fragments into the blood, with most ‘normal’ cell-free DNA (cfDNA) originating from the blood lineage (half life = minutes). In a person with cancer, some cfDNA is tumor derived and termed ctDNA, which is associated with active cancer. As such, ctDNA has emerged as a utility across the spectrum of prostate cancer:
Importantly, ctDNA genotyping can identify DNA repair gene alterations, such as BRCA2 mutations, with the frequency of somatic alterations in ctDNA similar to tumor tissue:
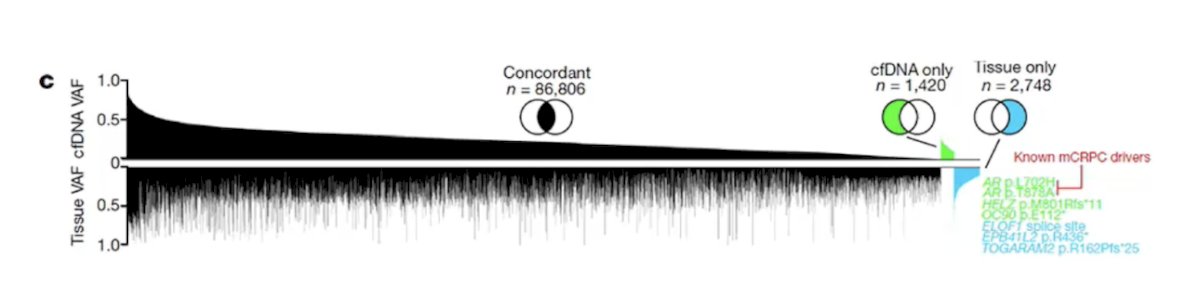
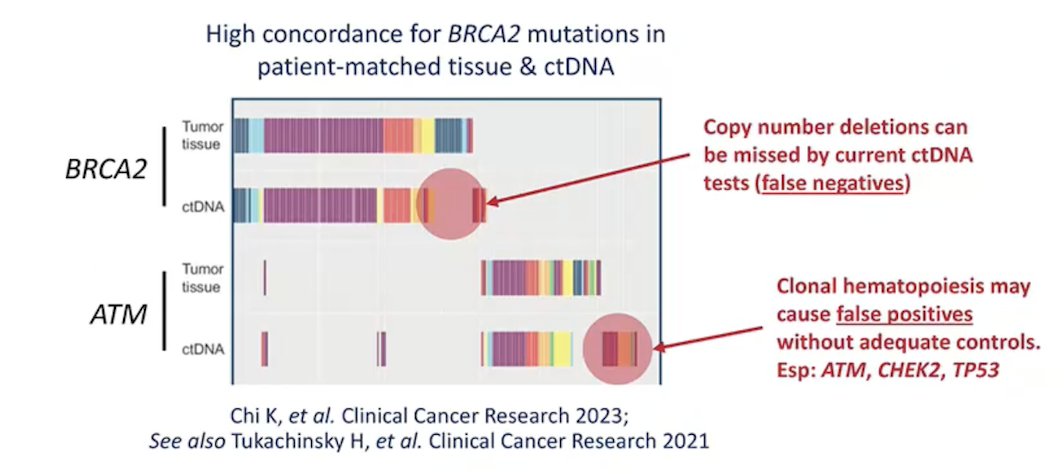
Previous studies have shown that genome wide mutation and copy number concordance is 85-95% for synchronous tumor tissue and ctDNA. Moreover, DNA repair defects tend to be ‘truncal’ and present in all tumor populations. Concordance between ctDNA and DNA repair gene alterations is high, but Dr. Wyatt cautions that we must be aware of false negatives due to low ctDNA:
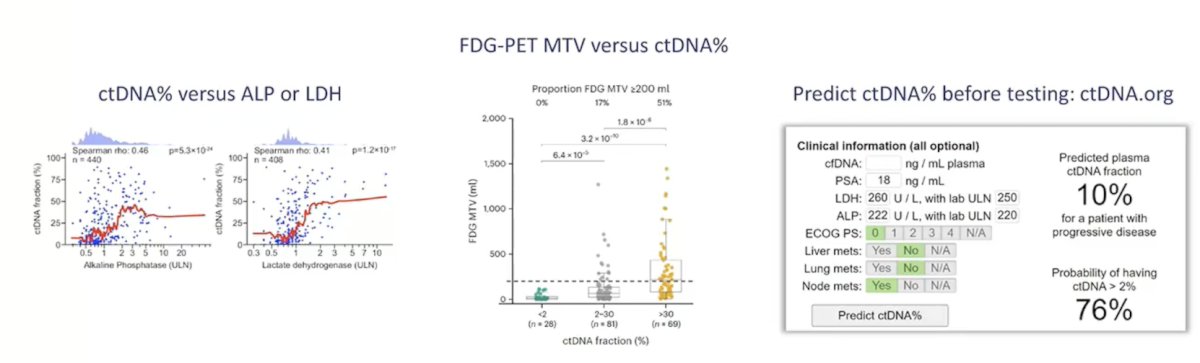
Dr. Wyatt recommends using genotype testing when ctDNA is high, and ordering tests for BRCA2 status at times of progressive disease. The ctDNA percentage is correlated with clinical metrics of active tumor burden, such as (i) ctDNA percentage versus ALP or LDH, (ii) FDG-PET MTV versus ctDNA percentage, or (iii) predicting ctDNA percentage before testing:
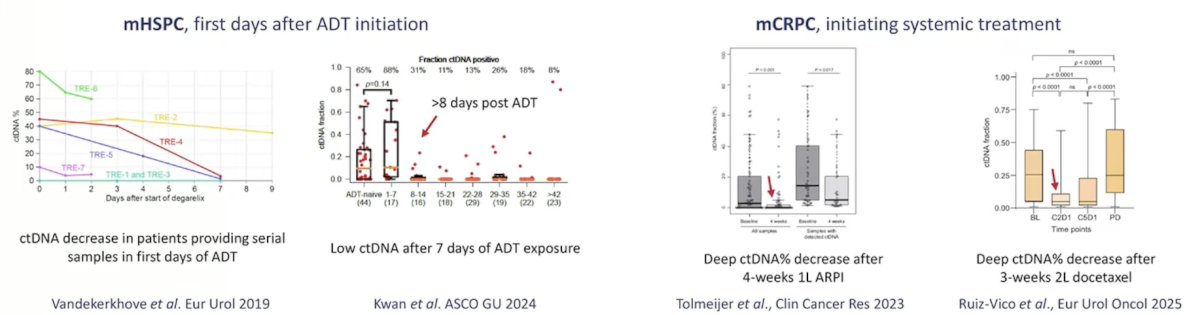
ctDNA fraction typically decreases during treatment response, with deep declines in the first weeks after systemic treatment initiation. Dr. Wyatt states that there is no evidence of a durable ‘spike’ in ctDNA levels in responding disease, and it is difficult to obtain a pre-ADT blood sample for testing in mHSPC:
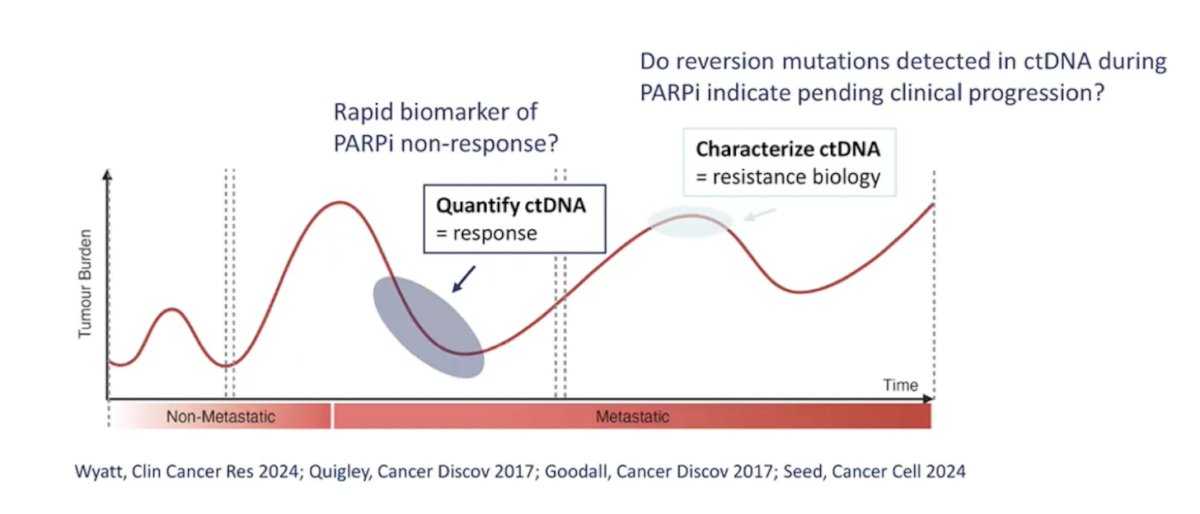
Dr. Wyatt concluded his presentation discussing when to use ctDNA in prostate cancer by emphasizing emerging clinical uses for ctDNA in the context of PAPR inhibitors, specifically monitoring for treatment response and resistance:
- Early on treatment declines in ctDNA percentage are associated with durable clinical benefit
- Polyclonal BRCA2 ‘reversion’ mutations are observed in ctDNA at progression on PARP inhibitors in patients with an initial response
Presented by: Alexander Wyatt, PhD, Vancouver Prostate Centre, University of British Columbia, Vancouver, British Columbia, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.