(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., was host to the Hormone sensitive metastatic prostate cancer: Thematic Session. Dr. Alberto Bossi delivered a presentation titled: RT to primary tumor, what for?
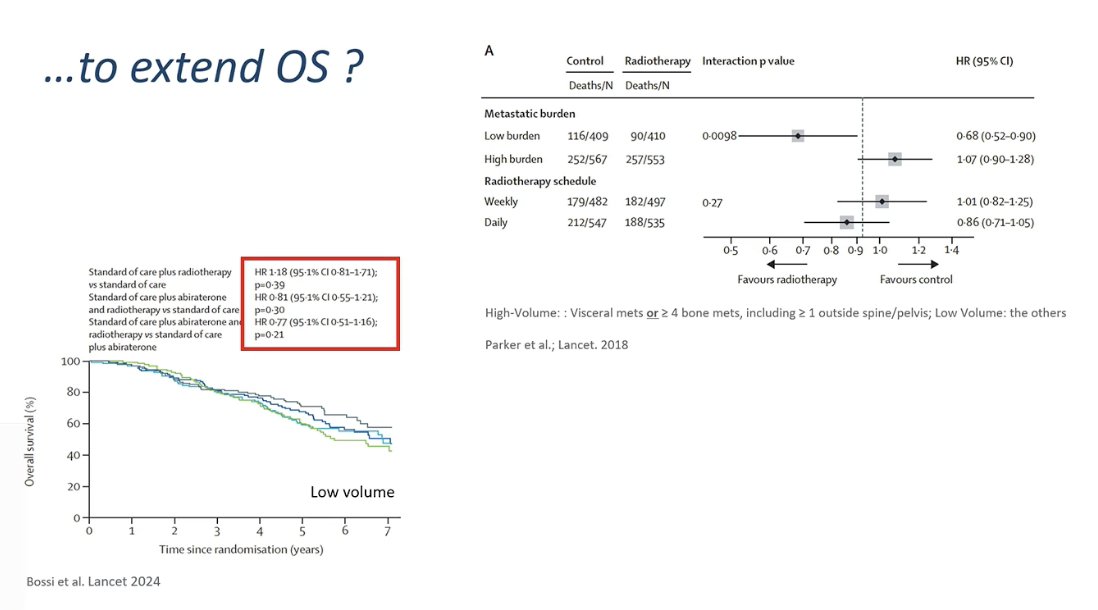
Dr. Bossi began by highlighting the well-known STOPCAP meta-analysis of individual participant data (IPD) but emphasized that important differences exist among the trials included in the analysis.1 He noted that the systemic therapies used across these studies varied substantially. For example, in the HORRAD trial, patients received ADT alone, whereas in PEACE-1, a large proportion of patients received treatment intensification, with approximately 50% receiving abiraterone and about 60% receiving docetaxel.1-3 These differences in background systemic therapy likely contributed to the variation in survival outcomes observed across the trials.

Dr. Bossi then raised the question of whether the goal of local prostate radiotherapy in metastatic disease should be to extend overall survival. For patients with low-volume metastatic disease, prior evidence, particularly from STAMPEDE, suggests that local radiotherapy can indeed improve survival. However, this effect was not clearly confirmed in the PEACE-1 trial, likely because many patients also received intensified systemic therapy such as abiraterone and docetaxel.4 As a result, the survival impact of local radiotherapy may be more difficult to detect when highly effective systemic treatments are already being administered.
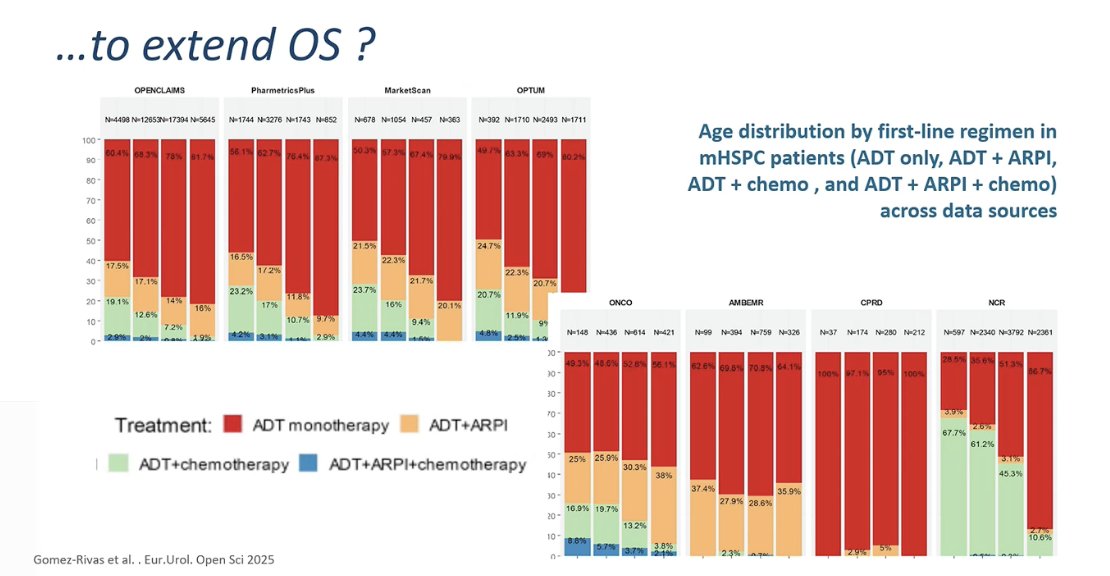
Dr. Bossi then reviewed real-world treatment patterns using data from the PIONEER 2.0 Big Data Investigation Group. This large analysis included nearly 49,000 patients with mHSPC across several international databases and provides a broad picture of how patients are treated outside clinical trials. Importantly, the characteristics of these patients closely resemble those seen in routine clinical practice. The analysis highlights substantial heterogeneity in treatment approaches, with many patients still receiving ADT alone, while others receive intensified regimens such as ADT + ARPI or ADT + chemotherapy.5
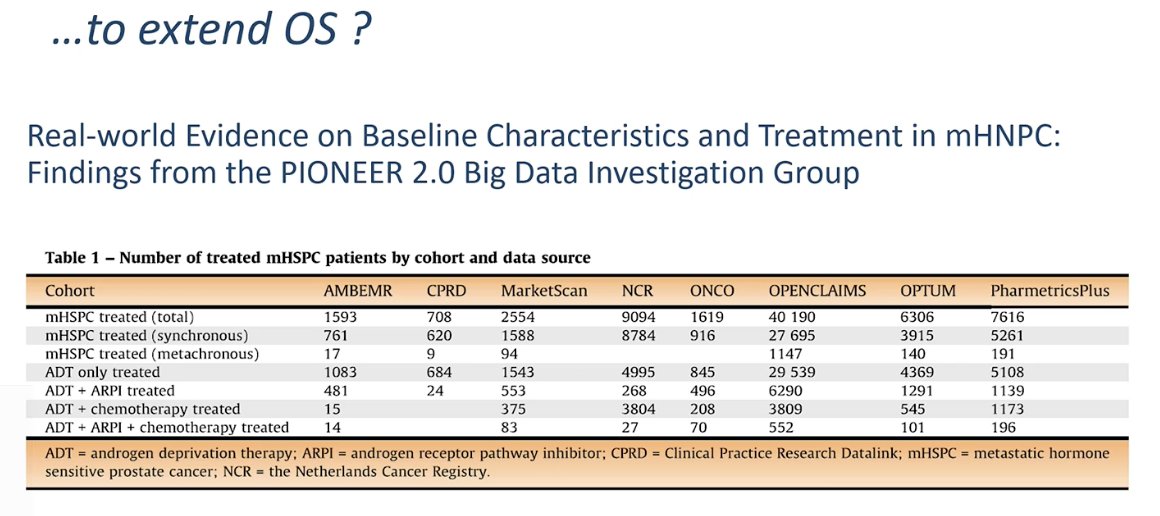
Real-world data show a persistent gap between guideline recommendations and everyday clinical practice. Across multiple large datasets, many patients with mHSPC continue to receive ADT alone, despite clear evidence supporting treatment intensification with ARPIs. These findings highlight that a substantial proportion of patients are still undertreated in routine practice. He noted that while local radiotherapy to the prostate may contribute to improved outcomes in selected patients, systemic intensification remains essential. Ultimately, he stressed the importance of discussing these treatment options with patients and understanding their priorities, including whether extending overall survival is a key goal of care.
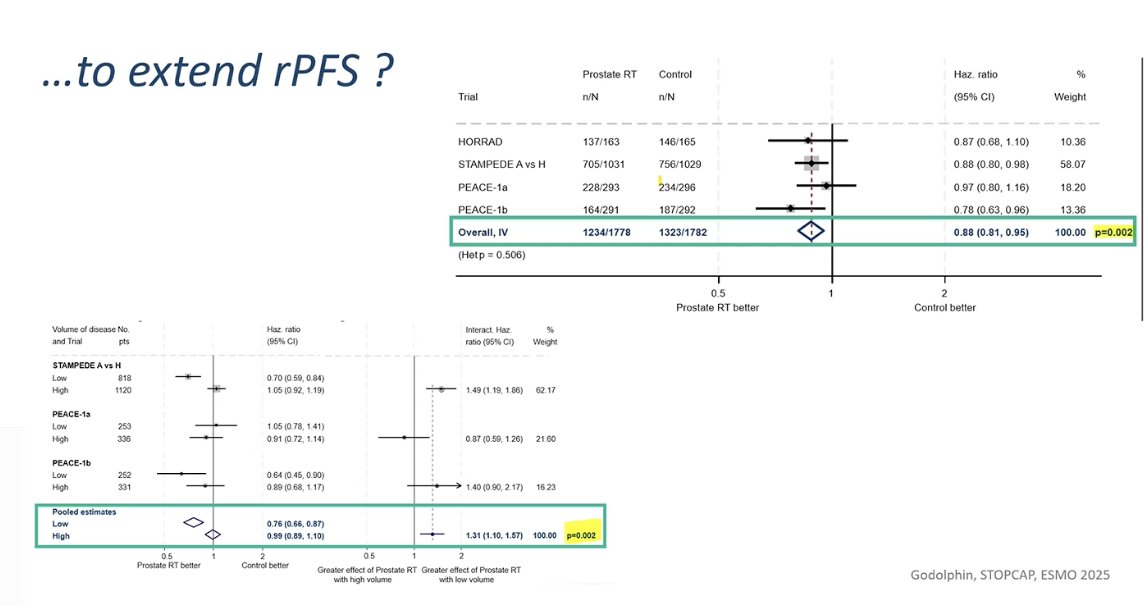
Dr. Bossi then discussed whether local radiotherapy could improve radiographic progression-free survival (rPFS). Data from pooled analyses of trials such as HORRAD, STAMPEDE, and PEACE-13,4 suggest that prostate radiotherapy may indeed reduce the risk of radiographic progression or death, with a significant improvement in rPFS observed overall. He noted that rPFS, defined as the time from randomization to radiographic progression or death from any cause, is an endpoint that many patients value, as it reflects a delay in disease progression. Therefore, even if the overall survival benefit remains debated in certain settings, improving rPFS may still represent a clinically meaningful outcome for patients.
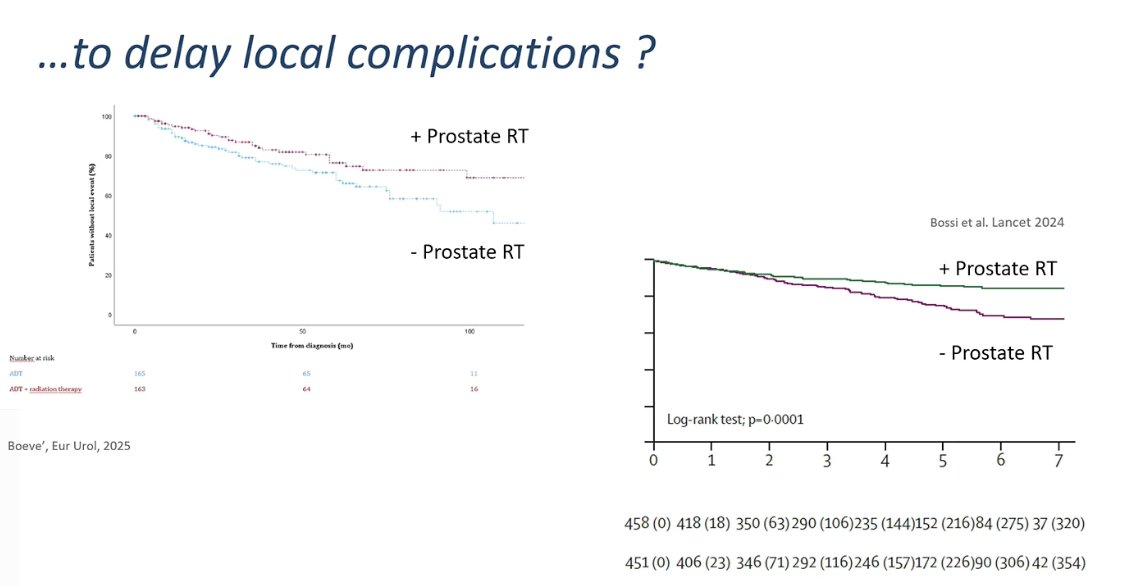
Another potential goal of local prostate radiotherapy is delaying local complications of the disease. Updated analyses from trials such as HORRAD, recently reported with longer follow-up, suggest that adding prostate radiotherapy can reduce or delay the occurrence of local complications, including urinary obstruction, hematuria, or the need for palliative interventions. Importantly, this effect appears to be observed across the overall study population, regardless of metastatic burden. He emphasized that these data should be discussed with patients, as delaying local complications may represent a meaningful clinical benefit even when the impact on overall survival is less clear.3
Dr. Bossi then presented additional data from PEACE-1 examining whether local prostate radiotherapy could delay the development of castration-resistant disease. The analysis showed a significant improvement in castration-resistant prostate cancer–free survival with the addition of prostate radiotherapy, both in patients with low-volume metastatic disease and in the overall study population. These findings suggest that local treatment may help delay progression to castration resistance, independent of metastatic burden, representing another potential clinical benefit of prostate radiotherapy in this setting.1,4

Dr. Bossi concluded that prostate radiotherapy should be considered for most patients presenting with de novo mHSPC. Evidence from the STOPCAP meta-analysis supports a benefit in radiographic progression-free survival and overall survival in patients with low-volume disease. In addition, data from trials such as PEACE-1, HORRAD, and STAMPEDE show that prostate radiotherapy can reduce severe local genitourinary complications and delay progression to castration-resistant disease across disease burdens.1-5 Importantly, toxicity from prostate radiotherapy is generally low. He also noted that real-world data continue to show that many patients still receive ADT alone; in these situations, where systemic therapy is less intensified, local radiotherapy may have an even greater impact on outcomes, including survival.
Notably, there are clinical scenarios in which prostate radiotherapy may not provide benefit. Patients presenting at diagnosis with severe local GU symptoms requiring interventions such as TURP, those with high-volume disease and visceral metastases, or patients treated with triplet therapy who demonstrate poor response after docetaxel may be less likely to benefit from local RT. In addition, he noted that in the era of PSMA-directed strategies, the role of prostate radiotherapy remains uncertain and requires further investigation.
Presented by: Alberto Bossi, MD, Head of the Urology and Prostate Brachytherapy Unit, Gustave Roussy Cancer Institute, Villejuif, France
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:- Burdett S, Boevé LM, Ingleby FC, Fisher DJ, Rydzewska LH, Vale CL, van Andel G, Clarke NW, Hulshof MC, James ND, Parker CC, Parmar MK, Sweeney CJ, Sydes MR, Tombal B, Verhagen PC, Tierney JF; STOPCAP M1 Radiotherapy Collaborators. Prostate Radiotherapy for Metastatic Hormone-sensitive Prostate Cancer: A STOPCAP Systematic Review and Meta-analysis. Eur Urol. 2019 Jul;76(1):115-124. doi: 10.1016/j.eururo.2019.02.003. Epub 2019 Feb 28. PMID: 30826218; PMCID: PMC6575150.
- Fizazi K, Foulon S, Carles J, Roubaud G, McDermott R, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Gravis G, Calabro F, Berdah JF, Hasbini A, Silva M, Thiery-Vuillemin A, Latorzeff I, Mourey L, Laguerre B, Abadie-Lacourtoisie S, Martin E, El Kouri C, Escande A, Rosello A, Magne N, Schlurmann F, Priou F, Chand-Fouche ME, Freixa SV, Jamaluddin M, Rieger I, Bossi A; PEACE-1 investigators. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707. doi: 10.1016/S0140-6736(22)00367-1. Epub 2022 Apr 8. PMID: 35405085.
- Boevé LMS, Hulshof MCCM, Verhagen PCMS, Twisk JWR, Witjes WPJ, de Vries P, Jeroen A van Moorselaar R, Vis AN, van Andel G. Prostate Cancer-related Events in Patients with Synchronous Metastatic Hormone-sensitive Prostate Cancer Treated with Androgen Deprivation Therapy with and Without Concurrent Radiation Therapy to the Prostate; Data from the HORRAD Trial. Eur Urol. 2025 Mar;87(3):357-363. doi: 10.1016/j.eururo.2024.08.035. Epub 2024 Sep 20. PMID: 39304427.
- Bossi A, Foulon S, Maldonado X, Sargos P, MacDermott R, Kelly P, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Salem N, Calabro F, Berdah JF, Hasbini A, Silva M, Boustani J, Ribault H, Fizazi K; PEACE-1 investigators. Efficacy and safety of prostate radiotherapy in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2024 Nov 23;404(10467):2065-2076. doi: 10.1016/S0140-6736(24)01865-8. Erratum in: Lancet. 2025 May 10;405(10490):1665. doi: 10.1016/S0140-6736(25)00903-1. PMID: 39580202.
- Lawlor A, Beyer K, Russell B, Steinbeisser C, Bjartell A, De Meulder B, Omar MI, Hulsen T, Butler J, N'Dow J, Rivas JG, Gandaglia G, Nicoletti R, Sakalis V, Smith EJ, Maass M, Zong J, Fullwood L, Abbott T, Tafreshiha A, Papineni K, Snijder R, Horgan D, Seager S, Evans-Axelsson S, Ribal MJ, Roobol MJ, Van Hemelrijck M; PIONEER Consortium. PIONEER big data platform for prostate cancer: lessons for advancing future real-world evidence research. Nat Rev Urol. 2025 Feb;22(2):116-124. doi: 10.1038/s41585-024-00925-4. Epub 2024 Sep 9. PMID: 39251785.