(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a late-breaking abstracts session and a presentation by Dr. M. Ruggeri discussing a 10-year follow-up of a phase 3 trial assessing extended versus limited pelvic lymph node dissection during radical prostatectomy for intermediate- and high-risk prostate cancer. The role of pelvic lymph node dissection in treating prostate cancer patients remains controversial, due to the lack of randomized trials with more extended and longer follow-up.
Dr. Ruggeri and colleagues previously reported early oncological outcomes from a randomized trial comparing limited pelvic lymphadenectomy versus extended pelvic lymphadenectomy during radical prostatectomy, and at EAU 2026, they reported updated data. The primary endpoint was biochemical recurrence-free survival, and the secondary endpoints were metastasis-free survival and cancer-specific survival.
Between May 2012 and December 2016, in a single institution, 300 patients with D'Amico intermediate or high risk prostate cancer (≥ cT2b and/or ≥ PSA 10 ng/mL and/or Gleason score ≥ 7), absence of bone metastasis, and no previous treatment were randomized to undergo extended pelvic lymphadenectomy (bilaterally chains: obturator, external iliac, internal iliac, common iliac, and pre-sacral) or limited pelvic lymphadenectomy (obturator chains) in proportion 1:1 (extended pelvic lymphadenectomy n = 150; limited pelvic lymphadenectomy n = 150) during radical prostatectomy. The trial was designed to demonstrate a minimum 15% advantage in 5-year biochemical recurrence-free survival with extended pelvic lymphadenectomy.
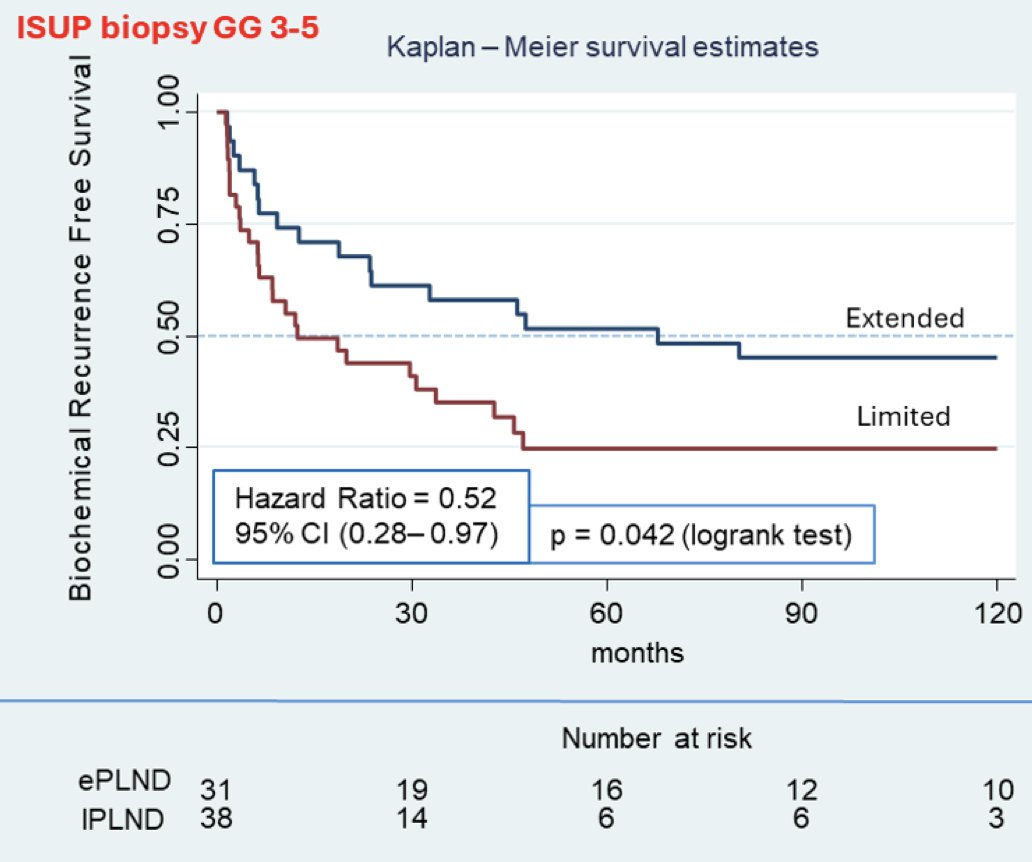
The mean and median follow-up were 113 and 123 months, respectively. Considering the whole cohort, there were similar biochemical recurrence rates between the arms (HR 0.91, 95% CI 0.79-1.28; p = 0.556). Additionally, there were no differences in metastasis-free survival (HR 0.63, 95% CI 0.31-1.25; p = 0.187) or cancer-specific survival (HR 0.99, 95% CI 0.29-3.42; p =0.988). Nevertheless, patients with preoperative biopsy ISUP grade groups 3–5 who underwent extended pelvic lymphadenectomy had better biochemical recurrence-free survival (HR 0.52, 95% CI 0.28-0.97; p =0.042; number needed to treat = 6):
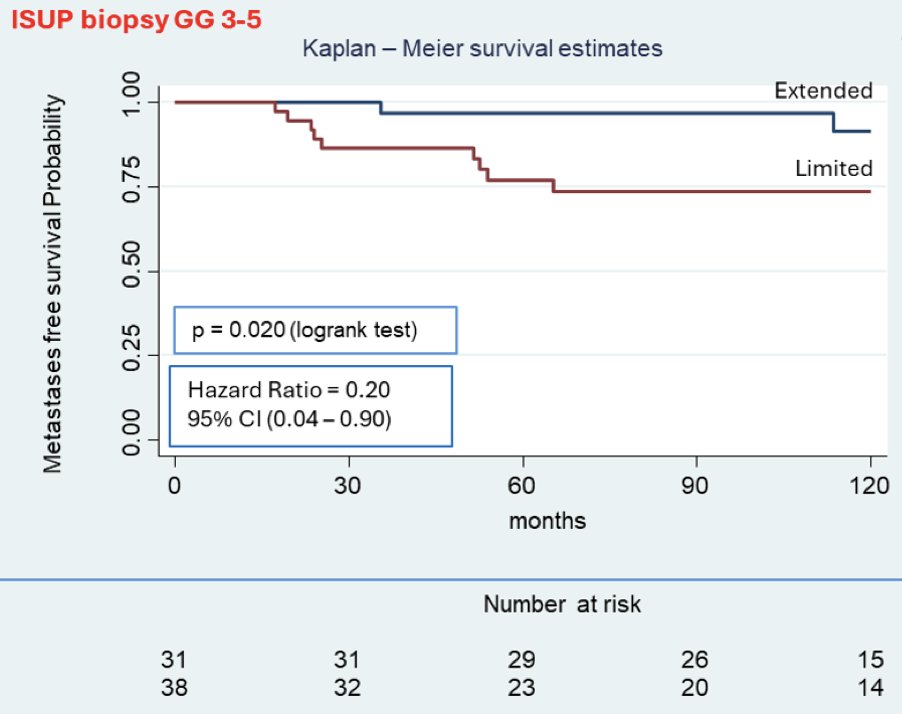
Additionally, in this high-grade subgroup, a significant improvement in metastasis-free survival was also observed with extended pelvic lymphadenectomy (HR 0.2, 95% CI 0.04–0.9; p = 0.020; number needed to treat = 7) with extended follow-up:
Dr. Ruggeri concluded this presentation discussing a 10-year follow-up of a phase 3 trial assessing extended versus limited pelvic lymph node dissection during radical prostatectomy for intermediate- and high-risk prostate cancer with the following take-home points:
- This long-term randomized phase 3 trial did not demonstrate oncologic superiority of extended pelvic lymphadenectomy over limited pelvic lymphadenectomy in unselected intermediate- and high-risk prostate cancer
- However, in patients with biopsy ISUP grade 3–5, long-term follow-up showed a significant benefit in biochemical recurrence-free survival and metastasis-free survival, suggesting that extended pelvic lymphadenectomy should be the standard of care in this subgroup undergoing radical prostatectomy
Presented by: Matheus Ruggeri, MD, Universidade de São Paulo, Urology, São Paulo, Brazil
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.