(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a late-breaking abstracts session and a presentation by Dr. Laurence Klotz discussing initial perioperative outcomes of CAPTAIN, a randomized controlled trial evaluating MRI-guided TULSA (Transurethral Ultrasound Ablation) versus robotic prostatectomy. MRI-guided TULSA delivers directional thermal ultrasound under real-time MRI thermometry control to precisely treat prostate tissue while sparing genitourinary function:

Previous randomized controlled trials comparing standard prostate cancer treatments to ablation have failed to recruit due to poor acceptance of randomization, and do not directly compare functional and oncological outcomes as primary endpoints. CAPTAIN is the first multicenter randomized clinical trial in this space to enroll to target, comparing MRI-guided TULSA to robotic prostatectomy for intermediate-risk prostate cancer. At EAU 2026, Dr. Klotz and colleagues compared procedural outcomes, recovery to baseline activities, and early functional recovery (pad-free urinary continence) in the CAPTAIN trial.
Eligible patients had primary localized ISUP 2/3 prostate cancer and PSA ≤ 20 ng/mL. Exclusions include contraindication to MRI or robotic prostatectomy and calcifications ≥3mm obstructing the ultrasound beam. CAPTAIN accrued from 4 countries, at 18 sites, and included 27 investigators. Robotic prostatectomy ± pelvic lymph node dissection followed local standard of care, and ablation plans ranged from hemi- to whole-gland with strategic sparing. Treatment/peri-procedural data collected included estimated blood loss, rate of pelvic lymph node dissection (robotic prostatectomy), ablation fraction (TULSA), length of stay, and catheterization duration. EQ-5D-5L assessed recovery of baseline activity and overall health, and pad-free continence was assessed by EPICQ5. The schema for the CAPTAIN trial is as follows:

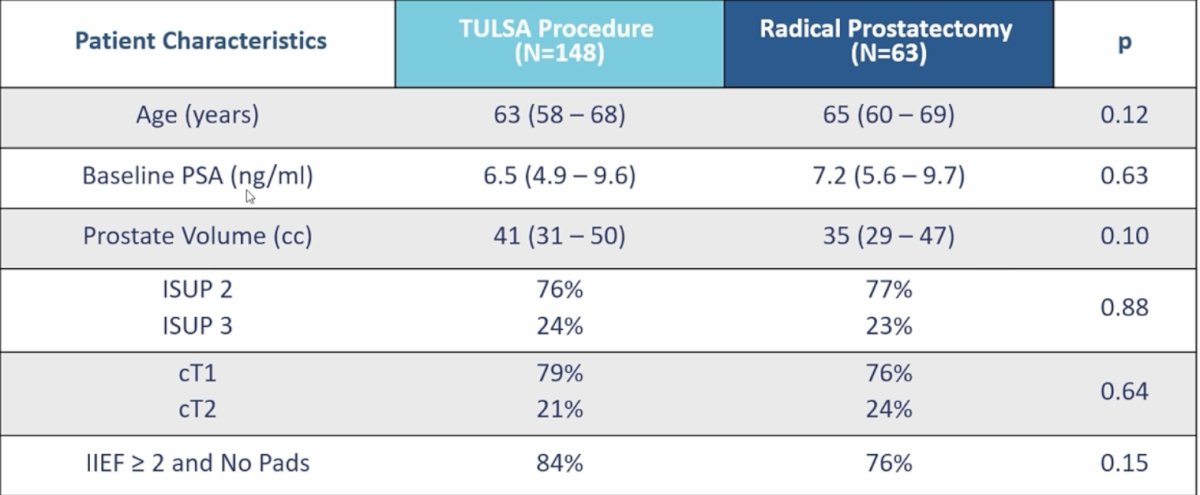
There were 148 patients randomized to the TULSA arm and 63 patients to the robotic prostatectomy arm. The median age for TULSA versus robotic prostatectomy was 63 (IQR 58-68) versus 65 (IQR 60-69) years (p = 0.12), PSA 6.5 (IQR 4.9-9.6) ng/mL versus 7.2 (IQR 5.6-9.7) ng/ml (p = 0.63), and gland volume 41 (IQR 31-50) cc versus 35 (IQR 29-47) cc (p = 0.10). Proportions with ISUP2/3 prostate cancer were 76%/24% versus 77%/23% (p = 0.88), for TULSA versus robotic prostatectomy:
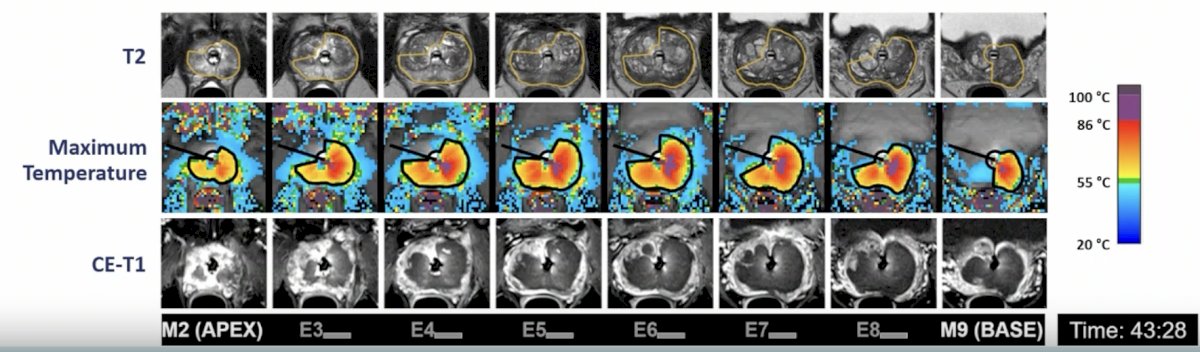
The median fraction of the gland reaching ablative temperatures on intra-procedural MRI thermometry was 78% (IQR 71-85), with 68% of cases comprising whole gland ablation and 32% sub-total ablation:
Surgically, nerve sparing was performed in 95% of cases (89% bilateral, 6% unilateral), and 77% of patients had a pelvic lymph node dissection. There was less intra-procedural blood loss (0 [IQR 0-0] versus 150 [IQR 100-200] mL) and shorter stay after TULSA (0.3 [IQR 0.2-0.3] versus 1.1 [IQR 1.1-1.3] days); both p < 0.001, but longer catheterization duration: 13 (IQR 11-15) versus 8 (IQR 8-10) days, p < 0.001. TULSA had reduced pain in the first week after treatment. There was less decline in EQ-5D overall health after TULSA versus robotic prostatectomy for all 30 days, and greater ability to perform usual activities for 9 days:
![Surgically, nerve sparing was performed in 95% of cases (89% bilateral, 6% unilateral), and 77% of patients had a pelvic lymph node dissection. There was less intra-procedural blood loss (0 [IQR 0-0] versus 150 [IQR 100-200] mL) and shorter stay after TULSA (0.3 [IQR 0.2-0.3] versus 1.1 [IQR 1.1-1.3] days); both p < 0.001, but longer catheterization duration: 13 (IQR 11-15) versus 8 (IQR 8-10) days, p < 0.001. TULSA had reduced pain in the first week after treatment. There was less decline in EQ-5D overall health after TULSA versus robotic prostatectomy for all 30 days, and greater ability to perform usual activities for 9 days:](/images/com-doc-importer/252-eau-2026/eau-2026-captain-randomized-controlled-trial-evaluating-mri-guided-tulsa-versus-robotic-prostatectomy---initial-perioperative-outcomes/image-4.jpg)
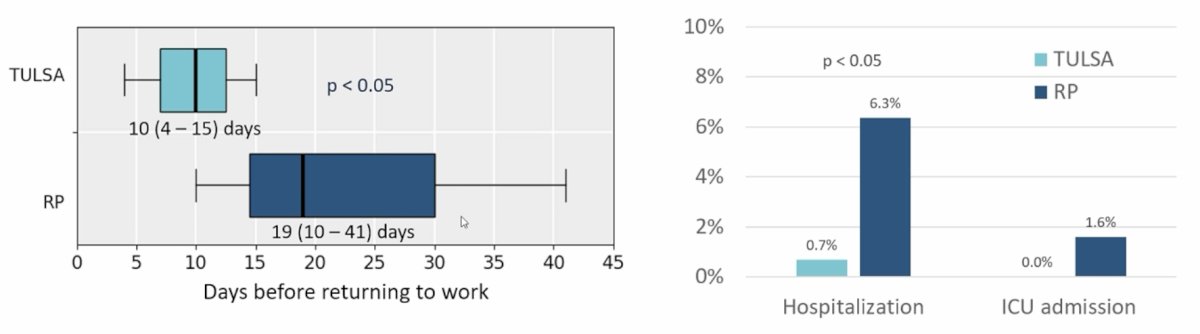
Between 30-90 days of recovery, there was significantly less time missed from paid employment within 30 days for TULSA versus robotic prostatectomy, and fewer admissions to the hospital or ICU for complications:
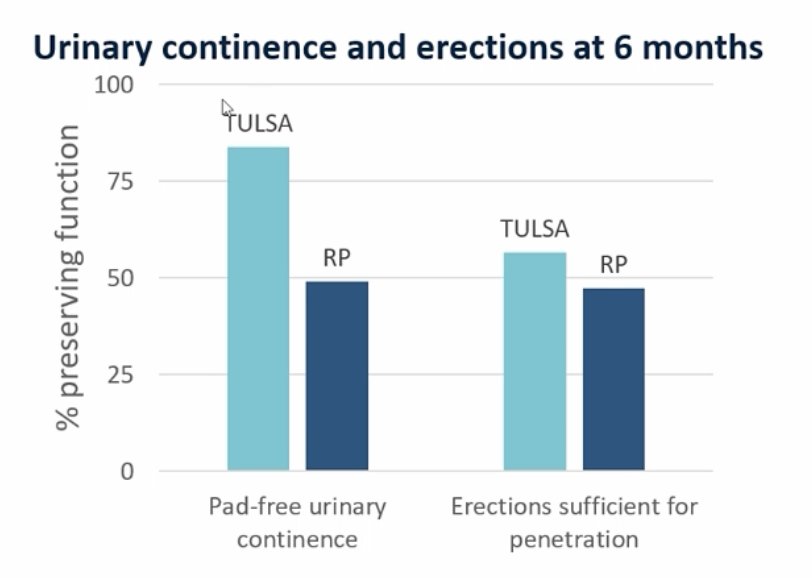
The primary safety endpoint at 6 months was preservation of EPIC pad-free continence and IIEF Q2 erections sufficient for penetration. The primary composite endpoint was 50% for TULSA versus 24% for robotic prostatectomy (RR 2.1, p <0.05):
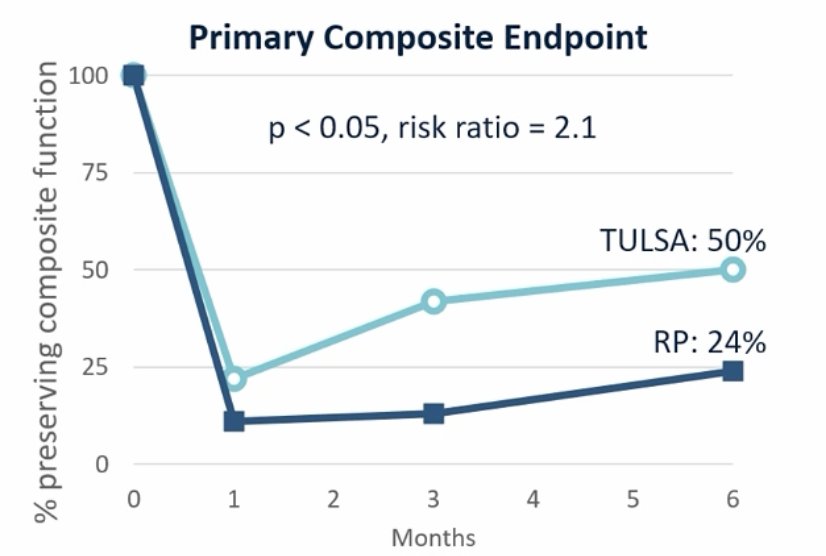
As follows is the bar graph for urinary continence and erections at 6 months between the two groups:
Secondary oncological outcomes included surgical pathology after radical prostatectomy, noting that 63% were pT2, 30% pT3a, and 5% T3b, with 33% of patients having positive margins. TULSA histology and imaging are awaiting the 12-month MRI + biopsy, and biochemical and clinical progression are pending additional follow-up.
Dr. Klotz concluded his presentation discussing initial perioperative outcomes of the CAPTAIN trial with the following take-home points:
- CAPTAIN is the first fully-enrolled phase 3 multicenter randomized clinical trial directly comparing functional and oncologic outcomes of ablation versus prostatectomy
- TULSA was superior for the primary safety endpoint at 6 months (similar to the TULSA single-arm pivotal registration study)
- TULSA was superior for secondary measures of recovery:
- Zero blood loss, no overnight stay, reduced post-procedure pain
- Faster recovery to work and daily activities, improved patient-reported overall health
- Fewer complications requiring hospitalization
- The primary oncologic endpoint (freedom from additional prostate cancer treatment) is to be reported at 3 years
- Follow-up will continue for 10 years
Presented by: Laurence H. Klotz, MD, FRCSC, University of Toronto, Toronto, Ontario, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.