(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a plenary prostate cancer session and a presentation by Dr. Renu Eapen discussing the optimal management of de-novo oligometastatic disease and whether we always need PSMA PET/CT in this setting. Dr. Eapen’s discussion was based on a prior case presentation of a 52 year old fit man with ISUP 5 oligometastatic prostate cancer (cT1cN0M1) on conventional imaging. Rather than the title of her talk being “can’t say we always need PSMA PET/CT imaging in this setting”, Dr. Eapen argues that it should be “we ALWAYS need PSMA PET/CT imaging in this setting.” The concept of oligometastatic prostate cancer is to identify all disease, followed by ablation of all lesions, aiming for a cure of oligometastatic prostate cancer. As such, oligometastatic prostate cancer is a function of imaging sensitivity.
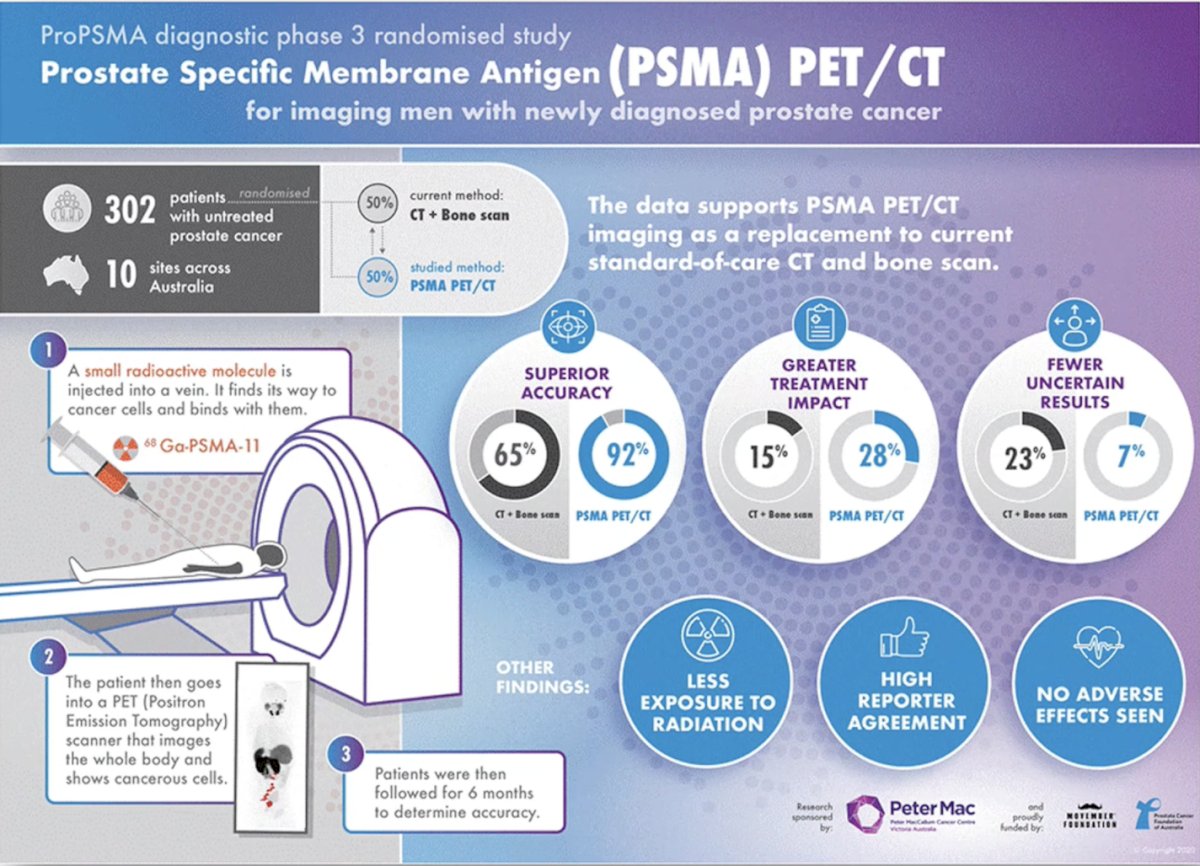
Dr. Eapen then discussed the proPSMA trial,1 a multi-center randomized controlled trial of men with histologically confirmed prostate cancer who were being considered for curative intent radical prostatectomy or radiotherapy. All patients had at least one high-risk factor, including serum PSA ≥ 20 ng/mL, Grade Group 3 to 5 disease, or clinical stage T3 or greater. Following enrollment, patients were randomly assigned in a 1:1 ratio to either conventional imaging consisting of bone scan and CT or 68Ga-PSMA-11 PET/CT. Between 2017 and 2018, 302 patients were randomized to either conventional imaging (n = 152) or 68Ga-PSMA-11 PET/CT (n = 150). PSMA PET/CT demonstrated a 27% absolute greater AUC for accuracy compared to conventional imaging (92% versus 65%) for the detection of either pelvic nodal or distant metastatic disease. Conventional imaging had both a lower sensitivity (38% versus 85%) and specificity (91% versus 98%). Subgroup analyses by site of metastasis demonstrated the superiority of PSMA PET/CT for pelvic nodal (AUC: 91% versus 59%) and distant metastases (AUC: 95% versus 74%):
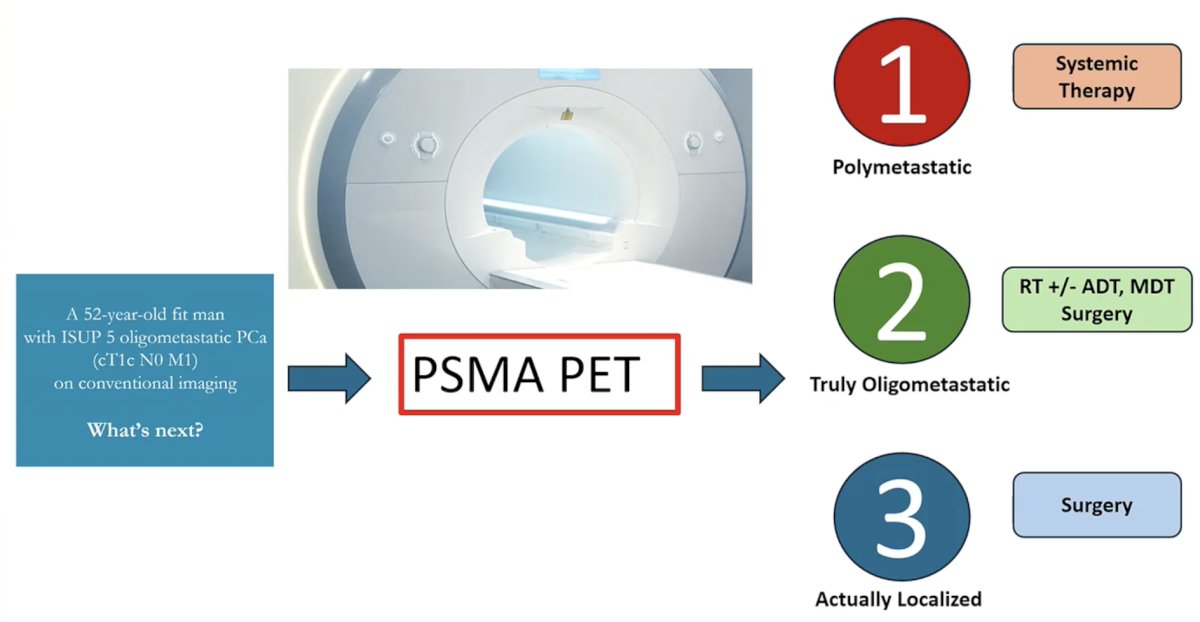
Dr. Eapen notes that there are 3 different scenarios for these patients after PSMA PET/CT imaging. The first is that the patient has polymetastatic disease, the second is that they truly do have oligometastatic disease, and the third is that the patient is downstaged from M1 to M0. Based on these assessments, she concluded her presentation by highlighting that PSMA PET allows polymetastatic patients to receive systemic therapy, truly oligometastatic patients to receive radiotherapy +/- ADT, metastasis directed therapy, or surgery, and localized patients to receive surgery:
Presented by: Renu Eapen, MBBS, FRACS, Peter MacCallum Cancer Centre, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Hofman MS, Lawrentschuk N, Francis, RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomized, multicentre study. Lancet 2020 Apr 11;395(10231):1208-1216.