(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a managing advanced disease in renal and rare cancer session and a presentation by Dr. Fernando Maluf discussing ongoing trials in rare genitourinary cancers. There are numerous barriers to rare genitourinary tumors, including:
- Geographical variations
- Lack of guidelines
- Unconventional therapies
- Low incidence
- Limited funding opportunities
- Pathology unrecognition
- Slow trial accrual
- Patient psychological barriers
- Entity heterogeneity
- Multidisciplinary treatment required
- Delayed diagnosis
- Lack of expertise
- Unfavorable performance status and nutrition status
Dr. Maluf emphasized that his discussion would focus on penile squamous cell carcinoma and genitourinary basket trials.
At ASCO 2024, Dr. Maluf presented the HERCULES (LACOG 0218), a phase II trial of pembrolizumab + platinum-based chemotherapy as first-line systemic therapy in advanced penile cancer. Patients with metastatic or locally advanced disease (recurrent or TanyN3M0 or T4NanyM0) not amenable to curative-intent therapy received 5-FU 1000 mg/m²/day IV D1-D4 + cisplatin 70mg/m² (or carboplatin AUC 5) IV D1 + pembrolizumab 200mg IV D1 every 3 weeks for 6 cycles, followed by pembrolizumab 200mg IV every 3 weeks up to 34 cycles. The trial design is as follows:
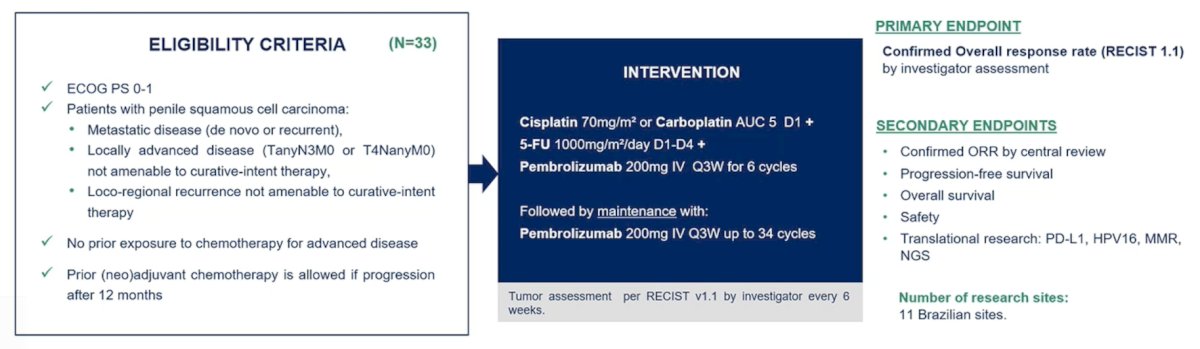
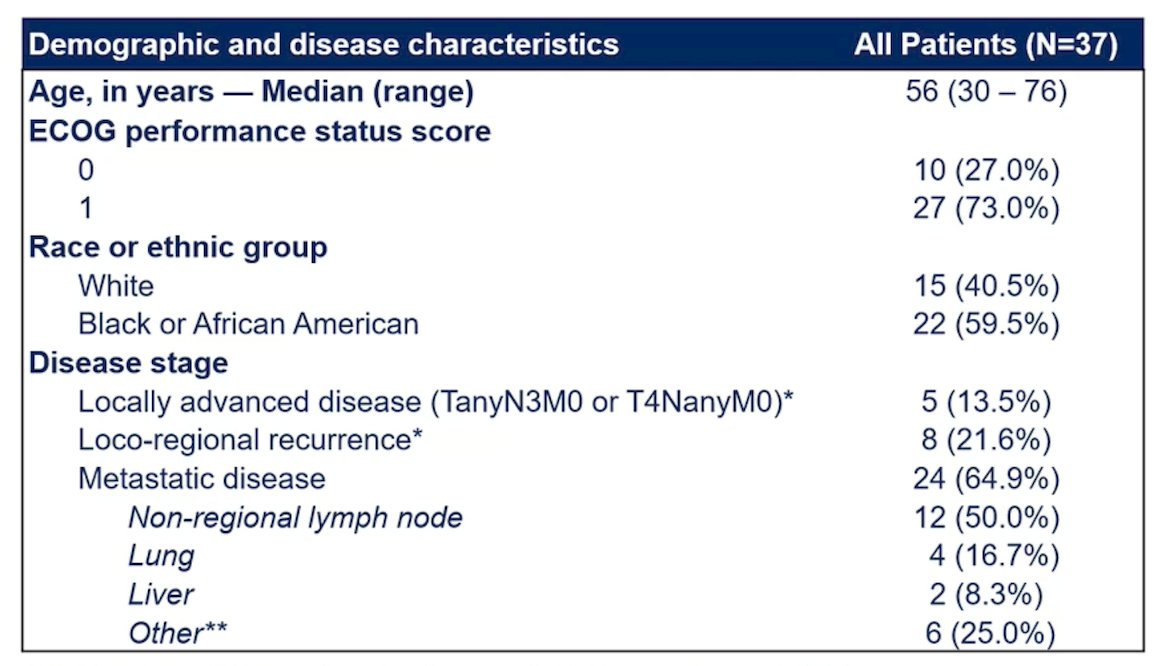
The primary endpoint is confirmed overall response rate assessed by the investigator according to RECIST 1.1. From August 2020 to December 2022, 37 patients were enrolled in 11 Brazilian centers, and 33 patients were eligible for efficacy analysis. The median age was 56 years (range: 30-76), 64.9% of patients had metastatic disease, 21.6% had recurrent disease, and 13.5% had locally advanced disease:
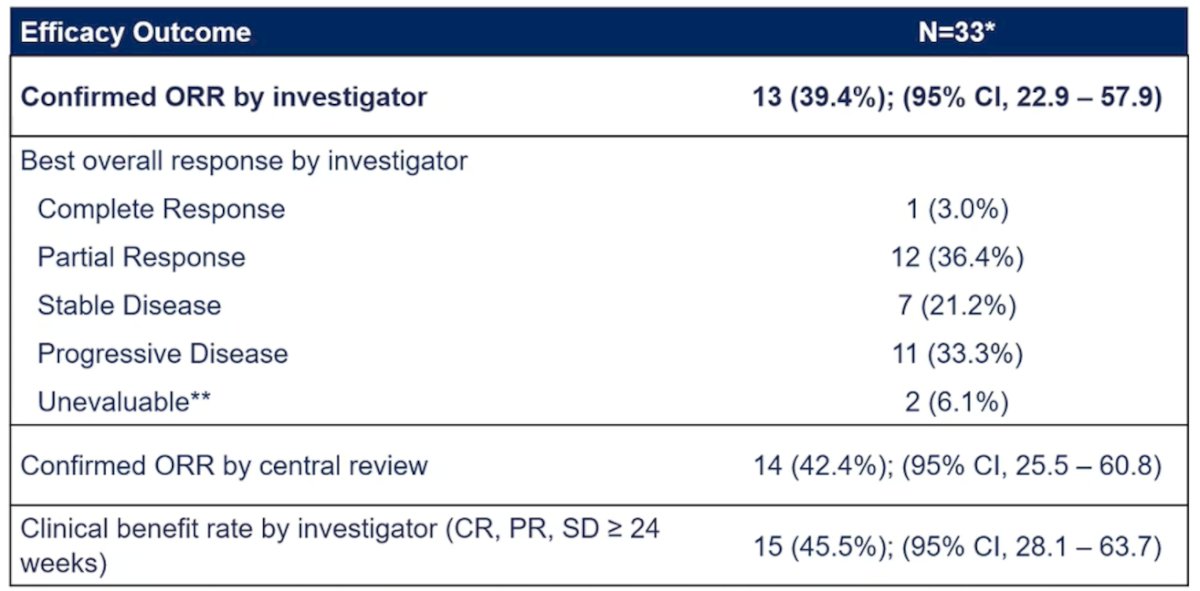
The confirmed overall response rate by investigator was 39.4% (95% CI 22.9-57.9%), with 1 complete response and 12 partial responses:
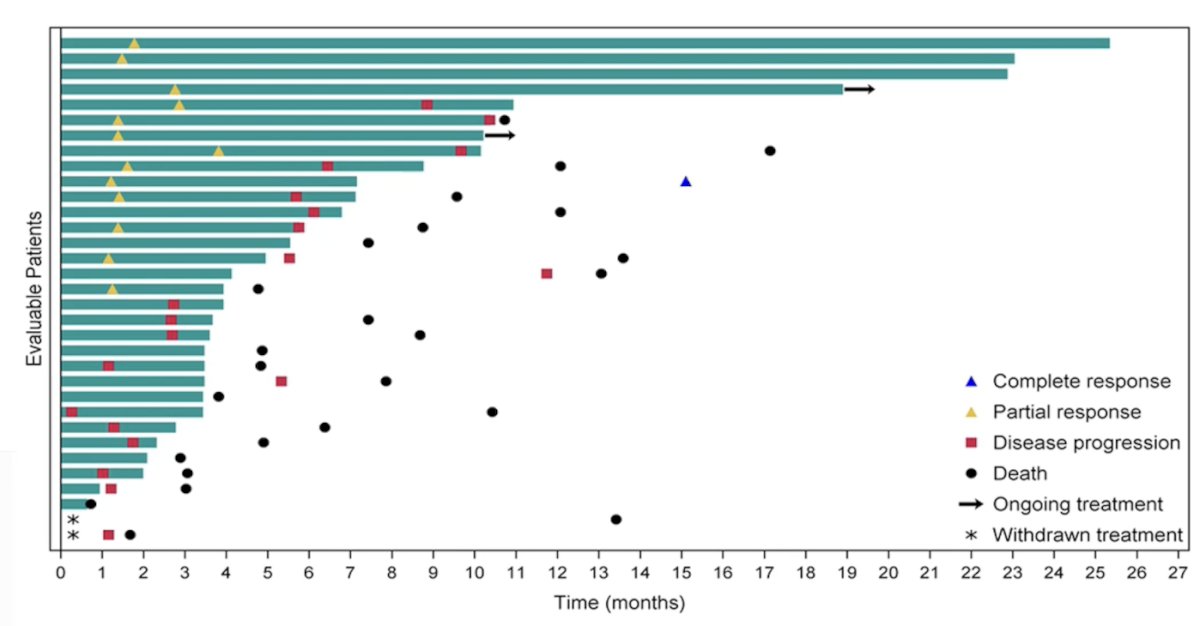
Tumor shrinkage of any magnitude was observed in 75.8% of patients:

The median duration of response was 5.9 months (95% CI 4.4-9.0), the median time to response was 1.4 months (95% CI 1.3-1.8), and the median follow-up was 24.0 months (95% CI 13.5-26.4):
The conclusions from the HERCULES trial were as follows:
- HERCULES met its primary endpoint of confirmed objective response rate of 39.4% by investigator assessment, which increased to 42.4% by central review
- HPV16-positive patients had a confirmed objective response rate of 55.6% and TMB-high 75%, which are potential biomarkers for efficacy with chemotherapy + immune checkpoint inhibitors in advanced penile squamous cell carcinoma
- This is the first trial to demonstrate the efficacy of immune checkpoint inhibitors in advanced penile squamous cell carcinoma with a manageable safety profile
- Pembrolizumab + platinum-based chemotherapy is a new treatment option for advanced penile squamous cell carcinoma
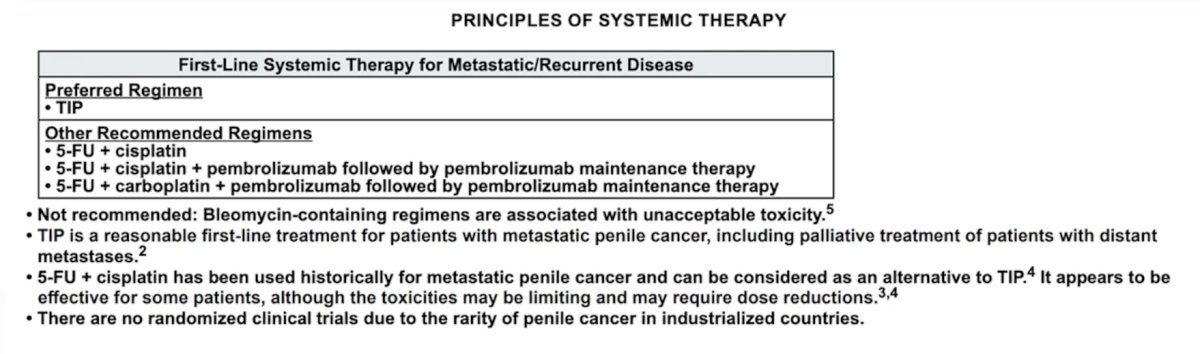
Based on the results of the HERCULES trial, the NCCN Guidelines Version 1.2025 for Penile Cancer added pembrolizumab to other recommended regimens:
Dr. Maluf then discussed several ongoing trials for penile squamous cell carcinoma, starting with the neoadjuvant space. The PRIAM trial is assessing carboplatin + paclitaxel + pembrolizumab for locoregionally advanced penile cancer, whereby 50 patients will receive neoadjuvant carboplatin + paclitaxel + pembrolizumab followed by surgery, followed by 7 cycles of adjuvant pembrolizumab. The primary endpoint is pathological complete response:

The InPACT trial will include men with biopsy-proven squamous cell carcinoma of the penis, clinical T any, N1-N3, and with measurable disease by RECIST criteria (>= 1.5 cm short axis diameter). The multi-arm InPACT trial design is as follows:
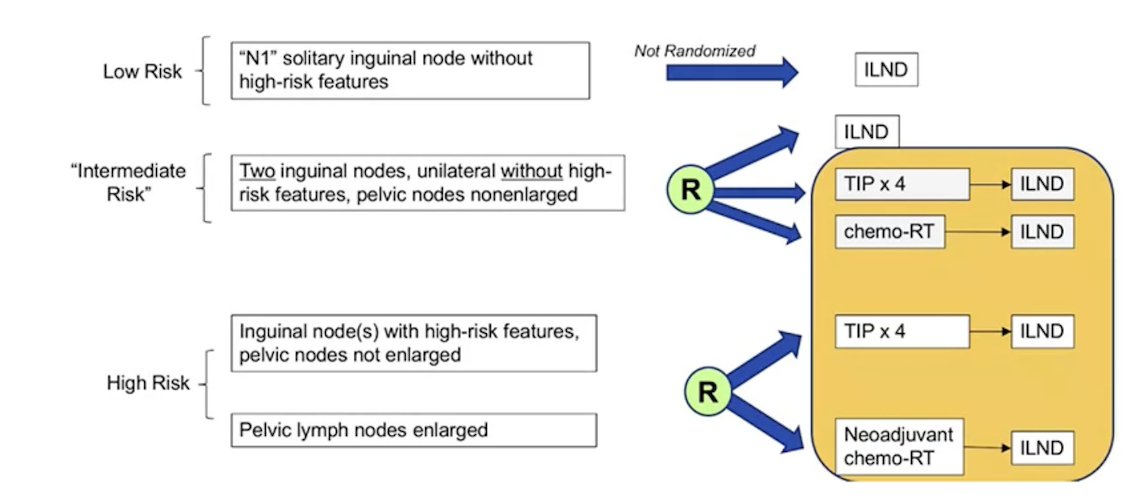
The primary endpoint of InPACT is overall survival, and the trial is now nearly fully accrued.
In the metastatic/recurrent first-line space, Dr. Maluf discussed a trial assessing enfortumab vedotin for the treatment of patients (n = 28) with metastatic or unresectable penile squamous cell carcinoma, with a primary endpoint of best response rate:

The DEPECA-1 trial is a phase II study evaluating first-line therapy with enfortumab vedotin + avelumab for advanced or metastatic penile carcinoma. Patients must not have had prior chemotherapy, with a planned accrual of 25 patients:

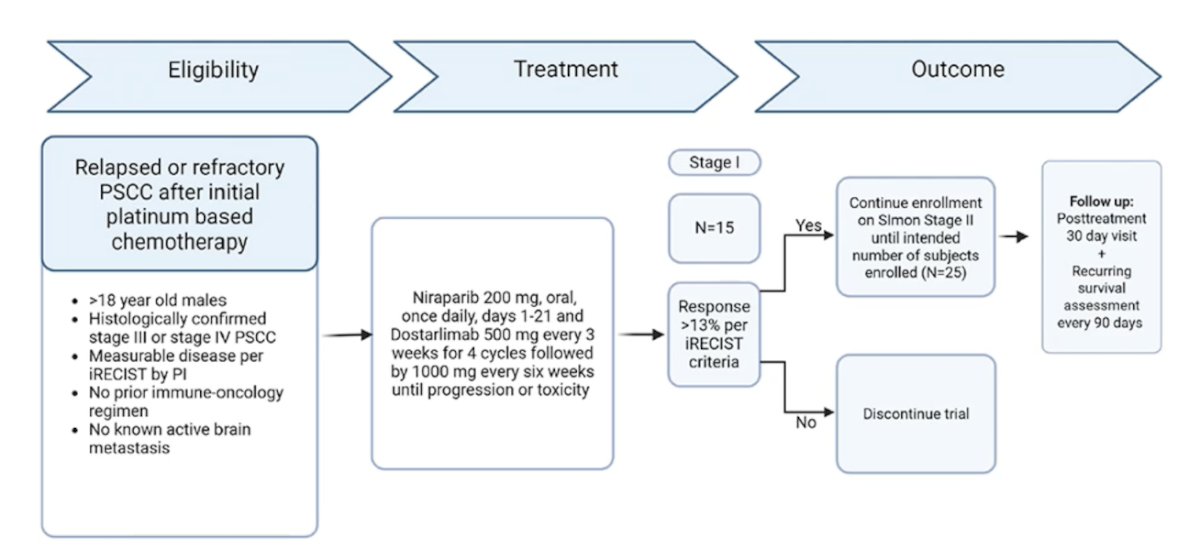
Third, 15 patients with advanced penile squamous cell carcinoma will be treated with combination dostarlimab + niraparib with a goal of >13% response per iRECIST criteria in order to continue enrollment on Simon Stage II (n = 25):
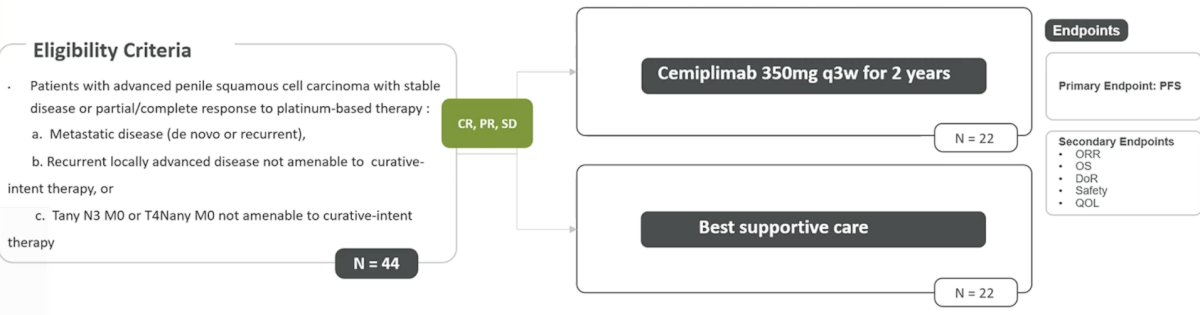
The BRAVA trial in Brazil, led by Dr. Maluf, is a phase II randomized trial of maintenance cemiplimab versus best standard of care in patients with metastatic/recurrent penile squamous cell carcinoma who had controlled disease on first-line platinum-based chemotherapy. There will be 44 patients randomized with a primary endpoint of progression-free survival:
The Desired Trial is a global HERCULES II study whereby immune checkpoint inhibitors will be combined with platinum-based chemotherapy versus platinum-based chemotherapy alone as first-line systemic therapy in advanced penile cancer (PI: Dr. Maluf). HERCULES II will randomize 186 patients with a primary endpoint of overall survival:
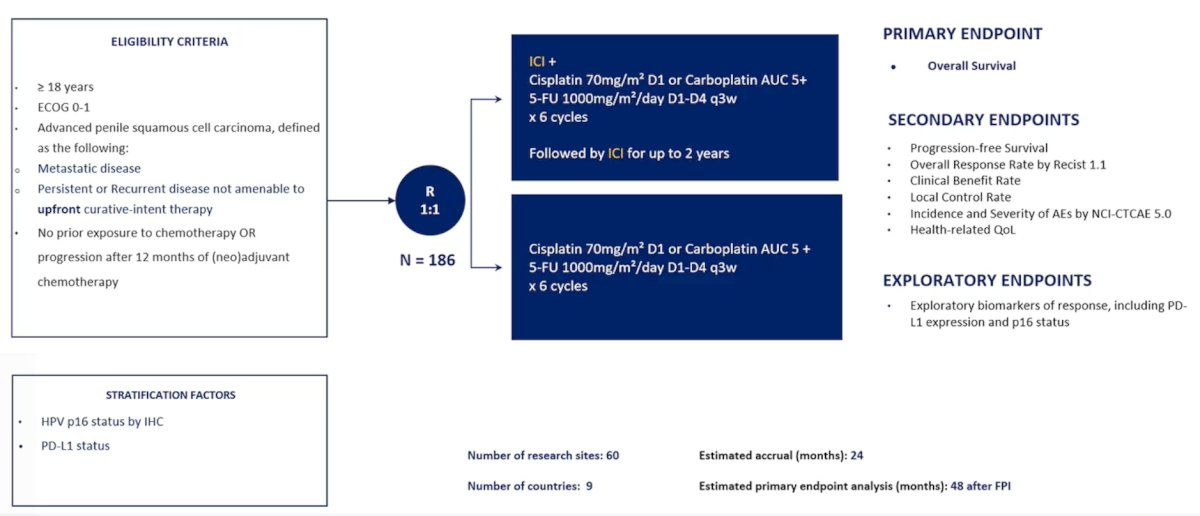
Potential countries include Brazil and other Latin American countries, the USA, France, and Italy.
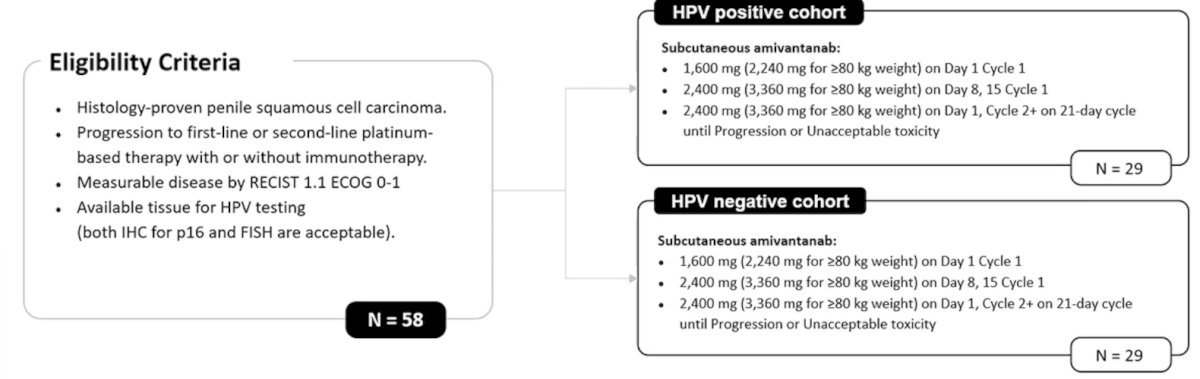
Moving to the metastatic/recurrent second-line space, Dr. Maluf discussed a trial he is PI of, the APOLO trial. This trial will assess amivantamab among 58 penile squamous cell carcinoma patients that progressed on first-line platinum-based chemotherapy. The primary endpoint is objective response rate by investigator assessment:
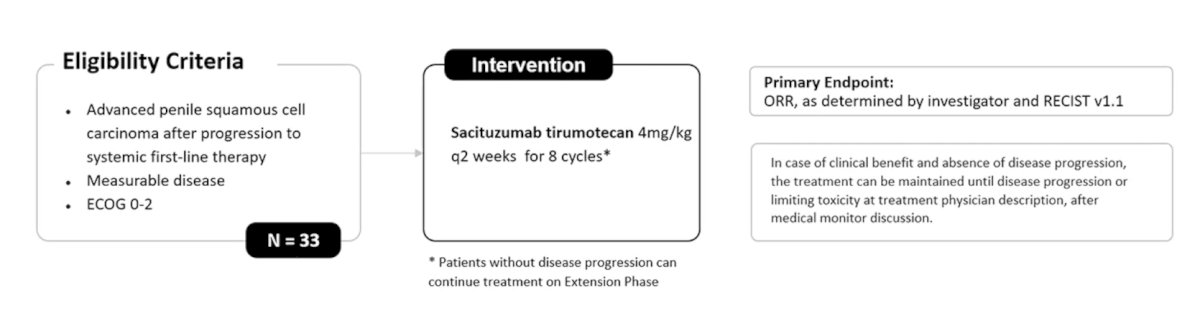
The PERSEUS trial (PI: Dr. Maluf) is a single-arm phase II trial of sacituzumab tirumotecan as second-line treatment, with a targeted accrual of 33 patients, and a primary endpoint of objective response rate by investigator assessment:
Finally, Dr. Maluf discussed several ongoing, key basket trials. SMART is a phase 2 study of sacituzumab govitecan with or without atezolizumab in rare genitourinary tumors (adenocarcinoma of the urinary tract, neuroendocrine carcinoma of the urinary tract, squamous cell carcinoma of the urinary tract, penile squamous cell carcinoma, and renal medullary carcinoma). Patients will either receive sacituzumab govitecan alone (if they previously received PD-1/PD-L1 immune checkpoint inhibitor) or in combination with atezolizumab. The primary endpoint is objective response rate:

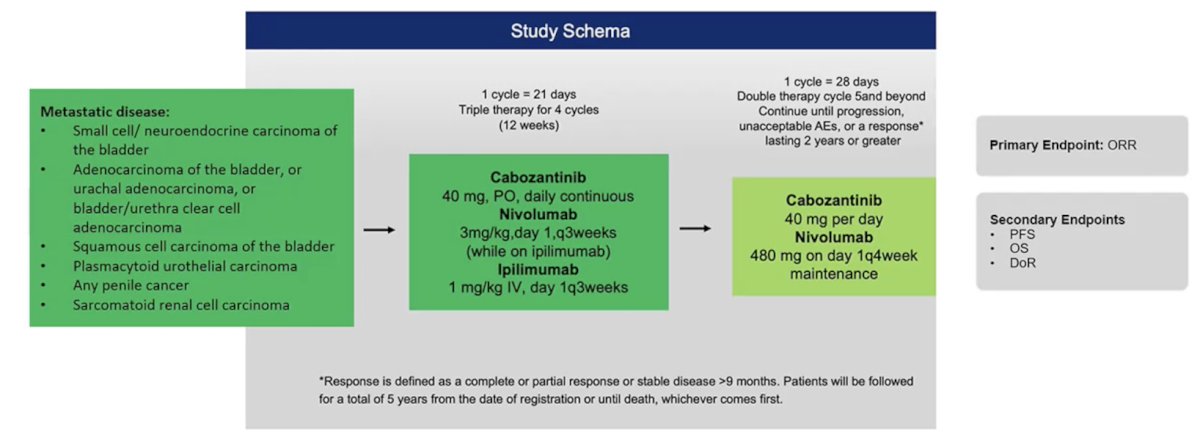
Another basket trial is assessing the effectiveness of two immunotherapy drugs (nivolumab + ipilimumab) with an anti-cancer targeted drug (ie, cabozantinib) for rare genitourinary tumors. Inclusion includes metastatic small cell/neuroendocrine, adenocarcinoma, squamous cell carcinoma, and plasmacytoid of the urinary tract, any penile cancer, and sarcomatoid renal cell carcinoma. The primary endpoint is objective response rate:
Dr. Maluf concluded his presentation discussing ongoing trials in rare genitourinary cancers with the following take-home points:
- Rare genitourinary tumors have a high unmet clinical need
- Active clinical trials are available and should be prioritized
- Clinical trials should focus on high-prevalence geographical areas (such as penile cancer)
- Early referral to expert centers improves access to care and outcomes
- Global collaboration is key to real and solid advances in this field
Presented by: Fernando Cotait Maluf, Associate Director, Oncology Center, Beneficência Portuguesa, São Paulo, Comittee Member, Oncology Center, Hospital Albert Einstein, São Paulo, LACOG Steering Comittee Member, Sāo Paulo, Brazil
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.