(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a game changer session and a presentation by Dr. Thomas Powles discussing primary and exploratory efficacy outcomes from the phase 3 LITESPARK-022 study assessing adjuvant pembrolizumab + belzutifan for clear cell RCC. Adjuvant pembrolizumab improved disease free survival and overall survival versus placebo in the phase 3 KEYNOTE-564 trial.1,2 However, efficacy may be further improved with combination therapy in this setting, given that ~40% of patients treated with adjuvant pembrolizumab experience recurrence or death within 5 years of nephrectomy. Belzutifan is a potent, selective HIF-2alpha inhibitor with established efficacy in patients with advanced RCC treated with prior immunotherapy and VEGFR-TKI therapy.3 The double-blind phase 3 LITESPARK-022 trial evaluated pembrolizumab + belzutifan versus pembrolizumab + placebo as adjuvant therapy in patients with clear cell RCC at increased risk of recurrence post nephrectomy.
Eligible patients for this trial had clear cell RCC stage M0 and intermediate-high (pT2 grade 4 or sarcomatoid, or pT3 any grade, N0) or high (pT4 any grade, N0, or any pT/grade, N+) risk of recurrence after nephrectomy, or clear cell RCC stage M1 with no evidence of disease after surgery. Patients were randomized 1:1 to pembrolizumab 400 mg Q6W (≤9 doses) and either oral belzutifan 120 mg or placebo QD:
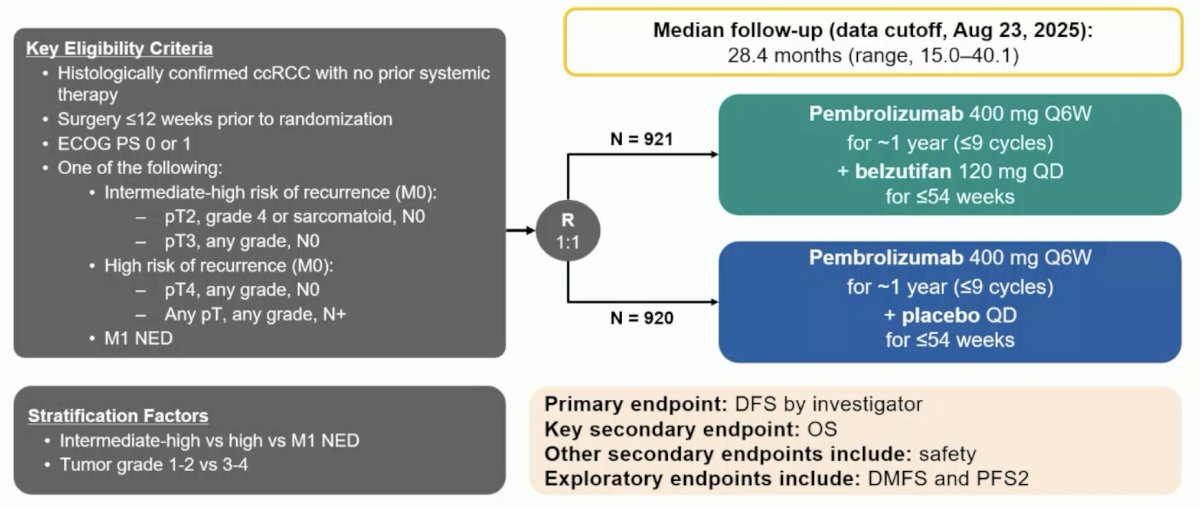
The primary endpoint was disease free survival by investigator, and secondary endpoints included overall survival (key secondary endpoint) and safety. Exploratory endpoints included distant metastasis free survival and progression free survival after next-line therapy. The enrollment plan was for 1,800 patients, with an actual enrollment of 1,841 patients. The primary endpoint of disease free survival was met at the first interim analysis. There were a planned ~396 disease free survival events and a minimum ~15 months after the last randomized participant, with an actual 432 disease free survival events and p value boundary of 0.01632. The median follow-up to data cutoff (August 23, 2025) was 28.4 months (range: 15.0 – 40.1), and overall survival was not significant at the first interim analysis. An alpha = 2.5% was passed to overall survival per rejection of the null hypothesis for disease free survival. There were 87 overall survival events (29% of the final analysis events) and actual p value boundary of 0.00003. At EAU 2026, Dr. Powles presented exploratory analyses for disease free survival in the presence and absence of sarcomatoid features, distant metastasis free survival, subsequent therapy, and progression free survival after next-line therapy.
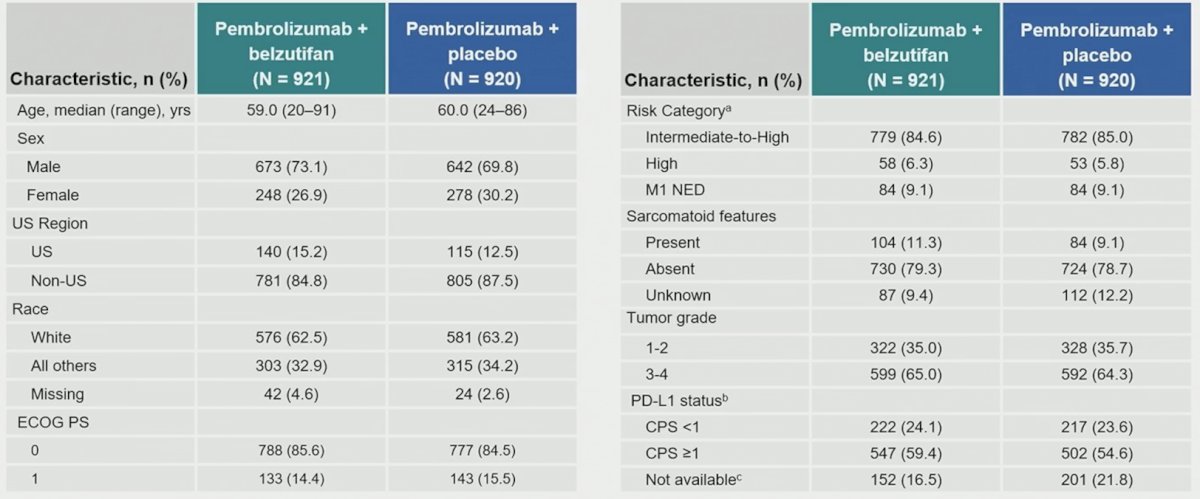
There were 921 patients assigned to pembrolizumab + belzutifan and 920 to pembrolizumab + placebo, and the baseline characteristics were well balanced between the two groups. Approximately 85% of patients were intermediate/high risk, and ~10% had sarcomatoid features:
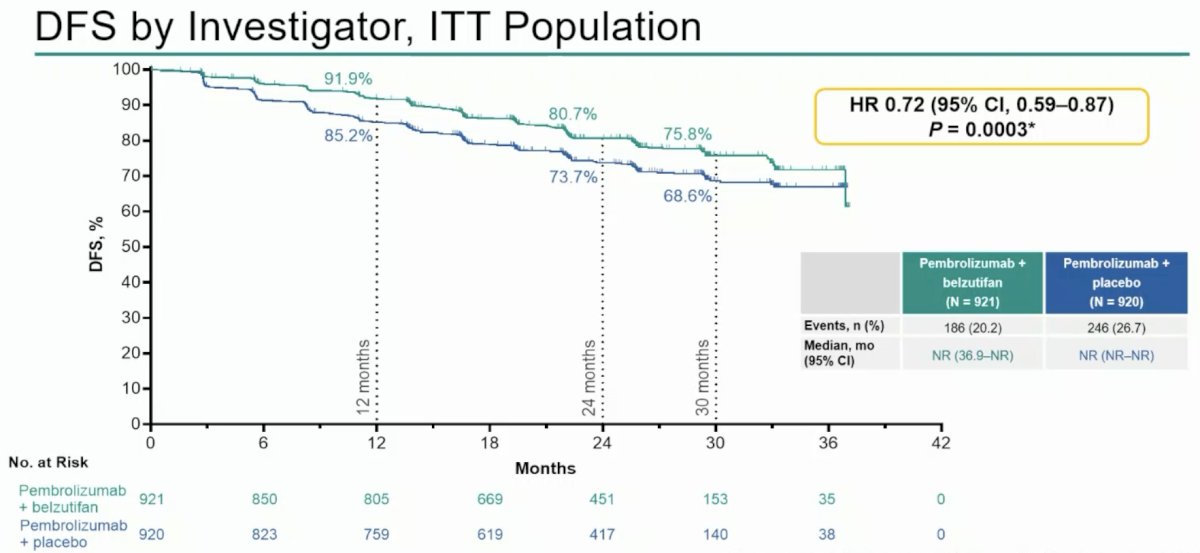
Presented by Dr. Choueiri at ASCO GU 2026, pembrolizumab + belzutifan significantly improved disease free survival versus pembrolizumab + placebo (HR 0.72, 95% CI 0.59–0.87; p = 0.0003), with the median disease free survival not reached in both arms. The estimated 24-month disease free survival rate was 80.7% (95% CI, 77.7–83.2) versus 73.7% (95% CI, 70.6–76.6), respectively:
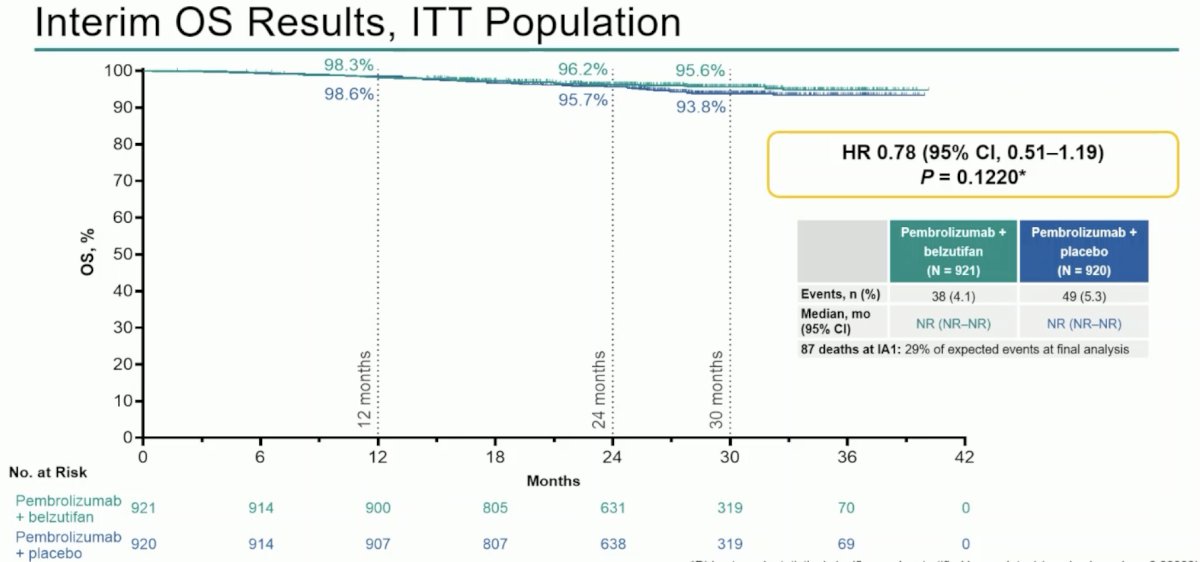
Overall survival was immature at the first interim analysis, with a total of 87 overall survival events (38 in the pembrolizumab + belzutifan arm versus 49 in the pembrolizumab + placebo arm) and did not reach statistical significance (HR 0.78, 95% CI 0.51–1.19; p = 0.1220) at 29% of the events needed for final overall survival analysis:
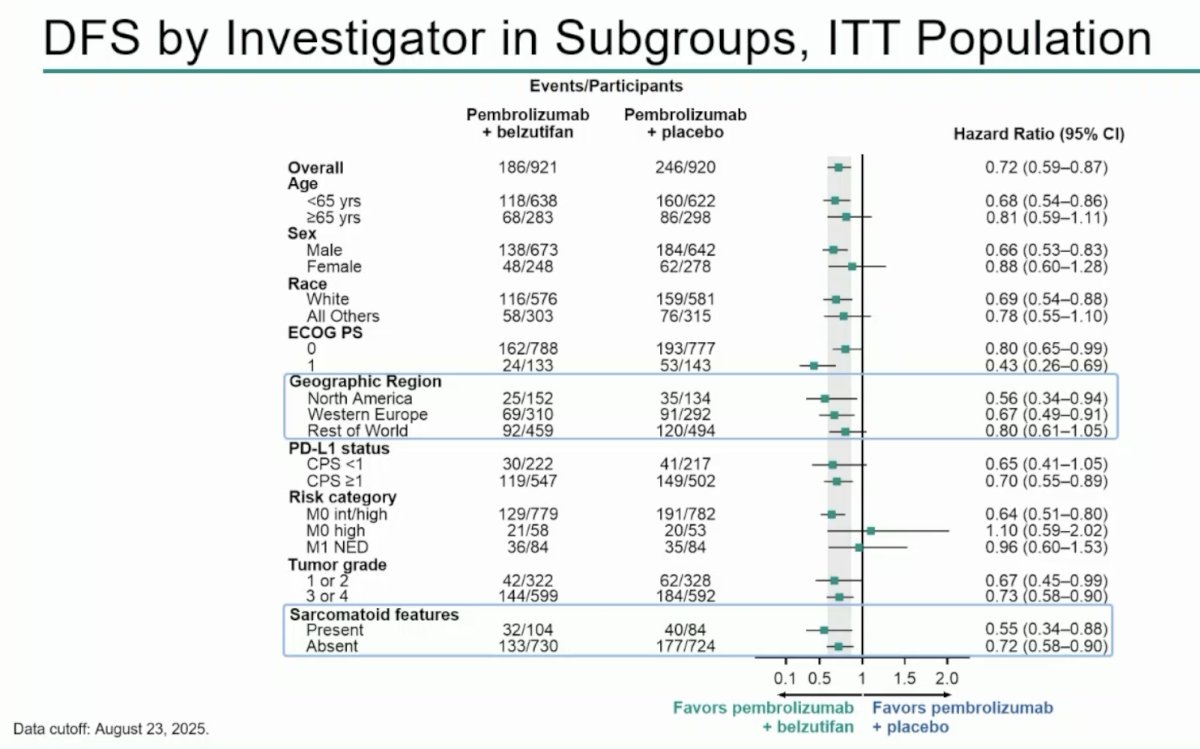
The disease free survival benefit of pembrolizumab + belzutifan generally favored all of the subgroups:
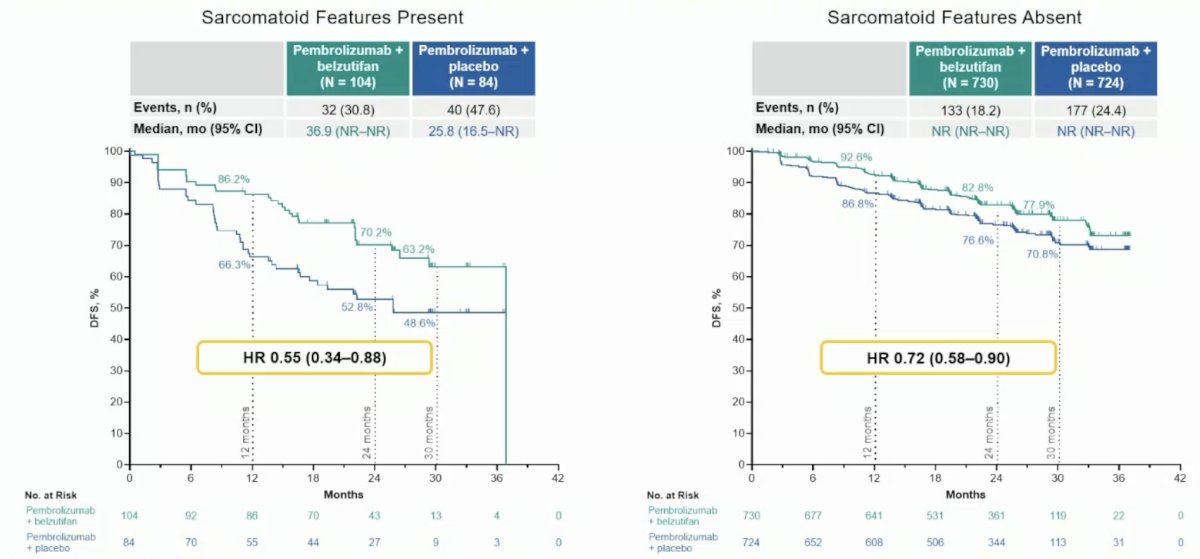
Disease free survival results by subgroups for patients with (HR 0.55, 95% CI 0.34-0.88) and without (HR 0.72, 95% CI 0.58-0.90) favored the pembrolizumab + belzutifan arm:
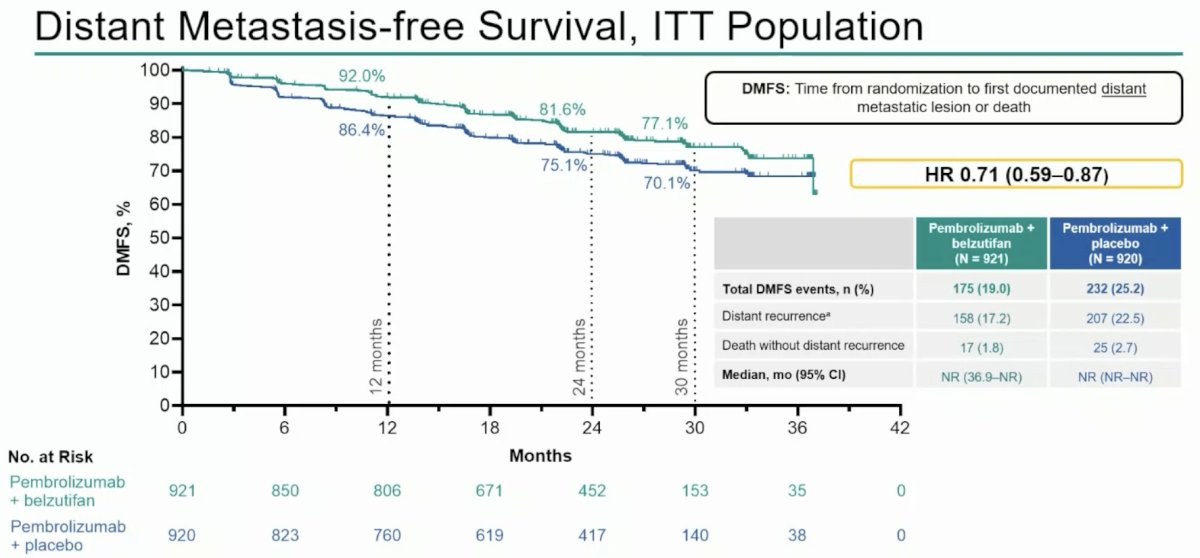
The median time to distant metastasis free survival was not reached in either arm, with a 24 month distant metastasis free survival rate of 81.6% for the pembrolizumab + belzutifan arm versus 75.1%in the pembrolizumab + placebo arm (HR 0.71, 95% 0.59-0.87):
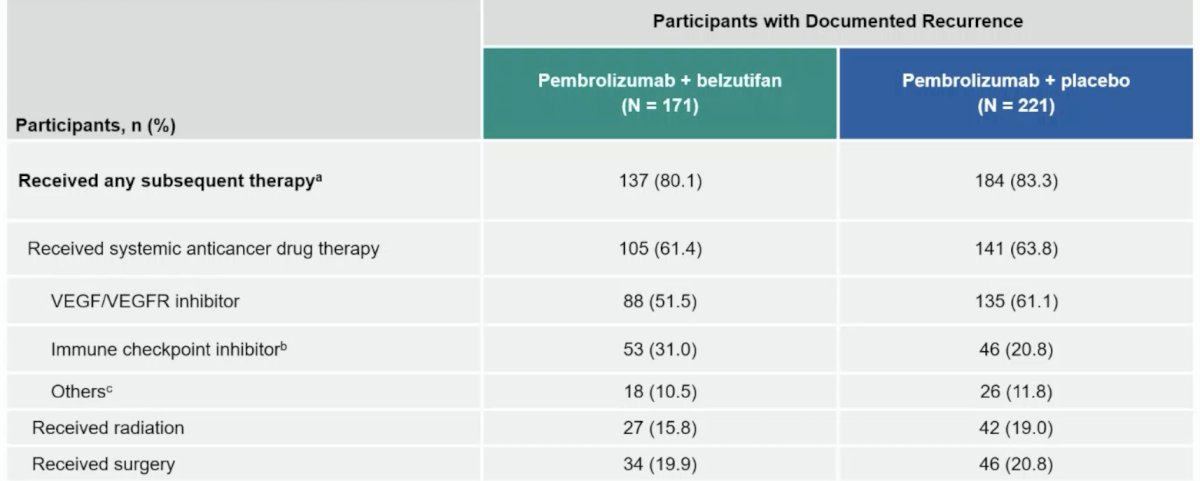
In terms of subsequent therapies in participants with recurrence, 80.1% of patients in the pembrolizumab + belzutifan arm and 83.3% in the pembrolizumab + placebo arm received a subsequent therapy, most commonly a VEGF/VEGFR inhibitor (51.5% versus 61.1%, respectively):
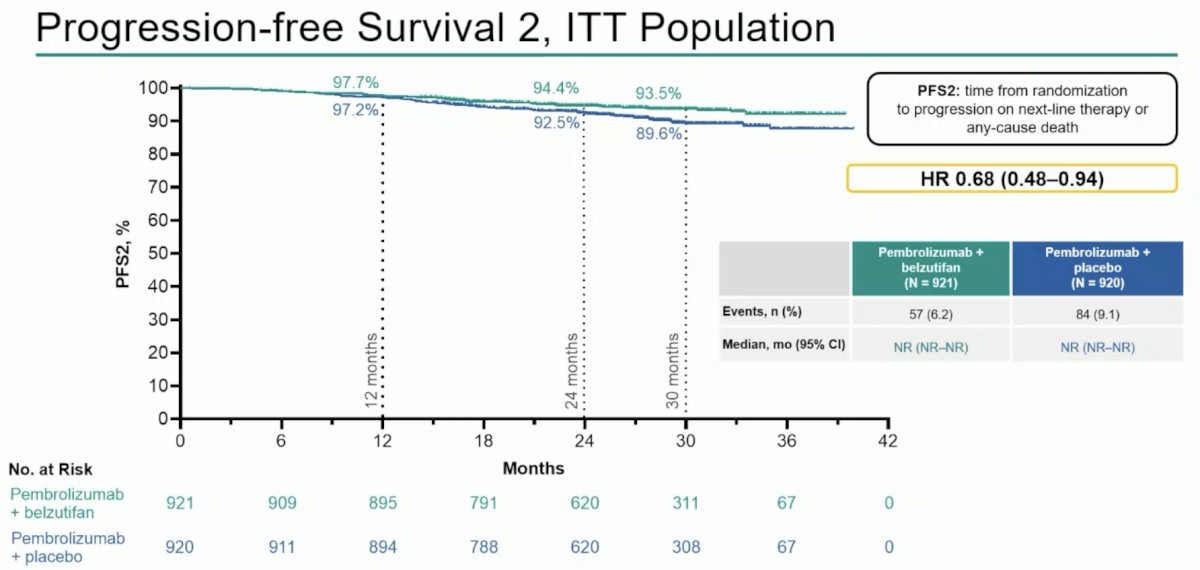
The median time to progression free survival after next-line therapy was not reached in either arm, with a 24 month progression free survival after next-line therapy rate of 94.4% for the pembrolizumab + belzutifan arm versus 92.5% in the pembrolizumab + placebo arm (HR 0.68, 95% 0.48-0.94):
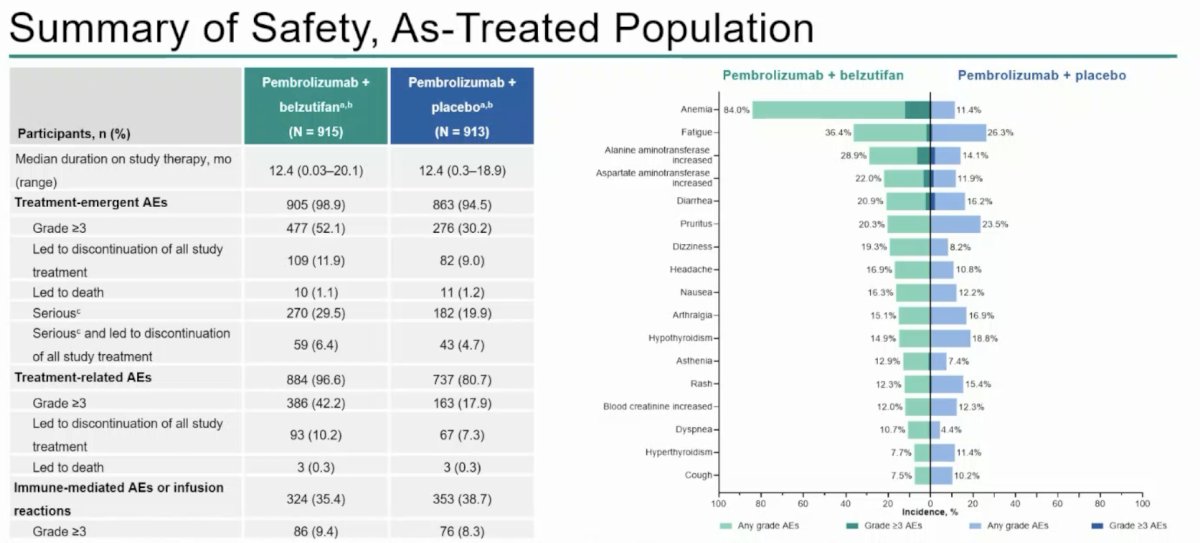
Among treated patients, grade ≥3 treatment emergent adverse events occurred in 52.1% of patients who received pembrolizumab + belzutifan and 30.2% who received pembrolizumab + placebo. The most common grade ≥3 treatment emergent adverse events were anemia (12.1% versus 0.4%), increased ALT (6.4% versus 2.0%), and hypoxia (4.6% versus 0%):
Dr. Powles concluded his presentation discussing primary and exploratory efficacy outcomes from the phase 3 LITESPARK-022 study with the following take-home points:
- LITESPARK-022 previously showed a statistically significant and clinically meaningful disease free survival improvement with adjuvant pembrolizumab + belzutifan versus pembrolizumab monotherapy in clear cell RCC at increased risk of recurrence post nephrectomy
– Additional follow-up is planned for overall survival
– The safety profile of pembrolizumab + belzutifan was consistent with expectations for each individual drug - At EAU 2026, the following results were reported for the first time:
– Disease free survival benefit with pembrolizumab + belzutifan was observed regardless of sarcomatoid feature presence
– Exploratory analyses of distant metastasis free survival and progression free survival after next-line therapy favored pembrolizumab + belzutifan compared with pembrolizumab + placebo
– Among participants with recurrence, most received subsequent systemic therapy; VEGF-targeted therapies were the most common type of subsequent systemic therapy received - LITESPARK-022 is the first positive phase 3 trial of adjuvant anti-PD-1 therapy combined with HIF-2α inhibition in RCC
– These results support adjuvant pembrolizumab + belzutifan as a standard of care within this setting
Presented by: Thomas Powles, MBBS, MRCP, MD, Barts Cancer Centre, London, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Choueiri TK, Tomczak P, Park SH, et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med. 2021 Aug 19;385(8):683-694.
- Choueiri TK, Tomczak P, Park SH, et al. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371.
- Choueiri TK, Powles T, Peltola K, et al. Belzutifan versus Everolimus for Advanced Renal-Cell Carcinoma. N Engl J Med. 2024 Aug 22;391(8):710-721.