(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a managing advanced disease in renal and rare cancer session and a Society of Urologic Oncology (SUO) lecture presentation by Dr. Brian Shuch discussing what the general urologist should know for rare renal tumors.
Kidney cancer is no longer just one disease. In 2014, the landscape included clear cell (~75%), papillary type 1 & 2 (16%), chromophobe (7%), and “other” (~2%), comprising translocation (1%), medullary (<0.5%), and collecting duct (<0.5%) histologies. Since then, our understanding of renal cell carcinoma has evolved, with the most recent WHO 2022 classification as follows:

The WHO updates that urologists must be aware of and need to be able to discuss with their team include:
- Updated classification of some of the benign renal neoplasms
- Some renal cancers are now “neoplasms”
- Papillary RCC reclassification
- Molecularly defined cancers
Dr. Shuch states that it is important to understand and recognize rare renal tumors because although most neoplasms are cancers of “standard histology”, (i) 30% of partial nephrectomies have historically been for benign lesions (not just oncocytoma), (ii) ~15-25% of rare kidney tumors are indolent and have limited metastatic potential, (iii) 5-10% of rare kidney cancers are highly aggressive and infiltrative, and (iv) 2-8% of RCC have a strong genetic component, with ~15% of rare tumors being hereditary. For the practicing urologists, the question of importance is whether a tumor should be a radical versus a partial nephrectomy, an enucleation versus a more adequate margin surgical approach should be taken, what genetic testing approach should be used, is there a role for systemic therapy, and should this patient be managed with active surveillance:

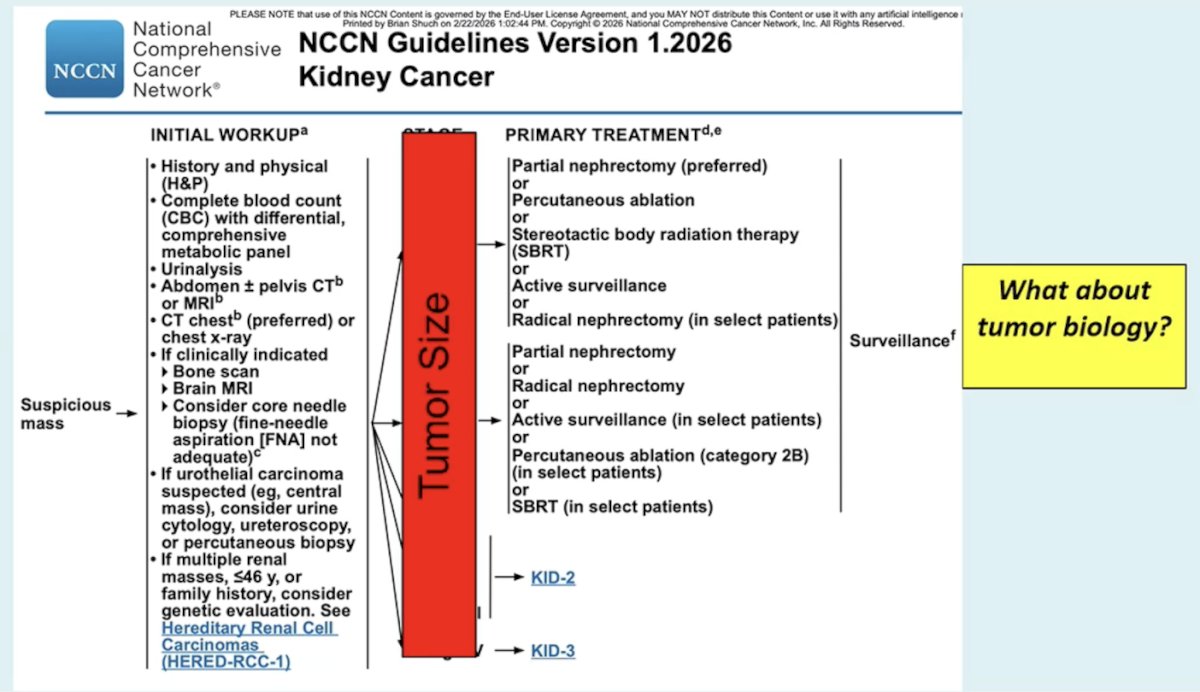
According to Dr. Shuch, the NCCN Guidelines Version 1.2026 for Kidney Cancer come down to tumor size and whether the patient is a surveillance candidate based on tumor biology:
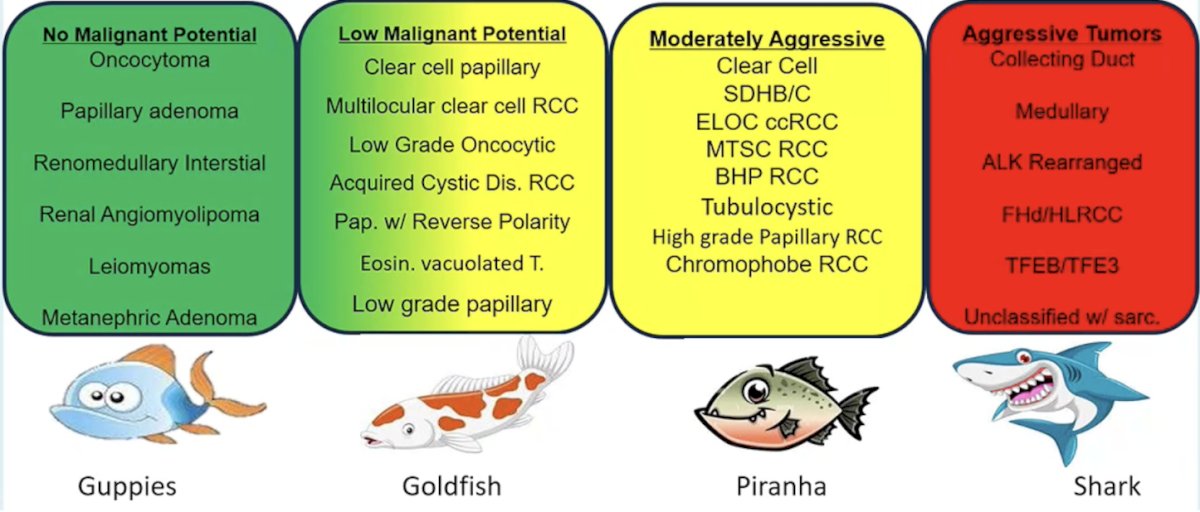
Management should not be driven by appearance, as size does not tell the whole story. RCC subtypes have different biological potential, and size, invasiveness, and metastatic potential varies. Dr. Shuch breaks these categories down into the guppies (no malignant potential), goldfish (low malignant potential), piranhas (moderately aggressive), and sharks (aggressive tumors):
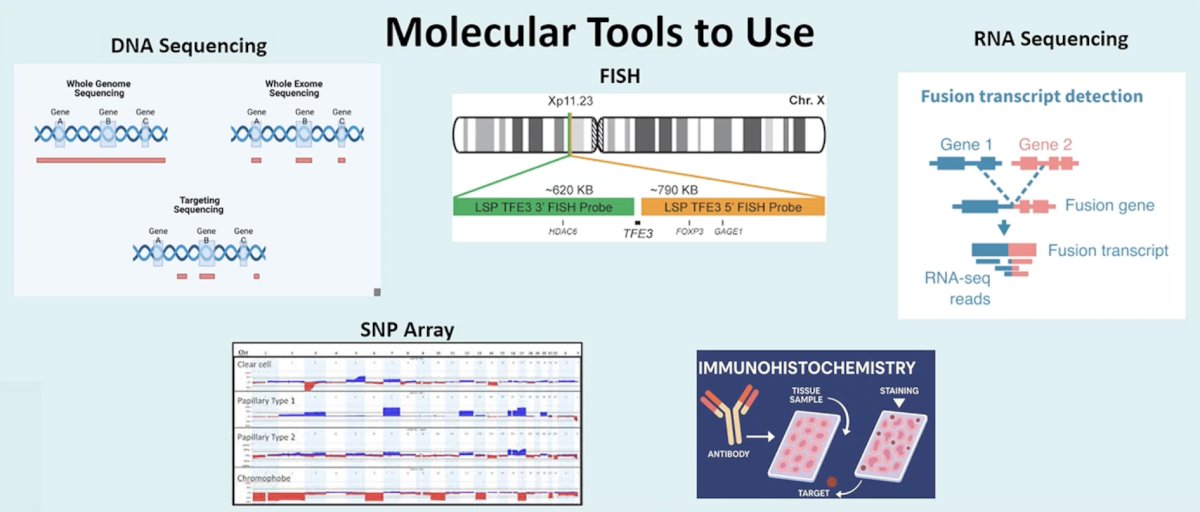
The modern-day urologic oncologist needs to have good tools, but it is also essential that these tools be used in the right way. These molecular tools include (i) DNA sequencing, (ii) SNP array, (iii) FISH, (iv) immunohistochemistry, and (v) RNA sequencing:
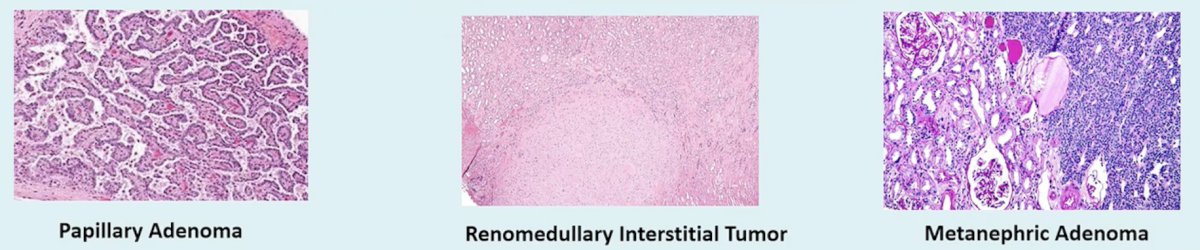
The guppies are the small/benign, and irrelevant lesions:
- Papillary adenoma: found in ~25% of autopsies, <= 15 mm in size, and the question is: is it a precursor to papillary RCC?
- Renomedullary interstitial tumor: formerly “fibroma or hamartoma”, found in 40-50% of autopsies, <= 7 mm, typically a circumscribed medullary nodule
- Metanephric adenoma: residual “nephrogenic rests” resembling Wilms tumor, basophilic/papillary cells, with 95% having a BRAF V600E mutation
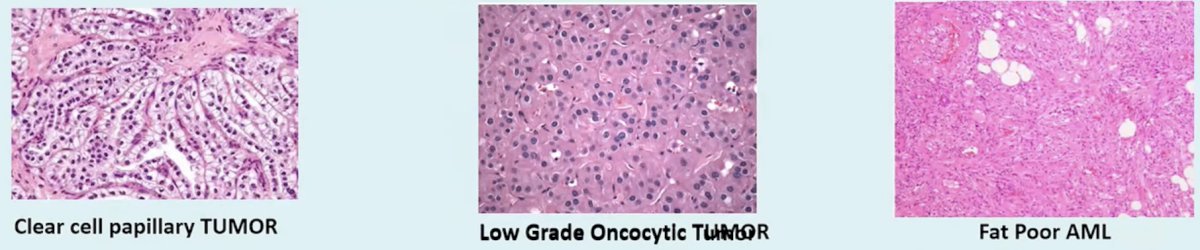
The goldfish are localized and often have incidental lesions:
- Clear cell papillary tumor: low stage/grade and looks “benign-ish”, 50% are solid/50% are cystic, often CK7 and CAIX (cup-like)
- Low-grade oncocytic tumor: benign, mostly < 3 cm, rarely large, often overlaps with renal oncocytoma and chromophobe RCC, CD117 negative/CK7 positivity
- Fat-poor AML: benign, but there is a bleeding risk, do not deform the kidney, and often comes off as a stalk, HMB-45 positive
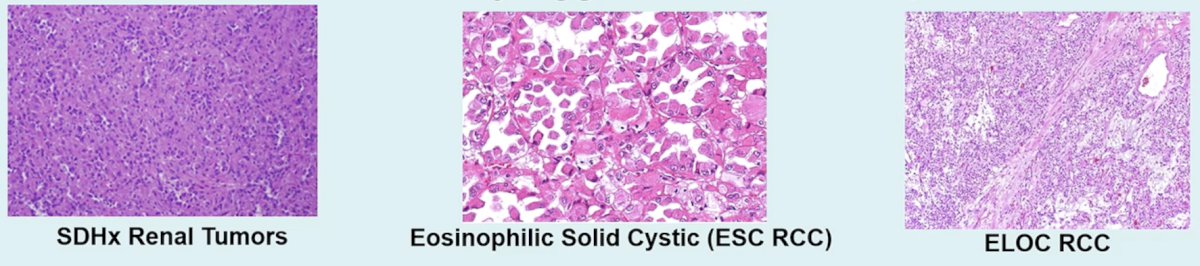
The piranhas are moderately aggressive tumors:
- SDHx renal tumors: early onset, germline mutation in SDHB/C/D, oncoytic but varies by B versus C subtype, and transformed tumors do spread early
- Eosinophilic solid cystic RCC: voluminous eosinophilic cytoplasm, Bosniak 2F/3/4 lesions that are growing, somatic TSC1/2 mutations
- ELOC RCC: clear cells that are separated by thick fibromuscular bands, TCEB1 (Elongin C)/chr8q loss, these may be less aggressive than classic RCC
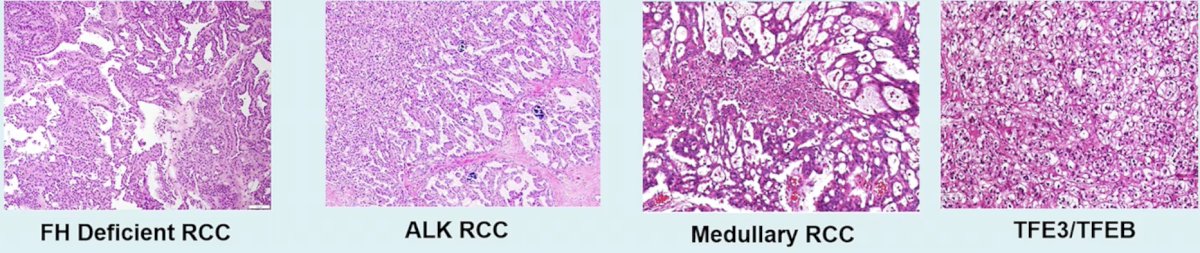
The sharks are aggressive/metastatic cancers:
- FH-deficient RCC: early onset, germline and somatic mutations, solid/cystic lesions, FH loss or 2SC expression
- ALK RCC: diverse patterns, T1/2 with aggressive course, ALK fusions/ALK immunohistochemistry positive, respond to ALK inhibitors
- Medullary RCC: African Americans with Sickle Cell trait, various histologies, loss of INI/SMARCB1 loss, surgery should not be first, as chemotherapy should be initiated as soon as possible
- TFE3/TFEB: clear cell/papillary, nodes are often involved, multiple somatic fusions, and FISH/RNA sequencing is better than immunohistochemistry
Dr. Shuch emphasized that specific histology alone (hybrid oncocytic/FH/SDH loss) should lead to genetic testing, and that age, multifocality, clinical features, and family history may be suggestive of hereditary RCC. The importance of clinical recognition of hereditary RCC to the individual is that it allows screening of other organs (ie. SDH RCC - neck screening), early intervention limits complications (ie. VHL – blindness, deafness), we can apply known management patterns (ie. 3 cm rule, use PET in HLRCC), and it provides choices for systemic therapies (ie. EGFR/VEGF HRLCC). The importance of clinical recognition of hereditary RCC to other family members is that they can be screened, and cascade testing can be initiated.
Dr. Shuch concluded his presentation discussing what the general urologist should know for rare renal tumors with the following take-home points:
- Renal tumor classification is expanding, with >20 WHO-recognized subtypes of tumors
- Rare renal tumors vary widely in their behavior
- Histologic and molecular characterization guide surgical decisions, surveillance strategies, and systemic therapy choices
- Clinical red flags, including unique histology, should prompt evaluation for hereditary RCC, benefiting both patients and at-risk family members
- Advanced imaging and molecular tools are reshaping diagnosis, risk stratification, and personalized care
Presented by: Brian Shuch, MD, Professor of Urology, Director of the Kidney Cancer Program, Alvin & Carrie Meinhardt Endowed Chair in RCC Cancer Research, University of California Los Angeles (UCLA), UCLA Urology, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.