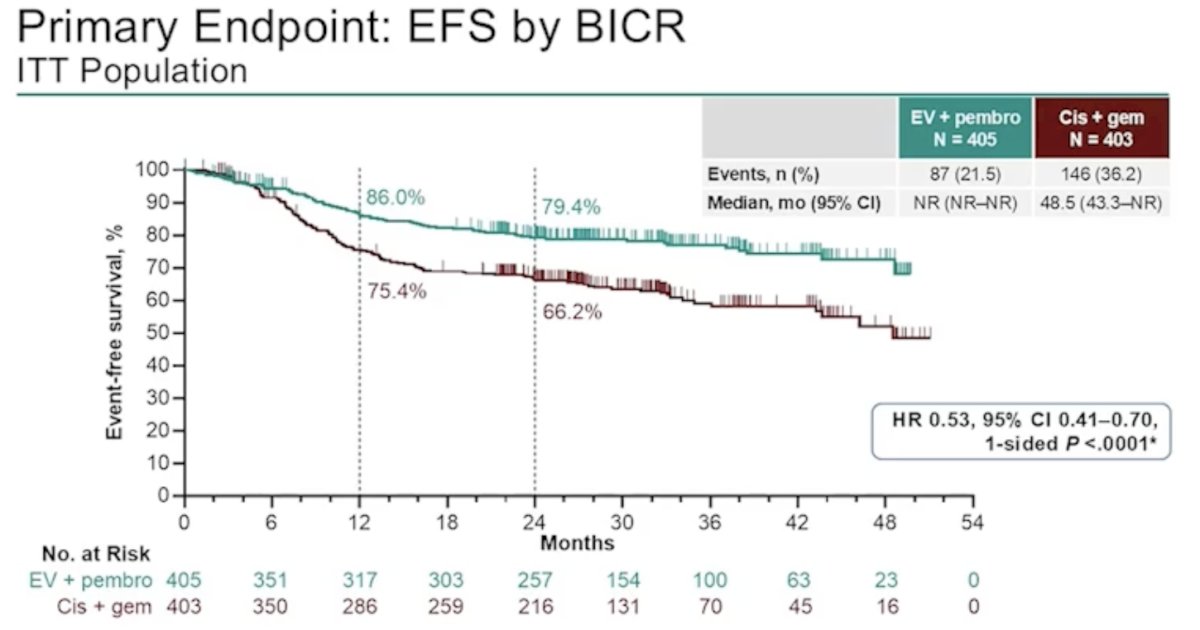
(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a game changer session and a discussant presentation by Dr. Ashish Kamat discussing pathological and surgical outcomes in KEYNOTE-B15/EV-304, assessing neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab for patients with muscle invasive bladder cancer who are eligible for cisplatin. Previously presented at ASCO GU 2026, Dr. Galsky reported that KEYNOTE-B15/EV-304 met its primary endpoint of improving event free survival, with a median not reached (95% CI not reached to not reached) for enfortumab vedotin + pembrolizumab and 48.5 months (95% 43.3 to not reached) for cisplatin + gemcitabine (HR 0.53, 95% CI 0.41-0.70; p < 0.0001). The 12 month event free survival rate for enfortumab vedotin + pembrolizumab was 86.0% versus 75.4% for cisplatin + gemcitabine, and the 24 month rate was 79.4% for enfortumab vedotin + pembrolizumab versus 66.2% for cisplatin + gemcitabine:
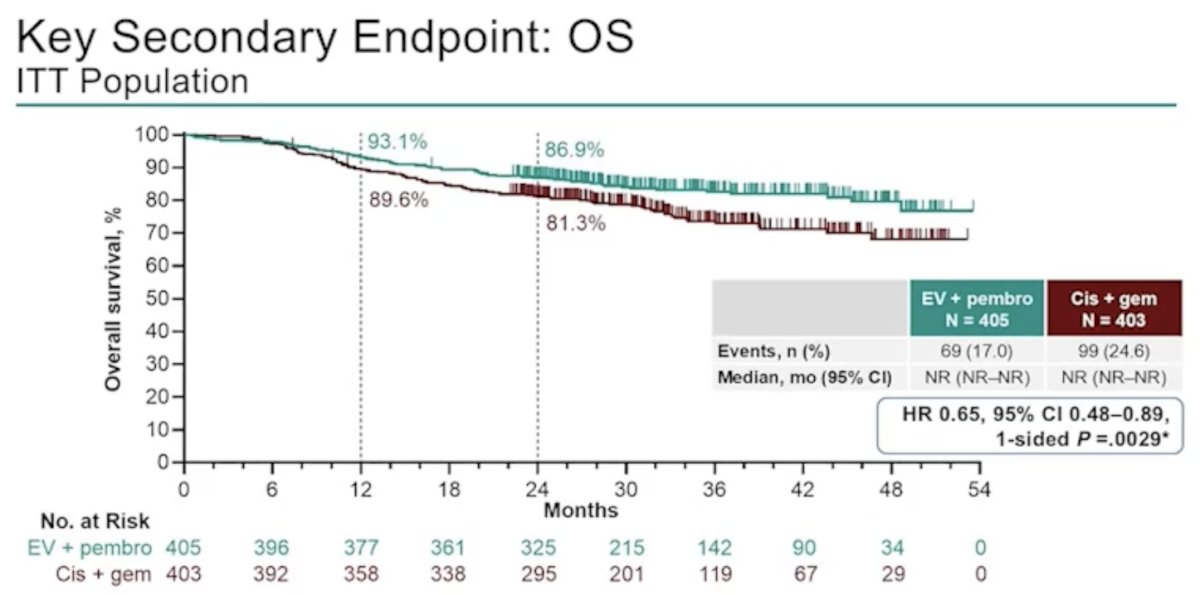
In addition, the key secondary endpoint of median overall survival was not reached in either arm, with the hazard ratio favoring enfortumab vedotin + pembrolizumab: HR 0.65, 95% CI 0.48-0.89; p = 0.0029. The 12 month overall survival rate was 93.1% for enfortumab vedotin + pembrolizumab versus 89.6% for cisplatin + gemcitabine, with a 24 month rate of 86.9% and 81.3%, respectively:
Dr. Kamat notes that there are several practical issues – enfortumab vedotin + pembrolizumab works, but:
- Does it preclude or delay radical cystectomy?
- Does it make the surgical procedures more complicated, hinder recovery, or increase complications?
- Does it change the role or necessity of radical cystectomy?
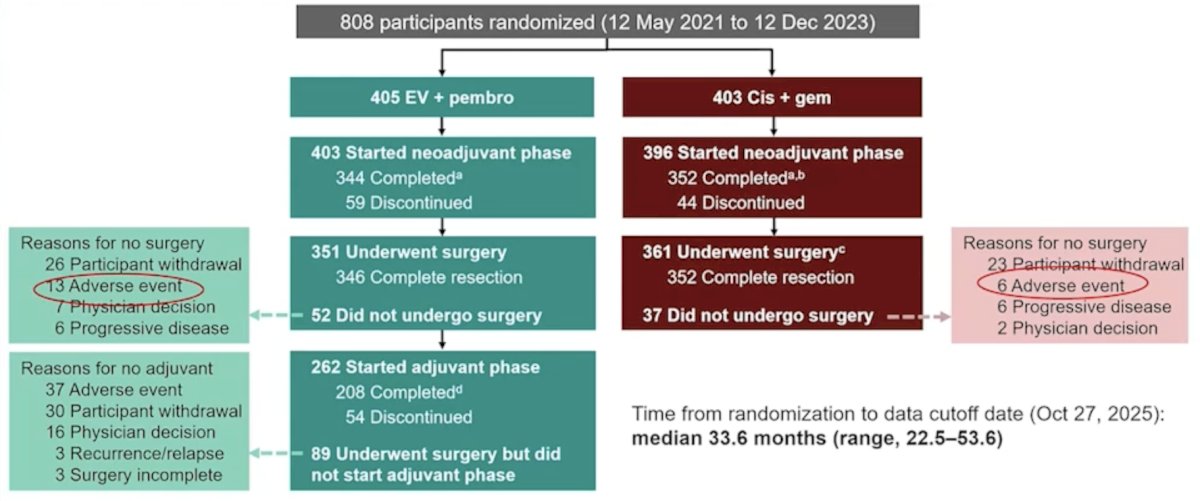
Looking at the patient disposition figure, Dr. Kamat notes that of the patients undergoing surgery in the enfortumab vedotin + pembrolizumab arm, 13 patients did not undergo surgery secondary to an adverse event compared to 6 patients in the cisplatin + gemcitabine arm, so enfortumab vedotin + pembrolizumab does not appear to preclude surgery:
Additionally, enfortumab vedotin + pembrolizumab does not appear to delay surgery, as 26 patients had a delay secondary to an adverse event compared to 16 for patients undergoing cisplatin + gemcitabine:
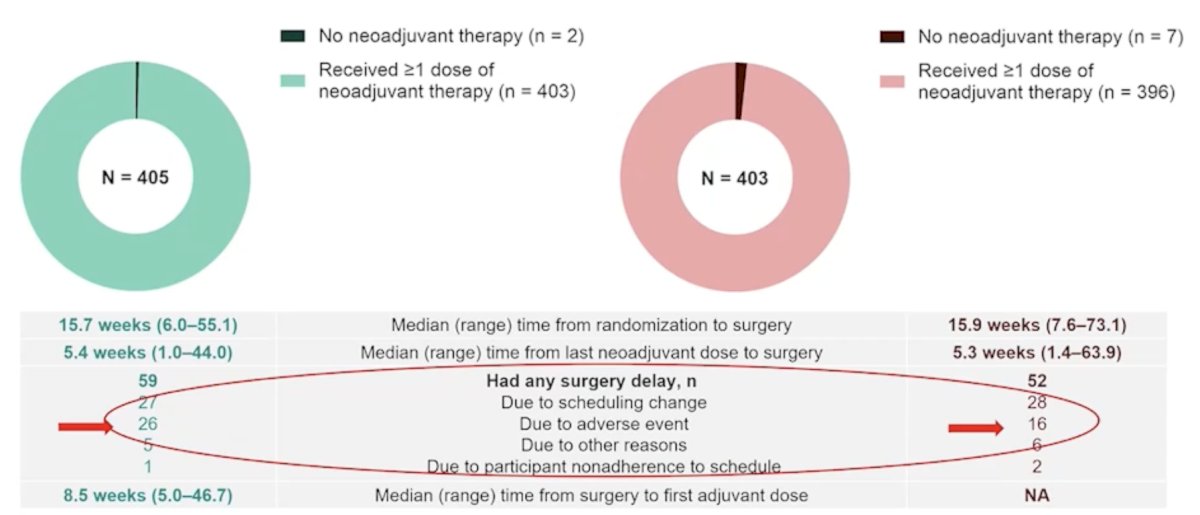
However, when comparing patients who did not undergo surgery secondary to an adverse event with those who had a delay in surgery secondary to an adverse event, there is a statistically significant difference between patients in the enfortumab vedotin + pembrolizumab arm (9.6%) compared to the cisplatin + gemcitabine arm (5.5%; p = 0.028). Dr. Kamat notes this, not because we should not be using enfortumab vedotin + pembrolizumab, but in order to recognize that there is a new toxicity profile that we have to be aware of. As such, a shifting toxicity profile requires proactive management: we are trading systemic chemotherapy side effects for distinct antibody drug conjugate specific and immunotherapy specific issues:
Dr. Kamat notes that these are not just ‘medical’ side effects; they directly impact a patient’s ability to recover from major abdominal surgery, and vigilant management is now a surgical duty.
Does it make the surgical procedures more complicated, hinder recovery, or increase complications?
During the surgical phase only, 36.2% of patients receiving enfortumab vedotin + pembrolizumab had treatment emergent adverse events compared to 35.4% of patients receiving cisplatin + gemcitabine:
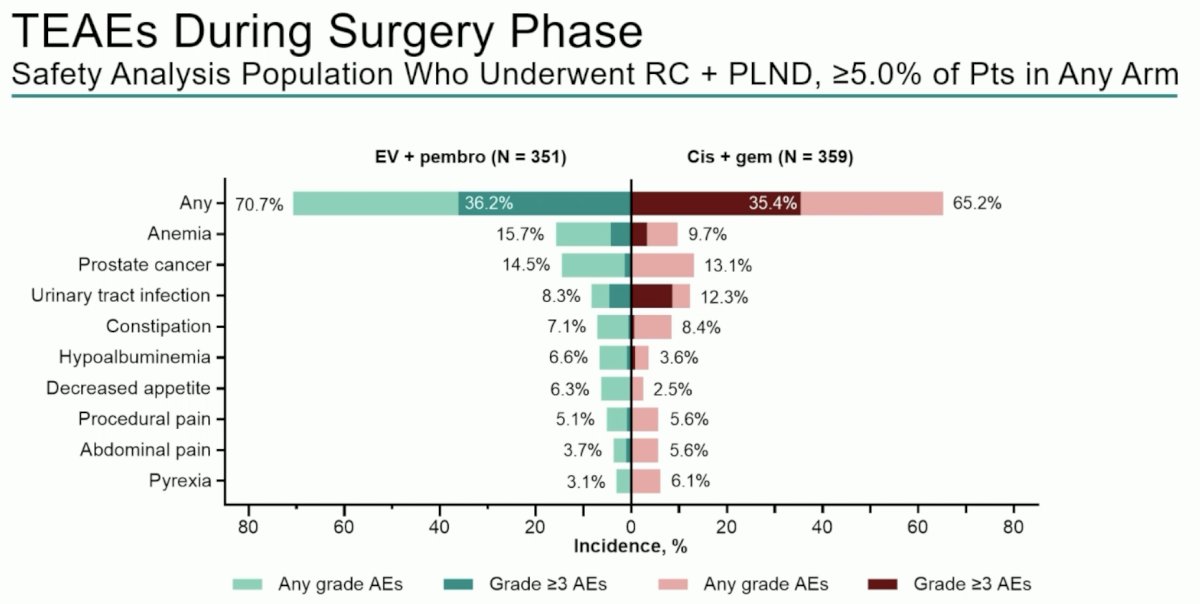
Dr. Kamat cautions that these data do not necessarily answer the question of whether enfortumab vedotin + pembrolizumab increases specific surgical issues such as anastomotic leaks or post-operative bowel issues. As follows is a composite slide of all the data from the KEYNOTE-B15 and KEYNOTE-905 trials created by Dr. Kamat:
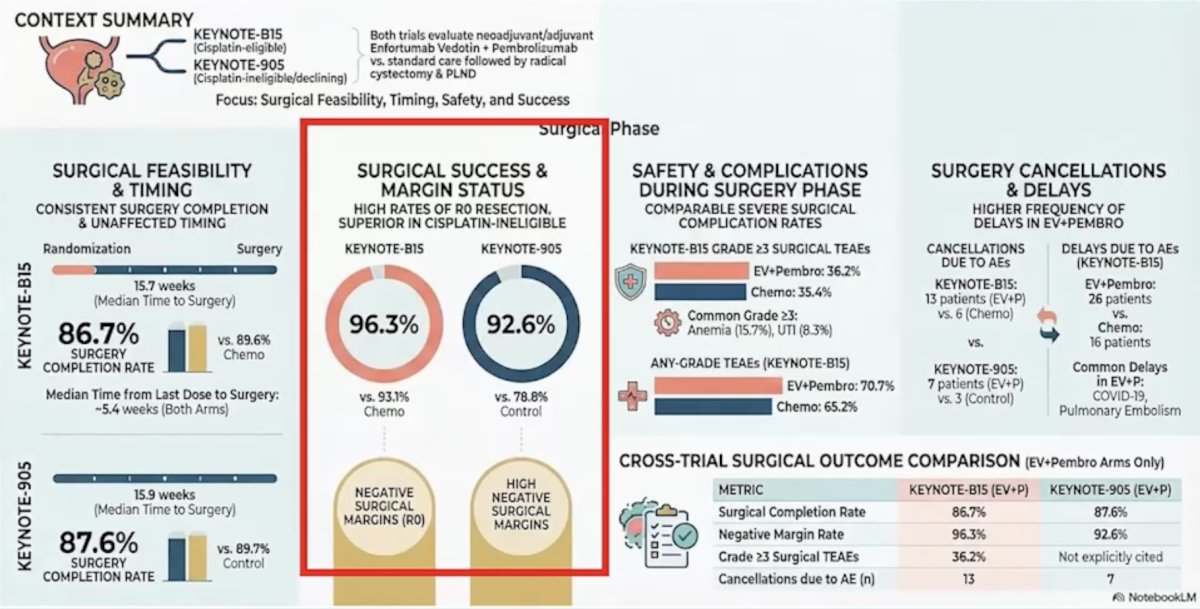
Of note, the surgical success and margin status show that the negative margin rates are higher in the enfortumab vedotin + pembrolizumab arm. Thus, while the surgery may be different compared to after cisplatin + gemcitabine, it does not appear to be more difficult.
Does it change the role or necessity of radical cystectomy?At ASCO GU 2026, the pathological complete response rate for enfortumab vedotin + pembrolizumab was 55.8% versus 32.5% for cisplatin + gemcitabine, with an estimated difference of 23.4% (95% CI 16.7 – 29.8; p < 0.001). Presented at EAU 2026, 258/405 patients (63.7%) in the enfortumab vedotin + pembrolizumab arm and 182/403 (45.2%) in the cisplatin + gemcitabine arm had pathological downstaging (estimated difference, 18.6%, 95% CI 11.8–25.2):
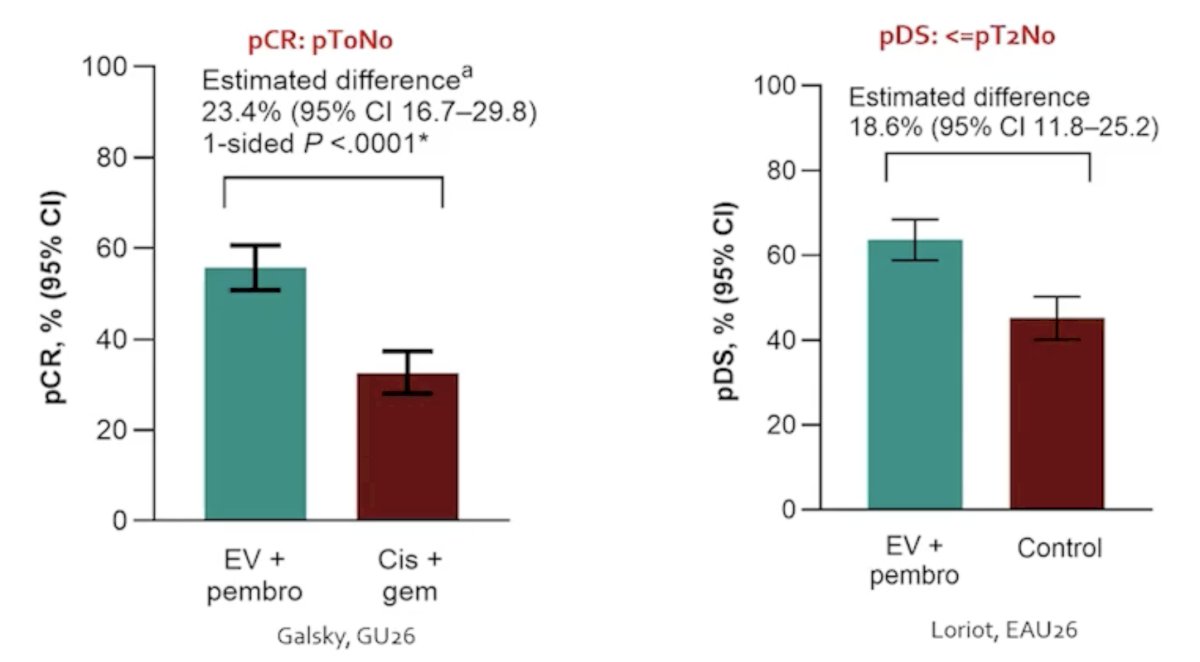
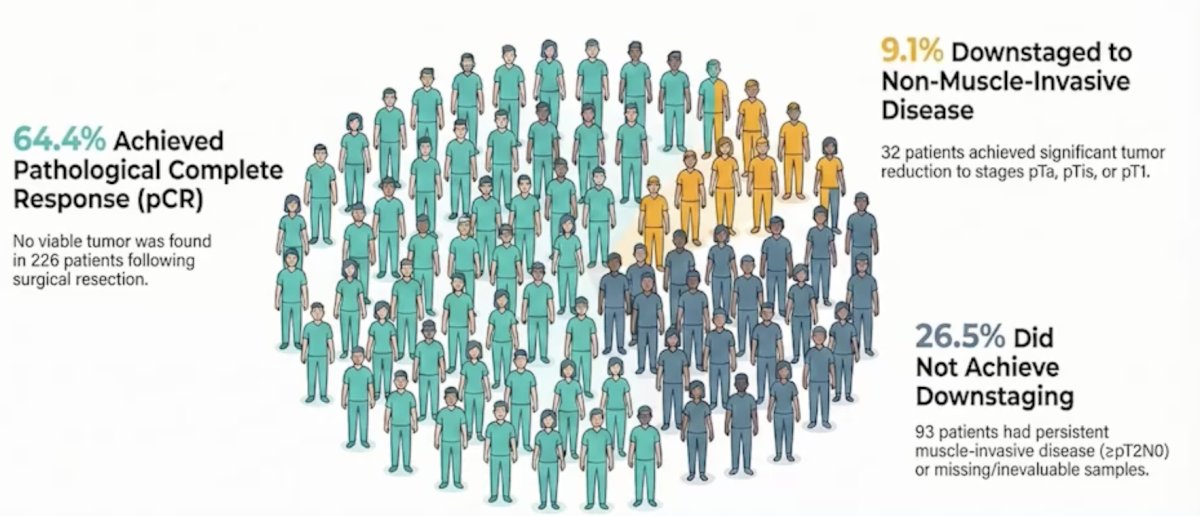
Dr. Kamat states that clearly, we are getting more patients with no disease in the bladder after enfortumab vedotin + pembrolizumab, in addition to downstaging to non muscle invasive disease in the bladder. Thus, among the 351 patients with muscle invasive bladder cancer receiving enfortumab vedotin + pembrolizumab that underwent radical cystectomy, 64.4% of patients achieved a pathological complete response, 9.1% had pathological downstaging, meaning that only 26.5% did not achieve downstaging in the bladder:
Patients are always asking, “Why do I have to have my bladder removed?” In order to address this issue, the International Bladder Cancer Group (IBCG) provided a consensus for end points for next generation bladder sparing perioperative trials for patients with muscle invasive bladder cancer.1 Importantly, in order to answer this question, we need to study it. As follows is an overview from the IBCG of standard of care treatment for surgically fit and systemic treatment eligible patients with muscle invasive bladder cancer and next generation bladder preservation strategies:
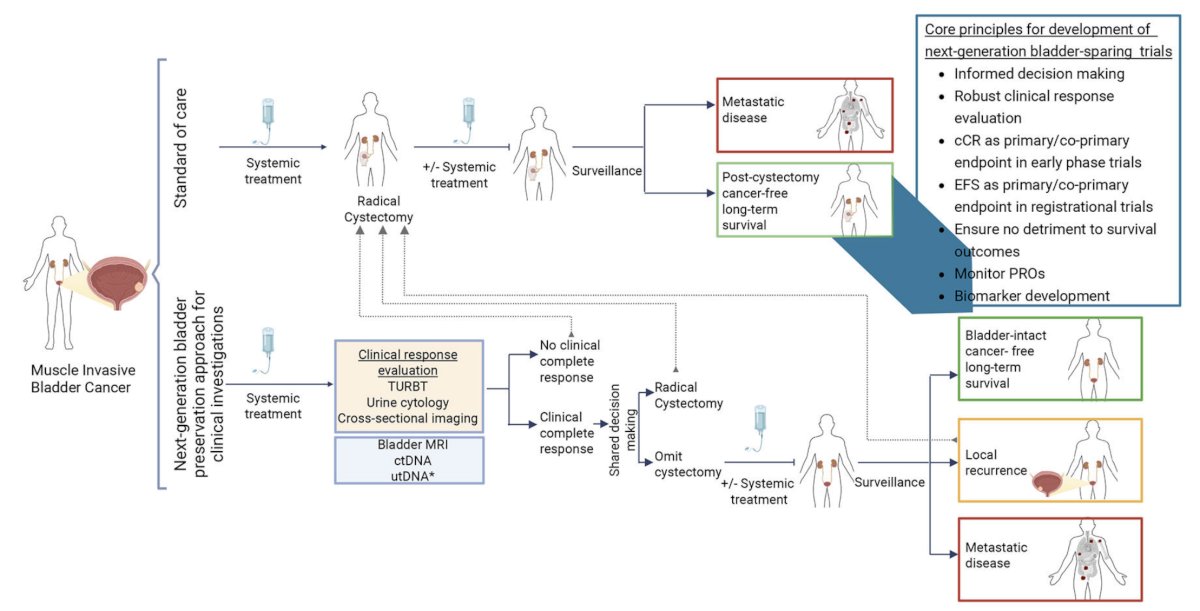
Until we have the answer as to whether we can safely spare the bladder, Dr. Kamat emphasized that we need to stick to the plan: deliver a unified message that enfortumab vedotin + pembrolizumab and radical cystectomy together provide a survival advantage. We cannot unilaterally skip the surgical phase of this paradigm outside of a clinical trial. The survival benefit seen in KEYNOTE-B15/EV-304 and KEYNOTE 905/EV-303 relies on consolidation with radical cystectomy + pelvic lymph node dissection, not observation and not trimodal therapy. Systemic therapy shrinks the tumor and surgical consolidation (radical cystectomy + pelvic lymph node dissection) cures the patient (mandatory).
Presented by: Ashish Kamat, MD, MBBS, Professor of Urology and Wayne B. Duddleston Professor of Cancer Research, University of Texas, MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References: