(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a game changer session and a presentation by Dr. Yohann Loriot discussing pathological and surgical outcomes in KEYNOTE-B15, assessing neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab for patients with muscle invasive bladder cancer who are eligible for cisplatin. The randomized phase 3 KEYNOTE-B15/EV-304 study previously demonstrated that neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab significantly improved event-free survival, pathological complete response rate, and overall survival versus neoadjuvant cisplatin + gemcitabine in patients with muscle invasive bladder cancer eligible for cisplatin-based therapy and radical cystectomy + pelvic lymph node dissection. At EAU 2026, Dr. Loriot and colleagues reported the pathological and surgical outcomes from the study.
Adult patients with muscle invasive bladder cancer (clinical stage T2-T4aN0M0 or T1-T4aN1M0 confirmed centrally) eligible for cisplatin-based therapy and radical cystectomy + pelvic lymph node dissection were randomized 1:1 to 4 cycles neoadjuvant enfortumab vedotin + pembrolizumab, surgery, and 5 cycles of adjuvant enfortumab vedotin + 13 cycles of adjuvant pembrolizumab versus 4 cycles neoadjuvant cisplatin + gemcitabine and surgery:

Secondary endpoints included pathological downstaging (<pT2N0 by central pathological review) rate, disease free survival (time from post-surgery scan to local/distant recurrence by blinded independent central review and/or biopsy or death in patients who were disease-free after surgery), and safety. The median study follow-up was 33.6 months (range, 22.5–53.6) as of the data cutoff date (October 27, 2025).
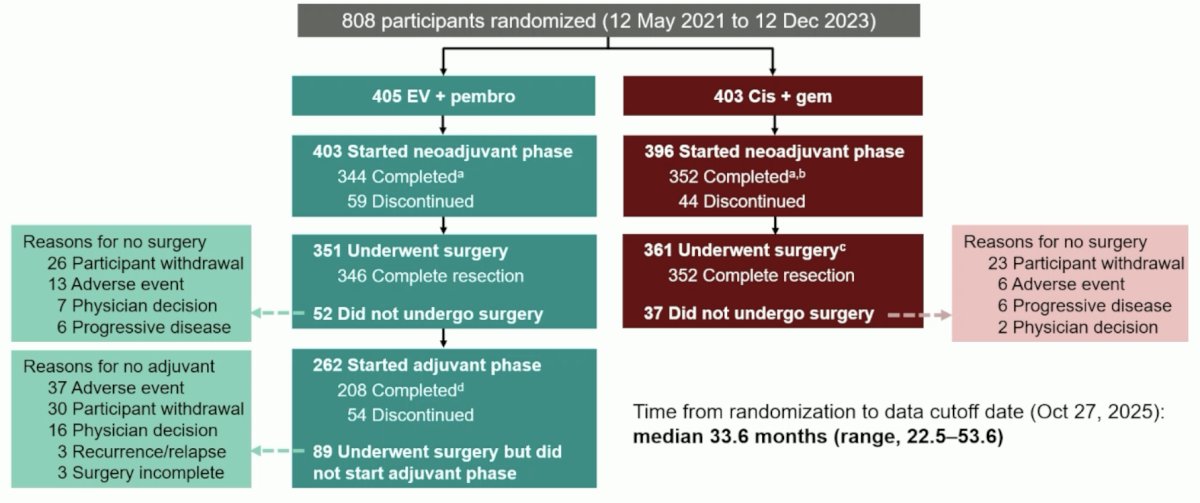
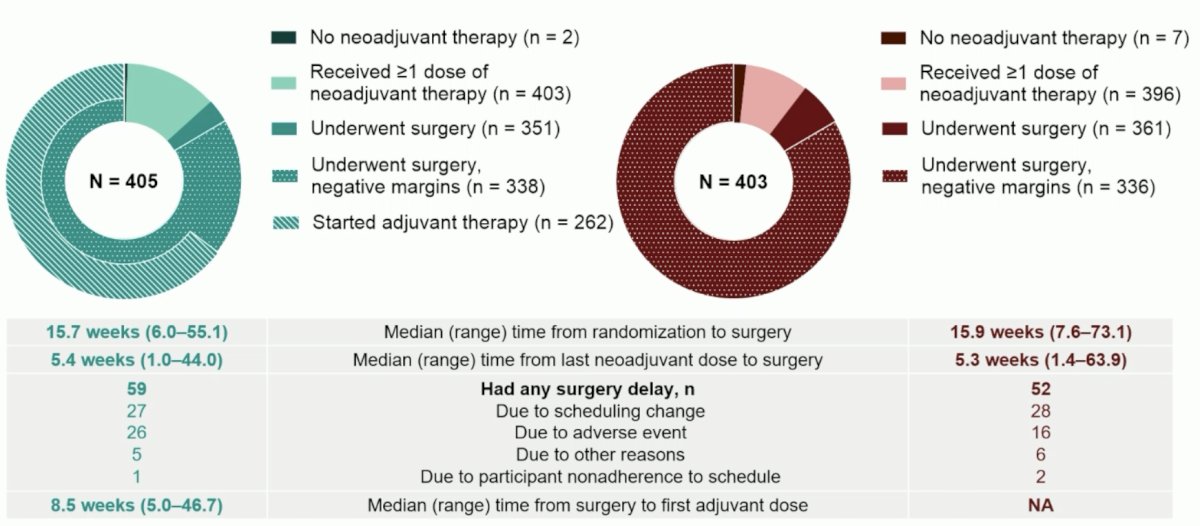
Overall, there were 808 patients randomized (405 to enfortumab vedotin + pembrolizumab versus 403 to cisplatin + gemcitabine). Among 351 and 361 patients who underwent surgery in the enfortumab vedotin + pembrolizumab and cisplatin + gemcitabine arms, 59 (16.8%) and 52 (14.4%) had surgery delay, most commonly due to scheduling change (n = 27 and 28):
There were 338 (96.3%) and 336 patients (93.1%), respectively, who had negative surgical margins after radical cystectomy + pelvic lymph node dissection. The median time from randomization or last neoadjuvant drug dose to surgery was 15.7 weeks (range: 6.0–55.1) and 5.4 weeks (range: 1.0–44.0) in the enfortumab vedotin + pembrolizumab arm, and 15.9 weeks (range: 7.6–73.1) and 5.3 weeks (range: 1.4–63.9) in the cisplatin + gemcitabine arm:
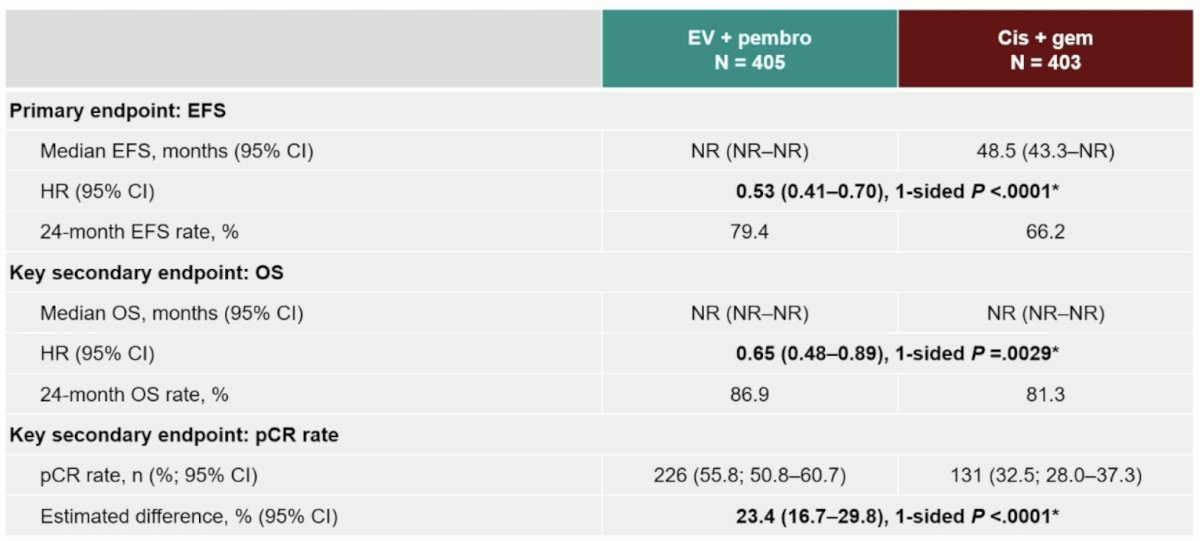
Presented previously at ASCO GU 2026, Dr. Loriot highlighted the primary endpoint results of event free survival, and key secondary endpoints of overall survival and pathological complete response:
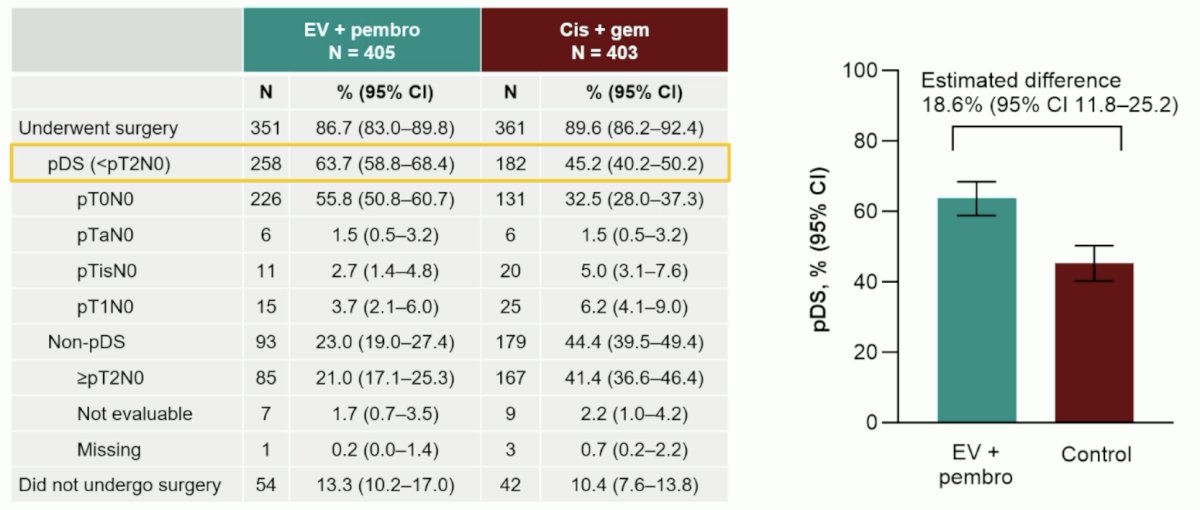
A total of 258/405 patients (63.7%) in the enfortumab vedotin + pembrolizumab arm and 182/403 (45.2%) in the cisplatin + gemcitabine arm had pathological downstaging (estimated difference, 18.6%, 95% CI 11.8–25.2):
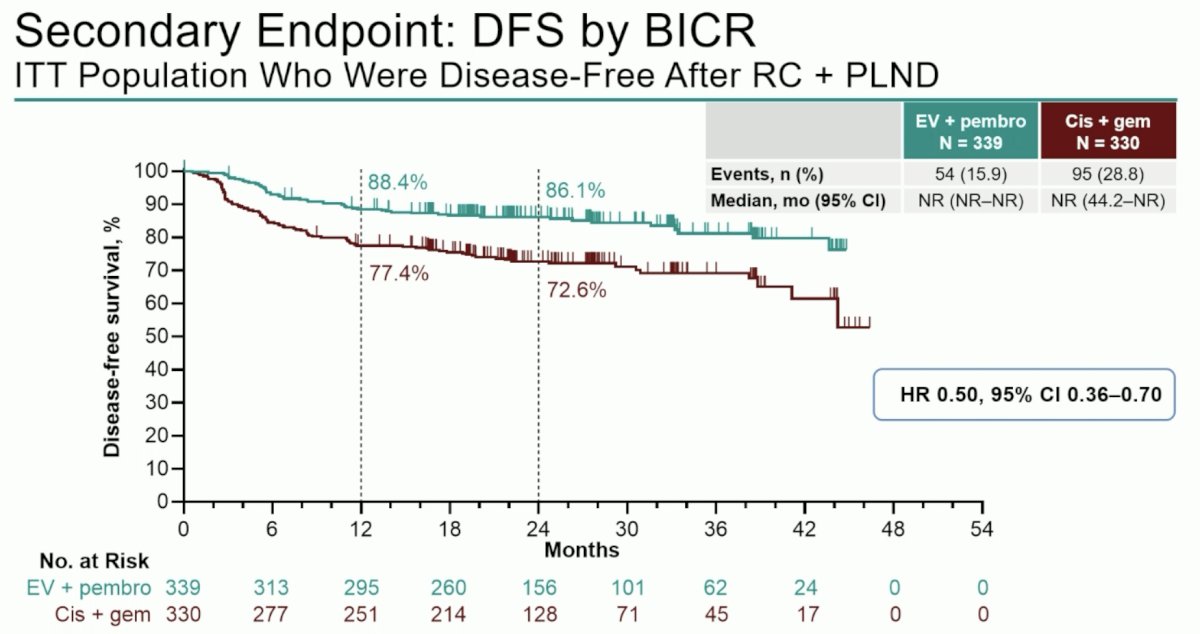
A total of 339 and 330 patients, respectively, were disease free at initial post-surgery scan, and the median disease free survival was not reached in either arm (24-month estimated disease free survival rate 86.1% versus 72.6%; HR 0.50, 95% CI 0.36–0.70):
The median total duration of therapy was 10.2 months (range: 0.03-25.5) in the enfortumab vedotin + pembrolizumab arm compared to 3.5 months (range: 0.03-16.8) in the cisplatin + gemcitabine arm:
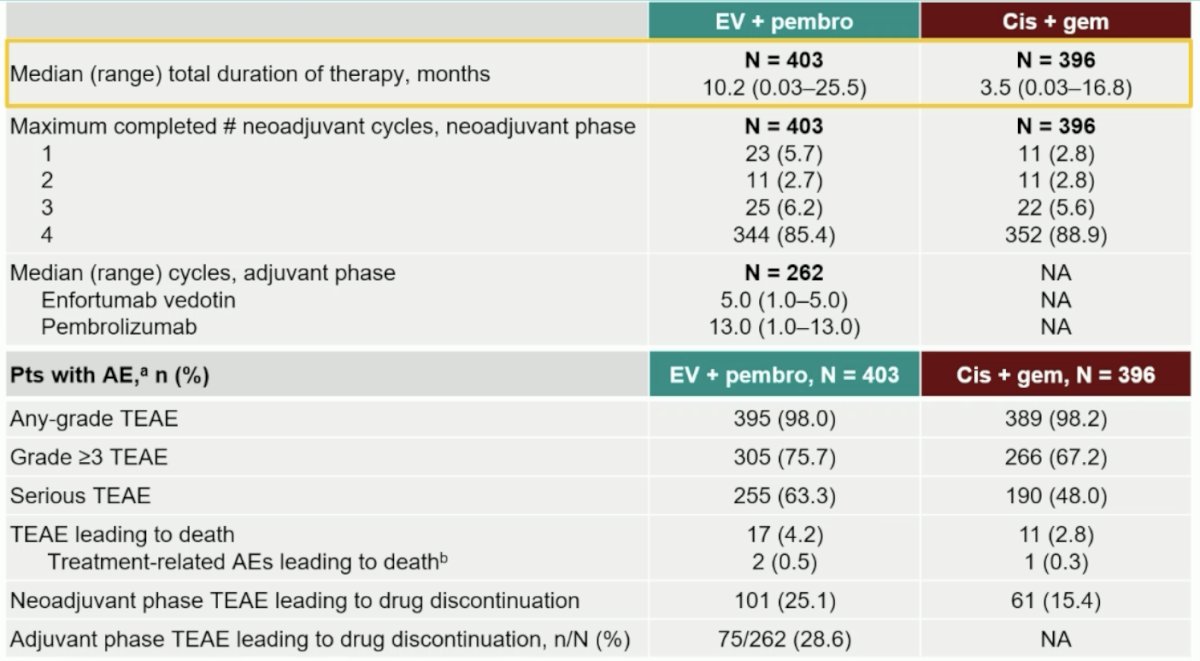
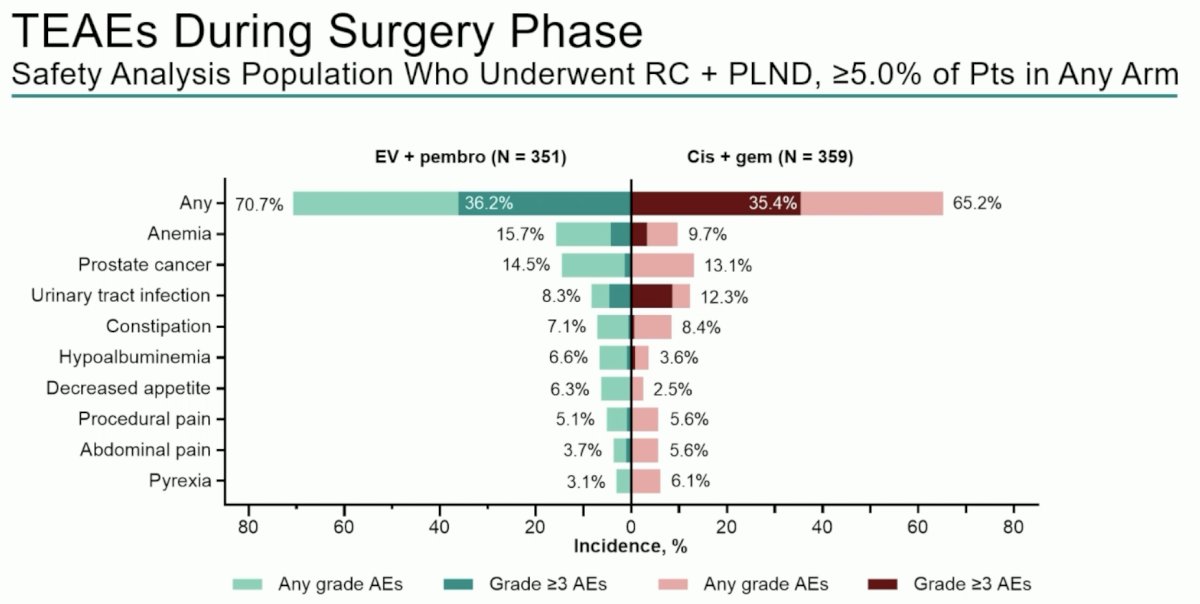
Among randomized patients with ≥1 dose study drug, grade ≥3 treatment-emergent adverse events occurred in 75.7% of 403 patients in the enfortumab vedotin + pembrolizumab arm and 67.2% of 396 patients in the cisplatin + gemcitabine arm over the totality of treatment, and in 36.2% and 35.4% of patients during the surgical phase only:
Dr. Loriot concluded his presentation discussing pathological and surgical outcomes in the KEYNOTE-B15 trial with the following take-home points:
- Enfortumab vedotin + pembrolizumab represents the first ADC + immune checkpoint inhibitor combination to show event free survival, overall survival, and pathological complete response rate benefit versus neoadjuvant cisplatin-based chemotherapy for patients with muscle invasive bladder cancer eligible for curative intent surgery and cisplatin-containing therapy
- Secondary outcomes such as pathological downstaging and disease free survival also favored the neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab arm, consistent with the primary outcomes
- Surgical outcomes and adverse events during the surgical phase were similar between arms:
– A similar proportion of participants underwent cystectomy and had negative margins after cystectomy
– There were no meaningful differences in time to surgery between arms - The safety profile of neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab was consistent with prior experience with this combination regimen (in patients with advanced urothelial carcinoma or patients with muscle invasive bladder cancer who are ineligible for cisplatin-containing therapy)
- Results of the KEYNOTE-B15 study, coupled with prior results from the KEYNOTE-905/EV-303 study, support neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab as a novel treatment option in muscle invasive bladder cancer irrespective of cisplatin eligibility
Presented by: Yohann Loriot, MD, PhD, Gustave Roussy, Cibles en Oncologie, Villejuif, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.