(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a surgical and non-surgical treatment of non-muscle invasive bladder cancer session and a presentation by Dr. Alexandre Zlotta discussing a matched analysis assessing reduced versus full dose BCG maintenance in non-muscle invasive bladder cancer patients treated with full dose induction.
Previous trials have concluded that maintenance BCG decreases the risk of recurrence and progression compared to induction therapy alone. However, there is no consensus on the optimal regimen and dosing. Due to the ongoing BCG shortage, and based on its immunological mode of action, a reduced BCG dose during maintenance—while administering full BCG at induction—has been proposed in non-muscle invasive bladder cancer management. However, data comparing a full BCG dose for induction followed by either a reduced or full dose for maintenance are lacking.
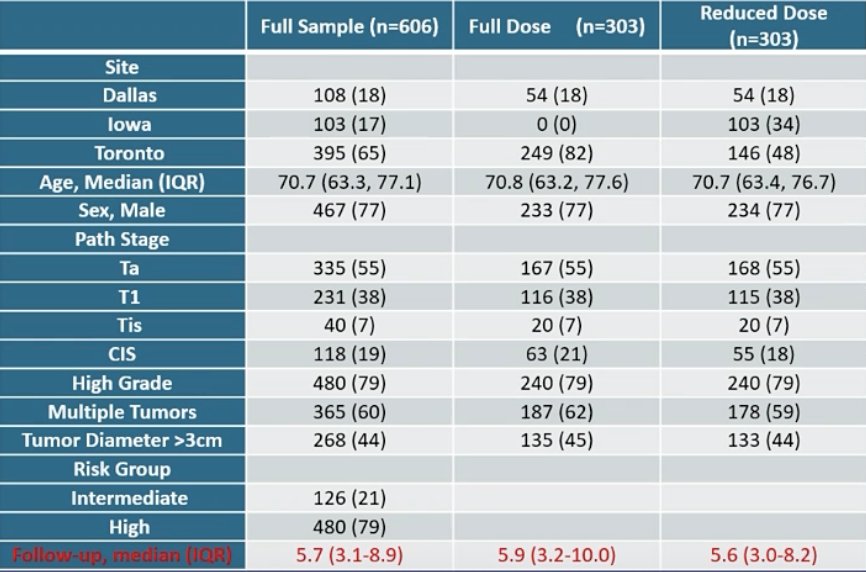
This multicenter retrospective cohort study included 989 patients from four academic institutions (University Health Network, Mount Sinai Hospital, Toronto; University of Iowa; and UT Southwestern, Dallas) from 2004 to 2023. Of these, 625 patients received full-dose BCG for both induction and maintenance, while 364 received full-dose induction followed by a reduced dose for maintenance (1/3 or less). The median follow-up duration was 5.9 (IQR 3.2-10.0) years for patients who received full BCG doses at induction and maintenance, and 5.6 (IQR 3.0-8.2) years for those with reduced maintenance doses. The primary outcome was time to progression (muscle-invasive, nodal, or metastatic disease). Secondary endpoints included overall survival, cancer-specific survival, and recurrence-free survival. Survival probabilities were estimated using the Kaplan-Meier method. Differences in survival outcomes based on treatment were analyzed using propensity scores incorporated into propensity score matching using logistic regression and 1:1 matching with replacement. Cox regression models were used to evaluate covariate associations with outcomes.
After matching, 606 intermediate and high-risk non-muscle invasive bladder cancer patients were included (303 in the full-dose and 303 in the reduced-dose maintenance). The median age was 70.7 (IQR 63.3-77.1) years, 77% were male, 38% had T1HG non-muscle invasive bladder cancer, and 79% had high-grade disease. Baseline clinicopathological characteristics prior to treatment were similar between groups:
The estimated five-year cumulative incidence of tumor progression was 14% (95% CI 10%-19%) for the full-dose BCG maintenance group versus 10% (95% CI 7%-14%) for the reduced dose group (p = 0.144). Multivariable Cox regression analyses, accounting for age, sex, treatment year, and presence of CIS, showed no significant difference in the primary outcome between the full and reduced BCG maintenance doses (HR 0.69; 95% CI, 0.44-1.11; p = 0.13). No significant differences were observed in cancer-specific survival and overall survival; recurrence-free survival was improved with the reduced maintenance dose (HR 0.53, 95% CI 0.43-0.67; p < 0.001):

Dr. Zlotta concluded his presentation discussing a matched analysis assessing reduced versus full dose BCG maintenance in non-muscle invasive bladder cancer patients treated with full dose induction with the following take-home points:
- This retrospective matched-cohort study found no difference in progression, cancer-specific survival, or overall survival between reduced and full BCG doses for maintenance in non-muscle invasive bladder cancer patients who completed full BCG induction
- These results support the need for a randomized clinical trial comparing full versus reduced maintenance BCG in patients after full BCG induction, especially given the shortage of BCG
Presented by: Alexandre R. Zlotta, MD, PhD, FRCSC, Director, Uro-Oncology, Division of Surgical Oncology, Princess Margaret Cancer Centre, University Health Network, Mount Sinai Hospital; Professor and Howard Sokolowski Chair in Uro-Oncological Research, Department of Surgery (Urology), University of Toronto
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.