(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a surgical and non-surgical treatment of non-muscle invasive bladder cancer session and a presentation by Dr. Pietro Scilipoti discussing a multicenter European study assessing the impact of BCG failure pattern on oncologic outcomes of intravesical gemcitabine and docetaxel in high-risk non-muscle invasive bladder cancer. Intravesical gemcitabine + docetaxel has emerged as a bladder-sparing option for patients with high-risk non-muscle invasive bladder cancer after BCG failure. Whether different BCG failure types affect gemcitabine + docetaxel outcomes remains unclear.
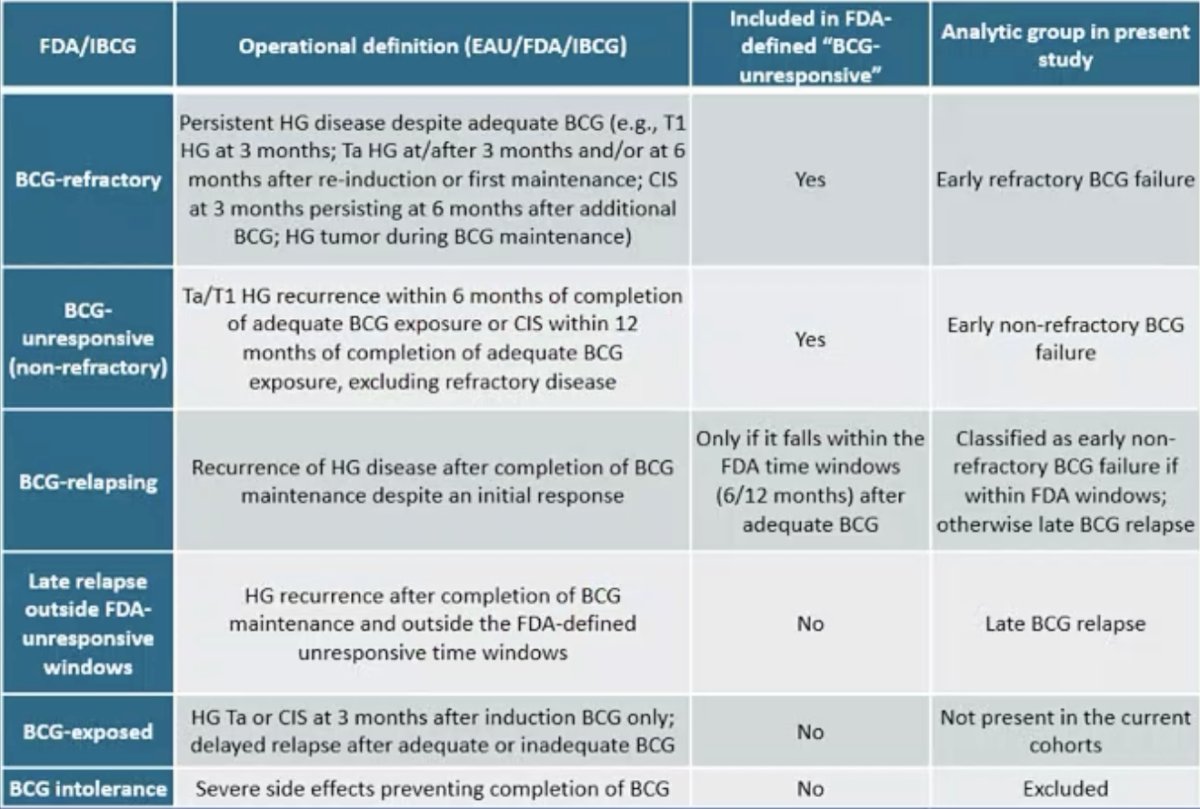
Dr. Scilipoti and colleagues retrospectively analyzed 186 patients with high-risk non-muscle invasive bladder cancer treated with gemcitabine + docetaxel after prior BCG across 14 European centers (2021–2025). Eligible patients completed ≥5 induction instillations and had at least one follow-up cystoscopy, while BCG-intolerant cases were excluded. BCG failure was classified per FDA/IBCG definitions as unresponsive, refractory, or relapsing:
Outcomes included recurrence-free survival, high-grade recurrence-free survival, progression-free survival, and radical cystectomy-free survival. Cumulative incidence functions estimated event risks, and multivariable Cox models, adjusted for histology, multifocality, and tumor size, evaluated associations between BCG failure type and outcomes.
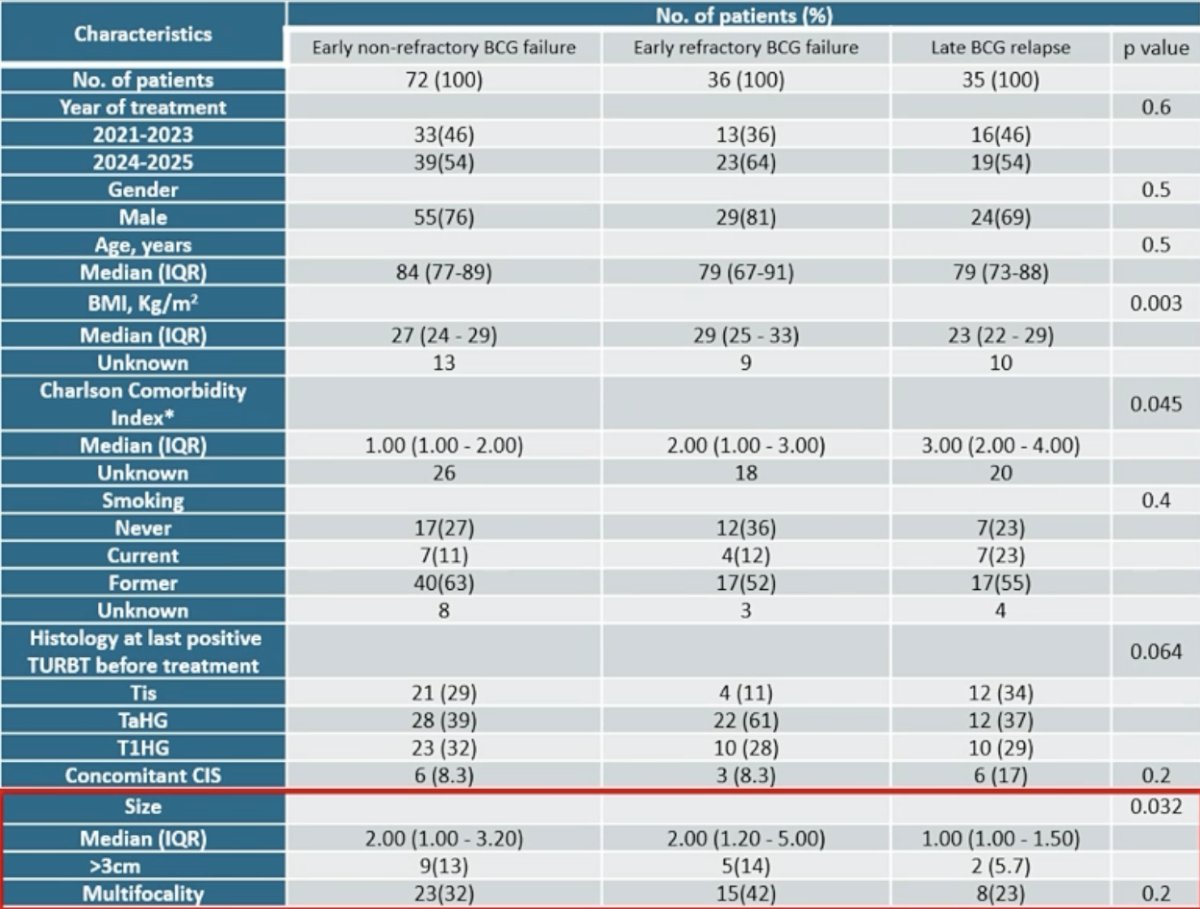
Among 143 eligible patients, 72 were BCG-unresponsive, 36 were BCG-refractory, and 35 were BCG-relapsing. The median age was 82 years (IQR 74–89), and relapsing patients had lower comorbidity and smaller tumors than refractory cases:
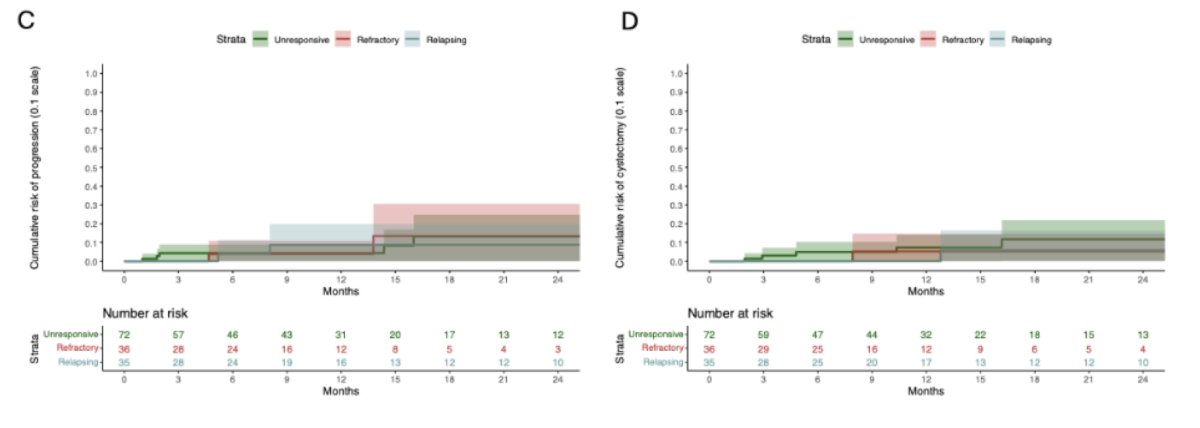
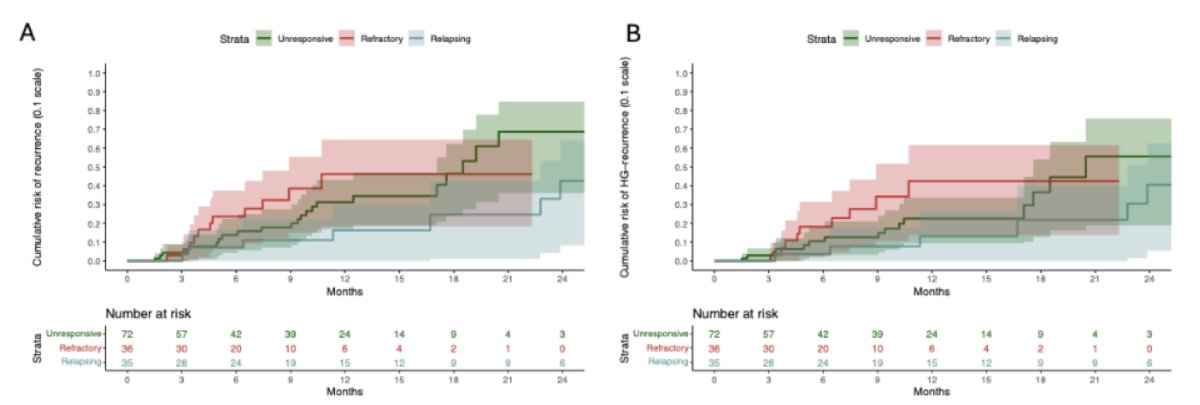
At 12 months, the cumulative recurrence risk was 28% for BCG-unresponsive, 34% for BCG-refractory, and 18% for BCG-relapsing disease. High grade-recurrence risks were 25%, 31%, and 15%, respectively (all p < 0.05), and progression risk and cystectomy rates remained <10% across groups:
On multivariable analysis, BCG-relapsing disease was associated with lower recurrence risk versus BCG-unresponsive disease (HR 0.40, 95% CI 0.16–0.97; p = 0.042), but not with high-grade recurrence (HR 0.48, 95% CI 0.18–1.27; p = 0.14):
Dr. Scilipoti concluded his presentation discussing a multicenter European study assessing the impact of BCG failure pattern on oncologic outcomes of intravesical gemcitabine and docetaxel in high-risk non-muscle invasive bladder cancer with the following take-home points:
- Gemcitabine + docetaxel is effective and well-tolerated across BCG failure types
- BCG-relapsing patients experienced more favorable outcomes, whereas BCG-refractory disease showed a higher recurrence risk
- These findings support gemcitabine + docetaxel as a viable bladder-sparing option but highlight the need for careful selection and counseling, particularly in BCG-refractory cases
Presented by: Pietro Scilipoti, MD, Urologist, IRCCS Ospedale San Raffaele, Vita-Salute San Raffaele University, Milan, Italy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.