(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., between March 13th and 16th 2026, was host to the BCG meets immunotherapy in high-risk NMIBC: Key lessons for urologists from POTOMAC, ALBAN, and CREST Thematic Session. Dr. Morgan Rouprêt presented highlights of the ALBAN trial - Atezolizumab + BCG (a negative trial).
Dr. Rouprêt began by highlighting that among the three trials discussed, ALBAN was the only negative study. However, he emphasized that there are still important lessons to be learned from it. The ALBAN trial was an academically driven study conducted through the APHP network, involving close collaboration between medical oncologists and urologists. It was designed as a phase III, randomized international trial, enrolling patients across multiple centers in France, as well as sites in Spain and Belgium
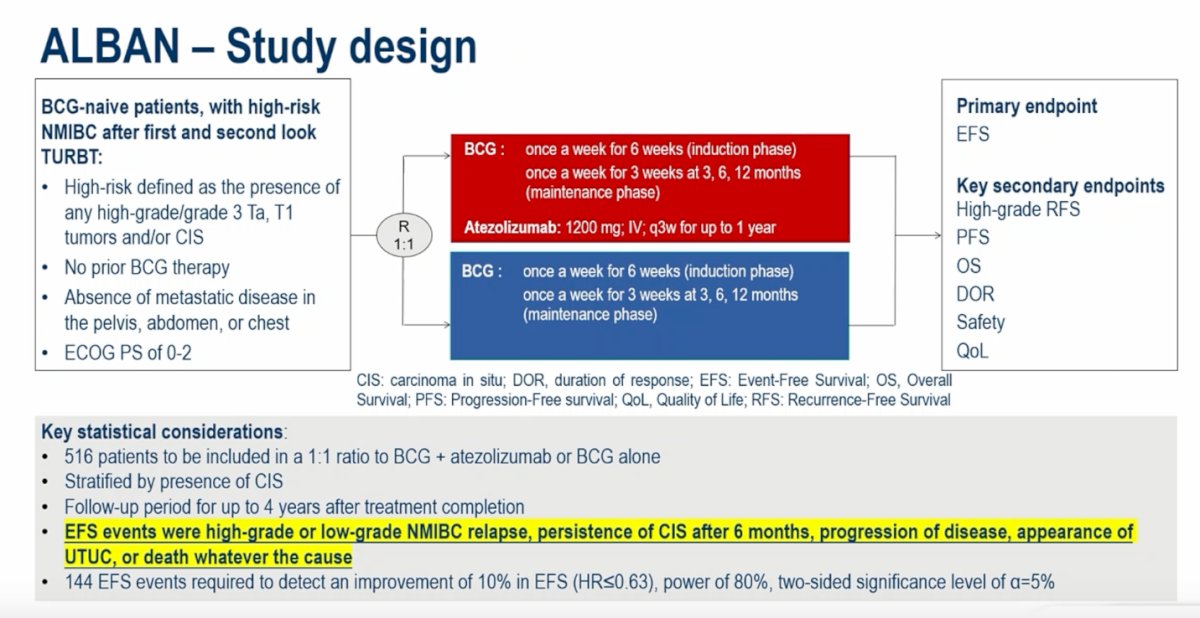
He then described the study design of the ALBAN trial, which was intentionally conceived as a pragmatic study. At the time the trial was designed, Europe was facing a significant BCG shortage. The investigators recognized the importance of maintenance BCG but were uncertain whether long maintenance schedules would be feasible given supply limitations, and therefore intentionally incorporated a shorter maintenance approach.
From a statistical standpoint, the trial planned to enroll 516 patients randomized in a 1:1 ratio to receive BCG plus atezolizumab or BCG alone, with stratification according to the presence of CIS. Patients were followed for up to four years after treatment completion. Event-free survival was the primary endpoint, with events defined broadly and including high-grade or low-grade NMIBC recurrence, persistence of CIS at six months, disease progression, development of upper tract urothelial carcinoma, or death from any cause. A total of 144 EFS events were required to detect an absolute improvement of 10% in EFS (HR ≤0.63), providing 80% power with a two-sided alpha level of 5%.
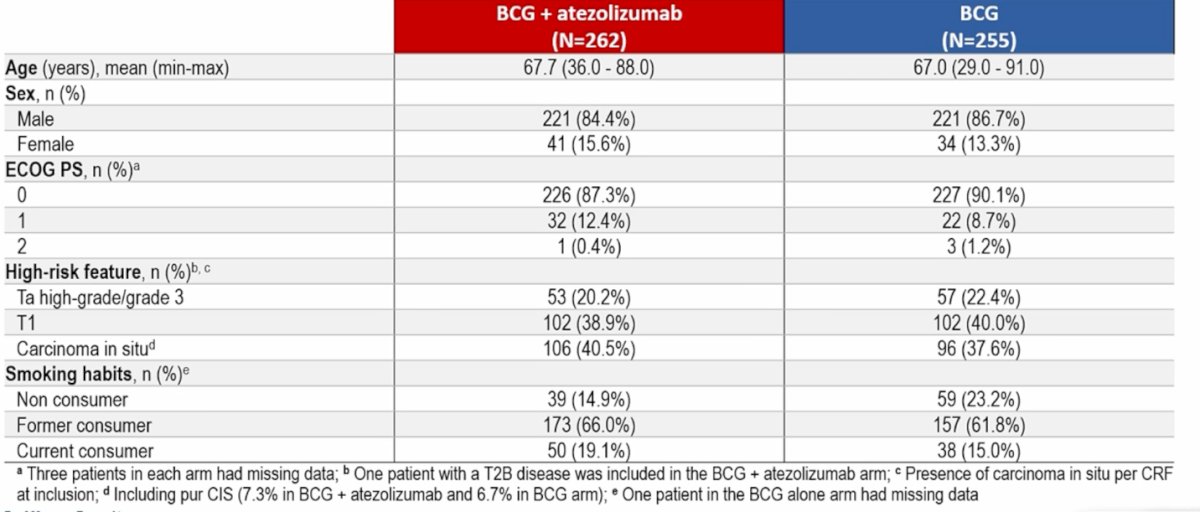
A total of 517 patients were randomized to receive either BCG plus atezolizumab (n=262) or BCG alone (n=255) across centers in France, Belgium, and Spain. Baseline demographic and disease characteristics were generally well balanced between the two treatment arms. The median age was approximately 67 years, and most patients had an ECOG performance status of 0. In terms of disease characteristics, high-risk NMIBC features were well represented, including T1 disease and carcinoma in situ. Notably, approximately 40% of patients in the BCG plus atezolizumab arm had CIS at baseline, reflecting a population with a substantial proportion of high-risk disease.
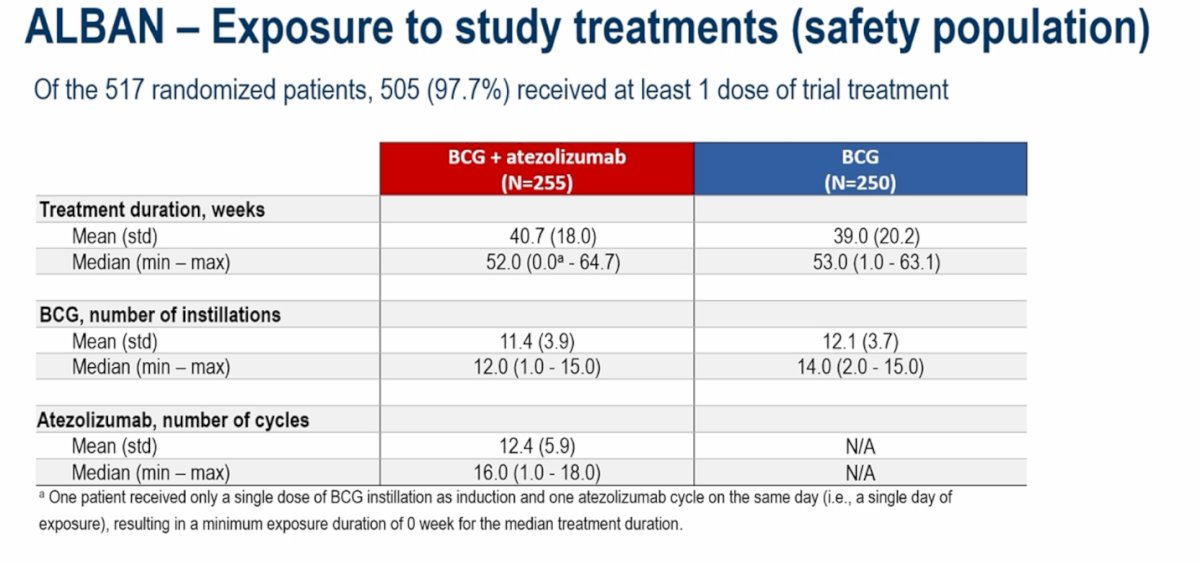
Dr. Rouprêt emphasized the concept of BCG exposure, noting that this is a term familiar to experts in the field and important when interpreting the ALBAN results. In this trial, BCG exposure was lower than in the other contemporary studies, with a median of 12 instillations in the BCG + atezolizumab arm and 14 in the BCG-alone arm. He pointed out that BCG exposure in ALBAN was therefore shorter than in POTOMAC and CREST, an important difference when comparing outcomes across trials.
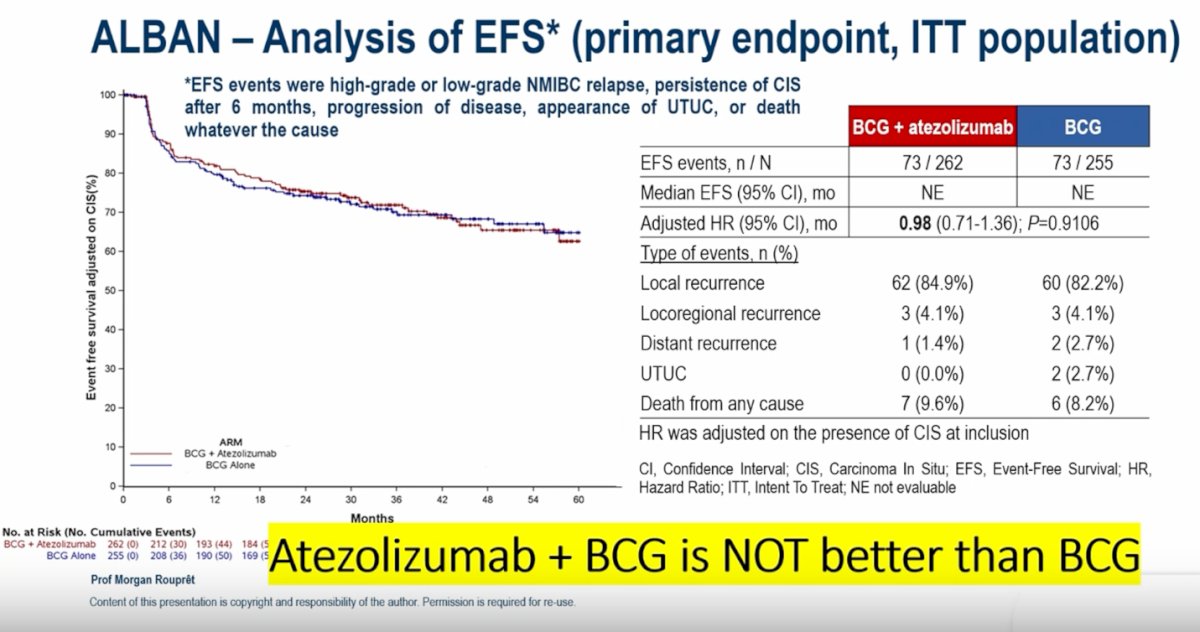
The ALBAN trial was negative for its primary endpoint. Event-free survival was similar between the two treatment arms, with 73 events observed in both groups. The addition of atezolizumab to BCG did not improve outcomes compared with BCG alone (HR 0.98, 95% CI 0.71–1.36; p=0.91), indicating no benefit from the combination in this setting.
Although the ALBAN trial was negative overall, Dr. Rouprêt highlighted that the subgroup analyses provide additional insights. In the forest plot, most subgroups showed no meaningful differences between treatment arms; however, the subgroup of patients with CIS demonstrated a trend toward benefit with the addition of atezolizumab to BCG, suggesting that this population may derive greater benefit from immune checkpoint inhibition.

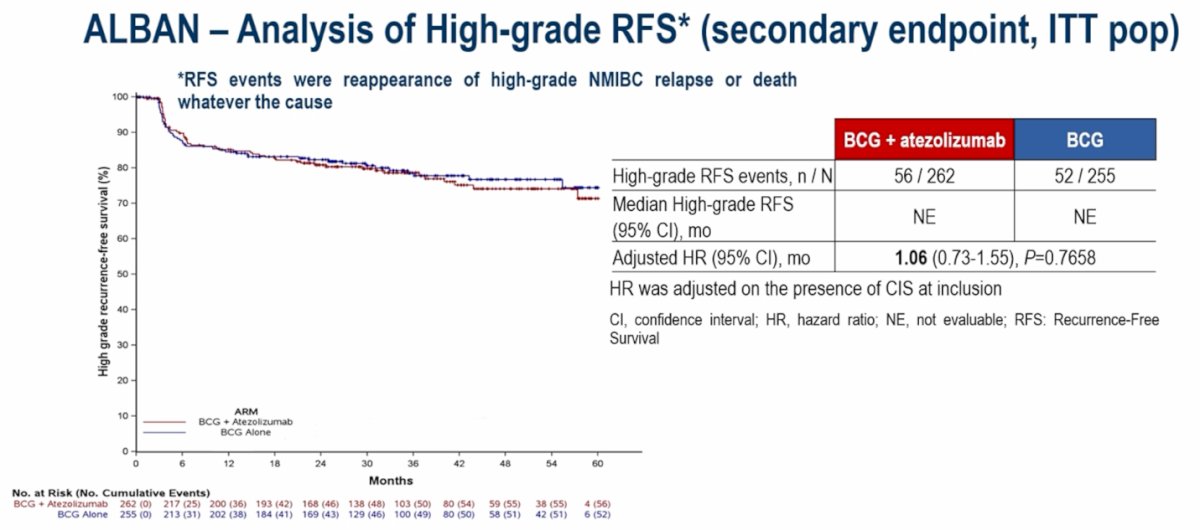
The secondary endpoint of high-grade recurrence-free survival (RFS) was also negative. High-grade RFS events occurred in 56 patients in the BCG plus atezolizumab arm and 52 in the BCG-alone arm, with an adjusted HR of 1.06 (95% CI 0.73–1.55; p=0.77), demonstrating no benefit with the addition of atezolizumab to BCG.
OS data was immature, so we can’t make any conclusions from the Kaplan Meier graphic below.

Regarding safety, Dr. Rouprêt noted that the systemic treatment with atezolizumab was administered for one year. Adverse events were more frequent in the combination arm, with any AEs reported in 98.8% of patients receiving BCG plus atezolizumab compared with 94.0% in the BCG-alone arm. Grade ≥3 AEs occurred in 40.0% versus 23.6%, respectively. Immune-related treatment-related adverse events were also more common with the addition of atezolizumab (54.9% vs 8.8%) as expected, although grade ≥3 immune-related events remained relatively infrequent (5.5% vs 1.2%). Treatment discontinuation due to adverse events occurred more often in the combination arm, reflecting the added systemic therapy exposure.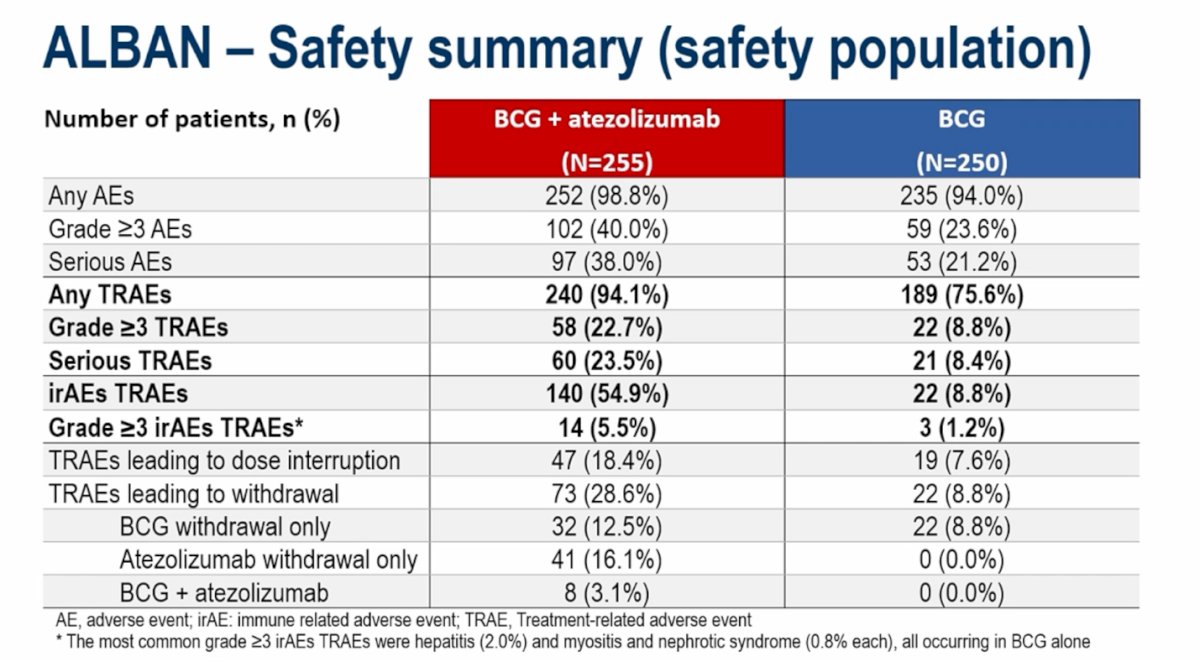
Dr. Rouprêt also noted that BCG reinduction was allowed at the discretion of the treating physician. Regarding safety, treatment-related adverse events were more frequent in the combination arm, although most were low grade. The most commonly reported events included urinary tract disorders, pollakiuria, hematuria, fatigue, and arthralgia, reflecting the expected toxicity profile associated with BCG-based therapy combined with systemic immunotherapy. Grade ≥3 events remained relatively uncommon across both groups, and there were no new safety signals compared to what we already know with the use of Atezolizumab in other trials of urothelial cancer.

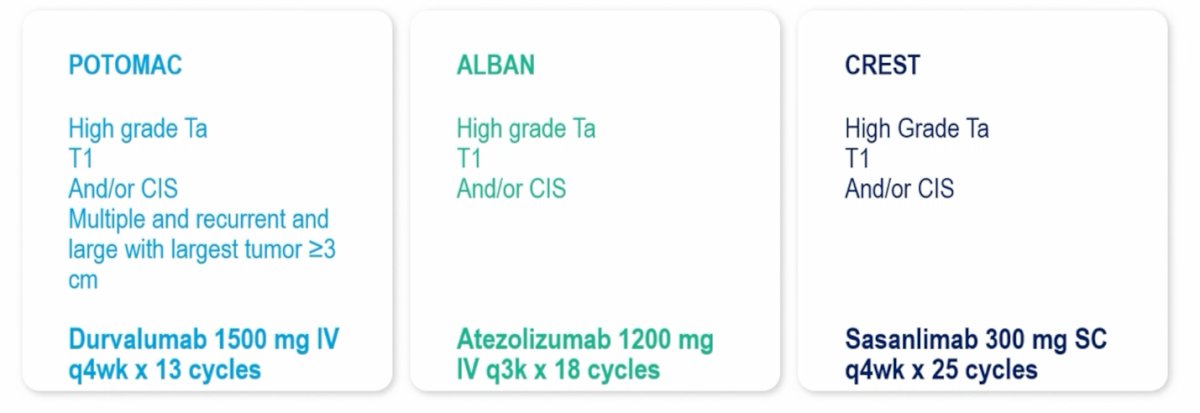
Dr. Rouprêt also compared the three trials and highlighted important differences in treatment exposure and duration of systemic therapy. In POTOMAC, durvalumab was administered at 1500 mg IV every 4 weeks for 13 cycles (approximately 1 year). In ALBAN, atezolizumab was given at 1200 mg IV every 3 weeks for up to 18 cycles. In contrast, the CREST trial evaluated sasanlimab 300 mg administered subcutaneously every 4 weeks for 25 cycles, resulting in a longer duration of treatment exposure compared with the other studies.
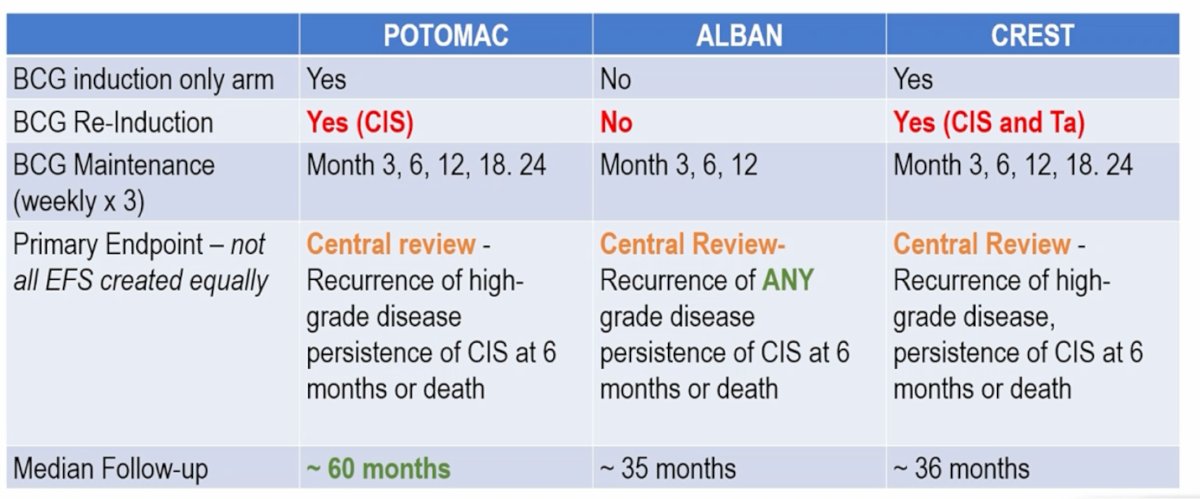
Importantly, Dr. Rouprêt highlighted several design differences across the three trials. ALBAN did not allow BCG reinduction, whereas reinduction was permitted in both POTOMAC (for CIS) and CREST (for CIS and Ta disease). Maintenance BCG schedules were also similar between POTOMAC and CREST, extending to months 3, 6, 12, 18, and 24, while ALBAN included a shorter maintenance schedule limited to months 3, 6, and 12. Another key distinction relates to follow-up duration. POTOMAC had the longest follow-up at approximately 60 months, compared with about 35–36 months in ALBAN and CREST.
Dr. Rouprêt concluded with the following key points:
- The addition of atezolizumab to BCG did not significantly improve event-free survival compared with BCG alone (HR 0.98; 95% CI 0.71–1.36; p=0.91).
- The safety profile of the combination was consistent with the known safety profiles of the individual agents.
- Higher rates of treatment-related adverse events and grade ≥3 treatment-related adverse events were observed in the combination arm compared with BCG alone.
Presented by: Morgan Rouprêt, MD, PhD, Professor of Urology, Pitié Salpêtrière Hospital, Sorbonne University, Paris, France
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Reference:- Roupret M, Bertaut A, Pignot G, Neuzillet Y, Houede N, Mathieu R, Corbel L, Besson D, Seisen T, Jaffrelot L, Lebacle C, Champiat S, Lebdai S, Timsit MO, Thibault C, Goeman L, Juárez Soto Á, La C, Léger C, Loriot Y. ALBAN (GETUG-AFU 37): a phase III, randomized, open-label international trial of intravenous atezolizumab and intravesical Bacillus Calmette-Guérin (BCG) versus BCG alone in BCG-naive high-risk, non-muscle-invasive bladder cancer (NMIBC). Ann Oncol. 2026 Jan;37(1):44-52. doi: 10.1016/j.annonc.2025.09.017. Epub 2025 Oct 17. PMID: 41110692.