(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., between March 13th and 16th 2026, was host to the BCG meets immunotherapy in high-risk NMIBC: Key lessons for urologists from POTOMAC, ALBAN, and CREST Thematic Session. Dr. Maria De Santis presented Trial Highlights: POTOMAC - Durvalumab + BCG (Positive trial).
Dr. De Santis began by emphasizing that the POTOMAC trial was designed to improve outcomes with BCG in patients with high-risk NMIBC. The current standard-of-care for these patients consists of transurethral resection of bladder tumour followed by BCG induction and maintenance therapy. Although BCG achieves high initial response rates, approximately 40% of patients experience early recurrence or progression within two years, and adherence to the recommended 2 to 3 years of maintenance BCG remains low in routine practice. Recurrence or progression despite BCG induction and maintenance remains a major clinical challenge, and according to the 2025 EAU guidelines, treatments other than radical cystectomy are considered oncologically inferior in patients with BCG-unresponsive disease. Based on this unmet need, the POTOMAC study evaluated whether combining durvalumab with BCG could improve long-term outcomes in patients with BCG-naive, high-risk NMIBC.1
Dr. De Santis explained the biological rationale behind the POTOMAC trial. BCG stimulates the immune system by initiating and expanding anti-tumor T-cell responses within the bladder microenvironment. In contrast, durvalumab, a PD-L1 inhibitor, enhances and prolongs the activity of cytotoxic T cells, potentially leading to a more durable anti-tumor response. She also highlighted translational data suggesting that PD-L1 expression may increase following BCG exposure, supporting the rationale for combining BCG with checkpoint inhibition in patients with high-risk NMIBC.2

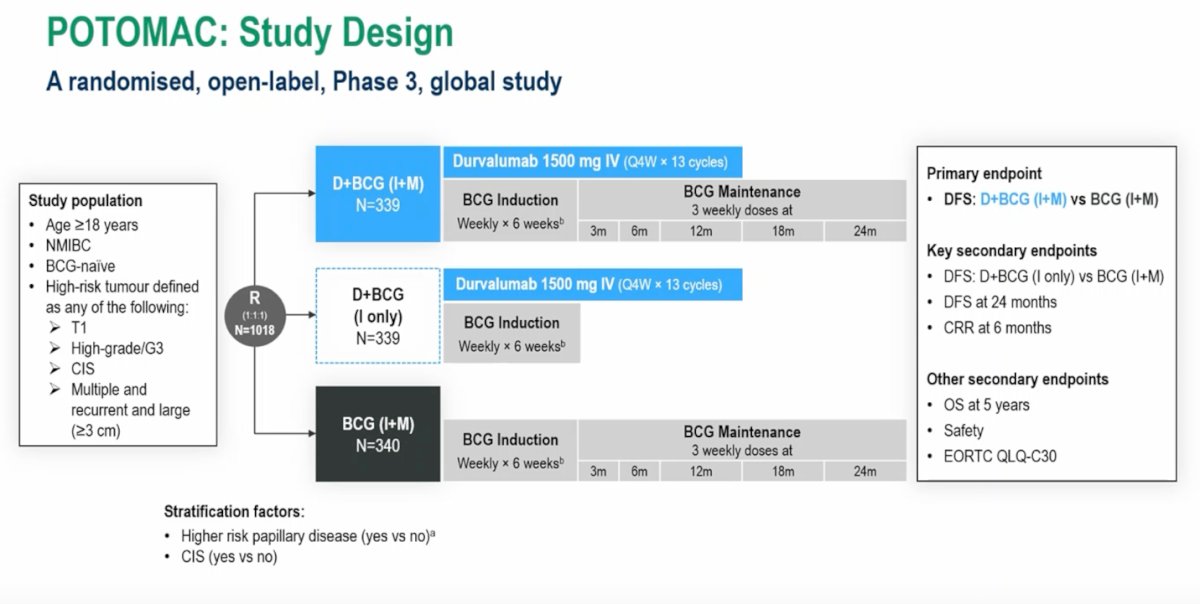
The POTOMAC study was a randomized, open-label, global phase III trial evaluating the addition of durvalumab to BCG in patients with BCG-naive, high-risk NMIBC. Eligible patients were adults with high-risk disease, including T1 tumors, high-grade Ta, carcinoma in situ, or multiple, recurrent, or large tumors (≥3 cm). A total of 1,018 patients were randomized 1:1:1 to one of three treatment arms: durvalumab plus BCG induction and maintenance, durvalumab plus BCG induction alone, or standard BCG induction and maintenance. Durvalumab was administered at 1500 mg intravenously every four weeks for up to 13 cycles. BCG induction consisted of weekly instillations for six weeks, followed by maintenance therapy at 3, 6, 12, 18, and 24 months in the maintenance arms.
The primary endpoint was disease-free survival comparing durvalumab plus BCG induction and maintenance versus BCG induction and maintenance alone. Key secondary endpoints included disease-free survival for durvalumab plus BCG induction alone versus BCG induction and maintenance, disease-free survival at 24 months, and complete response rate at six months, with additional endpoints including overall survival, safety, and patient-reported outcomes. The study design is shown below:
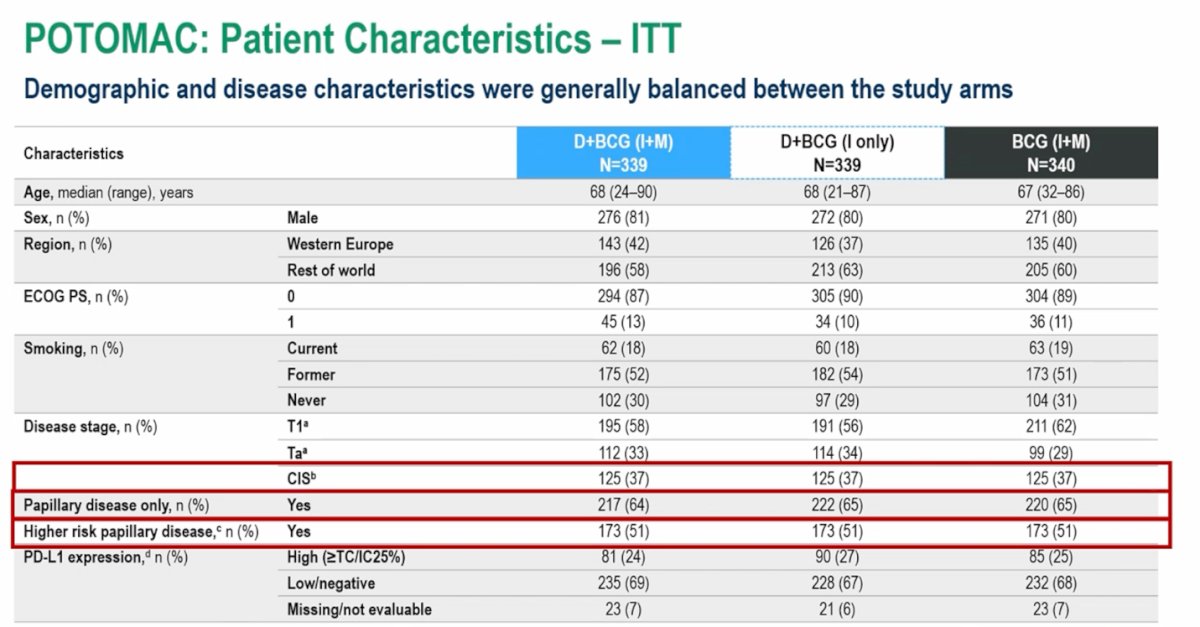
Baseline patient and disease characteristics were generally well-balanced across the three study arms. The median age was approximately 67–68 years, and about 80% of participants were male. Most patients had an ECOG performance status of 0, and the geographic distribution was similar across groups. In terms of disease characteristics, the population included a mix of high-risk NMIBC subtypes. Notably, approximately two-thirds of patients had papillary disease only, and about half of the overall cohort had higher-risk papillary disease.
BCG treatment exposure was similar between the durvalumab plus BCG induction and maintenance arm and the BCG induction and maintenance arm. Treatment compliance was high, with a median of six BCG instillations during induction and a median of 14 maintenance instillations in both groups. Overall, a substantial proportion of patients received prolonged BCG exposure, with approximately two-thirds completing at least 12 months of therapy and more than half reaching 18 months, indicating good adherence to the planned maintenance schedule across the study arms.

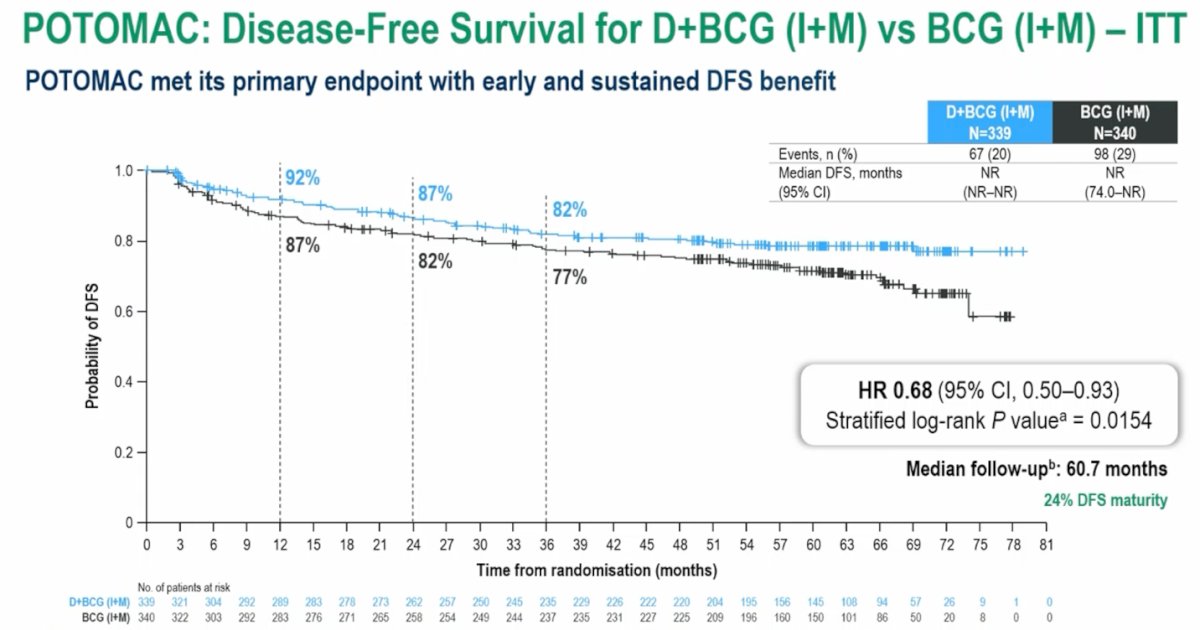
The POTOMAC trial met its primary endpoint, demonstrating a significant improvement in disease-free survival with the combination of durvalumab plus BCG induction and maintenance compared with BCG induction and maintenance alone. With a median follow-up of nearly 61 months, the addition of durvalumab reduced the risk of recurrence or progression by 32% (HR 0.68, 95% CI 0.50–0.93; p=0.0154). The benefit emerged early and was sustained over time, supporting the potential role of this combination strategy in patients with BCG-naive high-risk NMIBC.
Subgroup analyses demonstrated that the disease-free survival benefit with durvalumab plus BCG induction and maintenance was generally consistent across most predefined patient subgroups. The treatment effect appeared similar regardless of age, sex, geographic region, ECOG performance status, smoking status, BCG strain, and PD-L1 expression. Importantly, the benefit was observed both in patients with and without carcinoma in situ as well as among those with higher-risk papillary disease, supporting the robustness of the primary efficacy findings across different clinical subgroups.

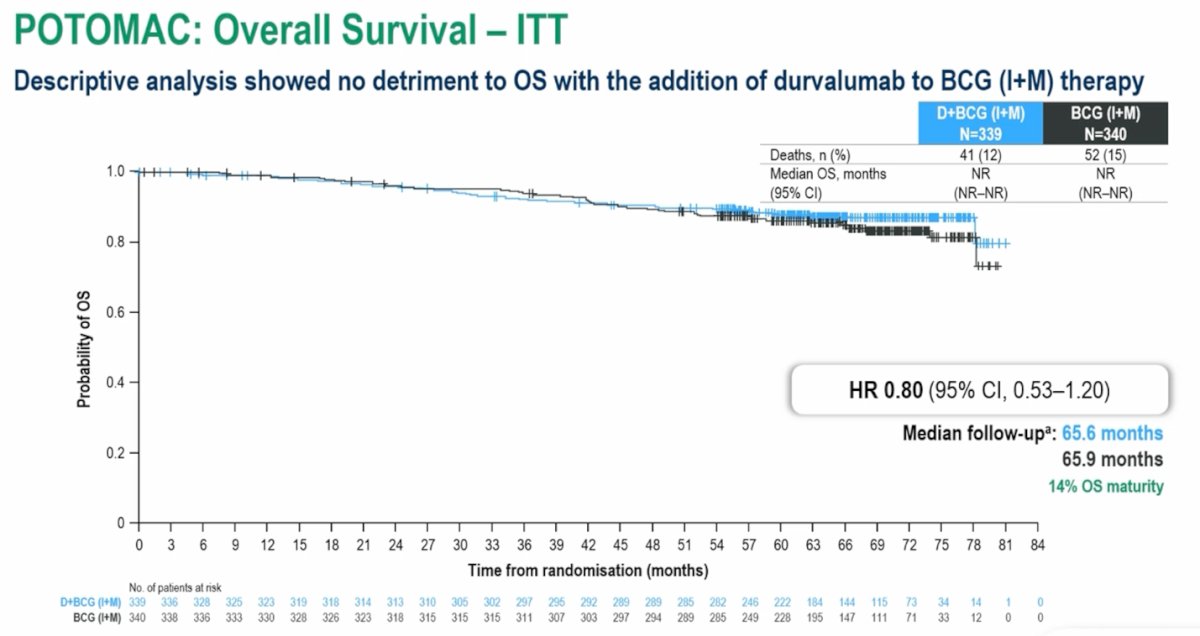
Overall survival was a secondary endpoint in the POTOMAC trial. At the time of this analysis, the data remain immature; however, a descriptive analysis showed no detriment to overall survival with the addition of durvalumab to BCG induction and maintenance therapy. With a median follow-up of approximately 66 months, the hazard ratio for overall survival was 0.80 (95% CI 0.53–1.20), although this data is still lacking maturity.
In a sensitivity analysis restricted to patients with papillary disease only, the disease-free survival results remained consistent with the overall study findings. The addition of durvalumab to BCG induction and maintenance continued to demonstrate a disease-free survival benefit compared with BCG alone, indicating that the overall DFS results were not driven by the presence of carcinoma in situ and were maintained in patients with papillary disease.

When examining the components of disease-free survival events, the addition of durvalumab to BCG induction and maintenance was associated with fewer total DFS events compared with BCG induction and maintenance alone. In particular, rates of high-risk disease recurrence were lower in the durvalumab plus BCG induction and maintenance arm. Persistent carcinoma in situ was uncommon across all treatment groups, occurring in only a small number of patients. The investigators also reported that 20 patients across the study received BCG re-induction, with most completing the full six planned doses. These findings further support the overall DFS benefit observed with the durvalumab plus BCG combination.

Several BCG strains were used across the study; however, this did not appear to impact the overall disease-free survival results, with consistent outcomes observed regardless of the BCG strain administered.
Adverse events with durvalumab plus BCG induction and maintenance were generally tolerable and manageable, with no unexpected safety signals. Dr. De Santis drew particular attention to immune-mediated adverse events, which occurred in 27% of patients receiving durvalumab of any grade, with grade 3–4 events observed in 8%. Importantly, no immune-related adverse events resulted in patient death.
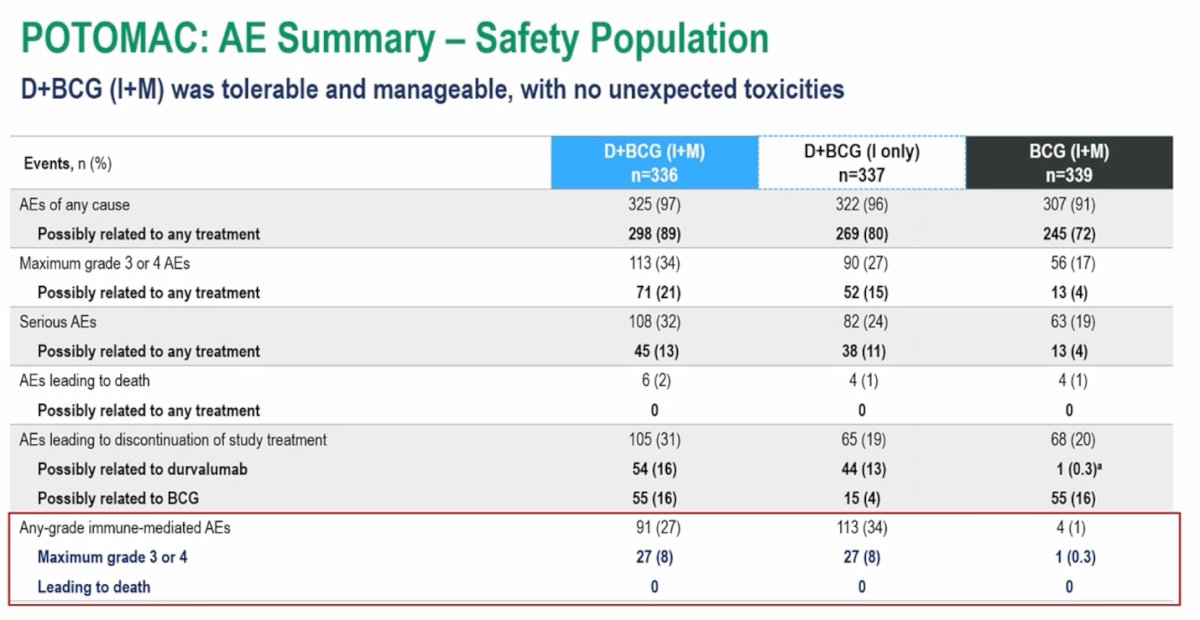
The overall safety profile was consistent with the known toxicities of the individual therapies. The most frequently reported adverse events were those typically associated with BCG therapy, including dysuria, hematuria, pollakiuria, urinary tract infection, and cystitis.

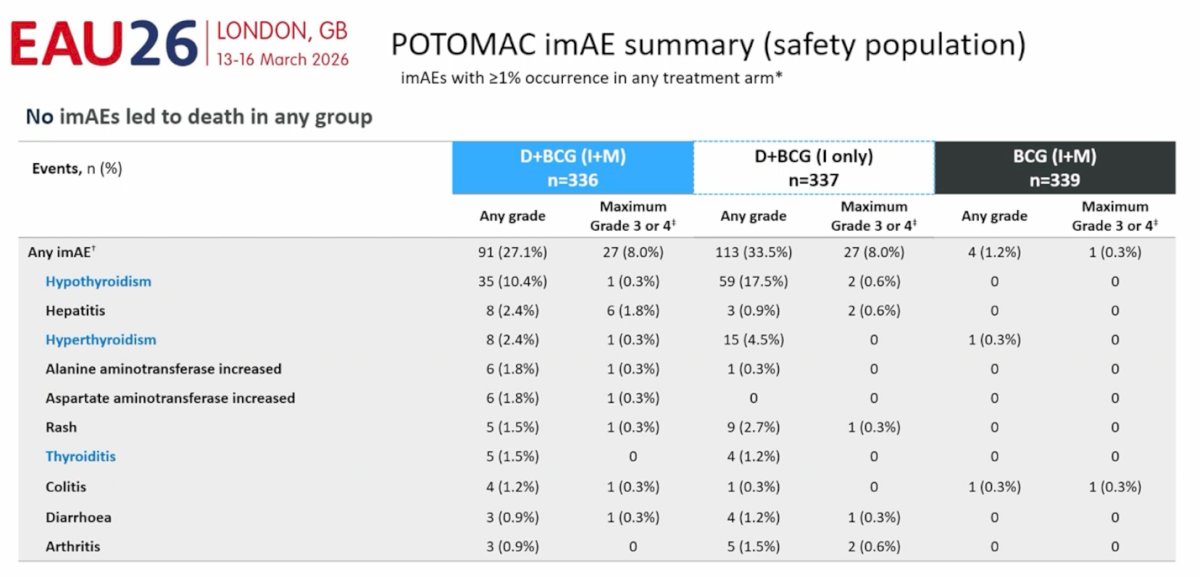
An overview of immune-mediated adverse events showed that these events were more frequent in the arms receiving durvalumab, as expected with checkpoint inhibition. In the durvalumab plus BCG induction and maintenance arm, immune-mediated adverse events of any grade occurred in approximately 27% of patients, with grade 3–4 events observed in about 8%. The most commonly reported immune-mediated events included hypothyroidism, hepatitis, hyperthyroidism (44%), and rash. Importantly, no immune-mediated adverse events resulted in death in any treatment group.
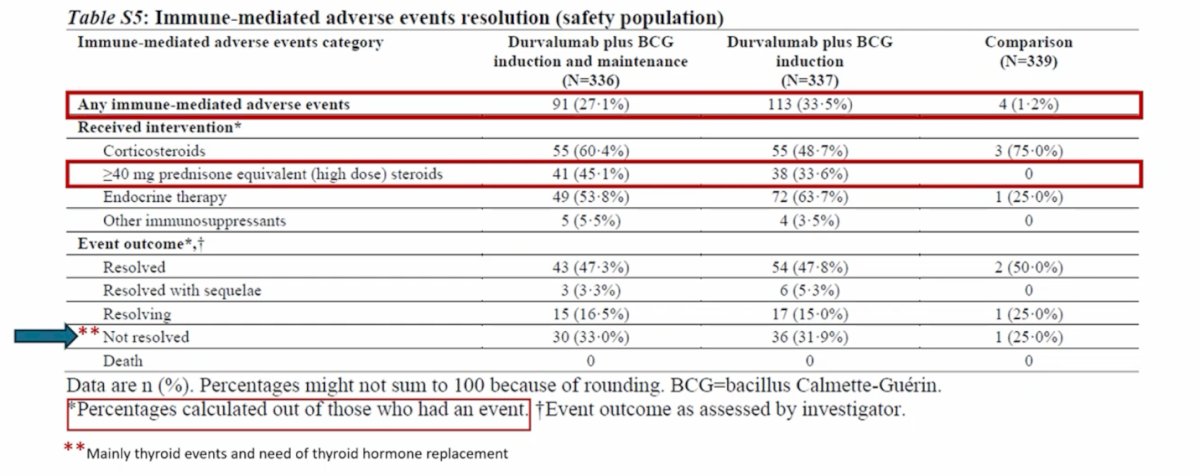
In the durvalumab plus BCG induction and maintenance arm, immune-related adverse events occurred in 27% of patients. Among those who developed these events, approximately 45% required high-dose corticosteroids, defined as more than 40 mg of prednisone or equivalent, underscoring the need for close monitoring and appropriate management of immune-related toxicity when adding checkpoint inhibition to BCG therapy.
Dr. De Santis concluded with several key points:
- The POTOMAC trial demonstrated that durvalumab combined with BCG induction and maintenance significantly improved disease-free survival compared with BCG induction and maintenance alone in patients with BCG-naive, high-risk NMIBC.
- The combination resulted in a 32% reduction in the risk of disease-free survival events (HR 0.68; 95% CI 0.50–0.93; p=0.0154).
- The DFS benefit emerged early, within the first four months, and was sustained over time with more than five years of follow-up.
- Overall survival data remain immature; however, descriptive analysis showed no detriment to OS with the addition of durvalumab (HR 0.80; 95% CI 0.53–1.20).
- The safety profile of durvalumab plus BCG induction and maintenance was tolerable and manageable, consistent with the known safety profiles of the individual therapies, and no treatment-related deaths were reported.
- Based on these findings, the POTOMAC trial supports the use of one year of durvalumab in combination with BCG induction and maintenance as a potential new treatment strategy for patients with BCG-naive, high-risk NMIBC.
Presented by: Maria De Santis, MD, PhD, Medical Oncologist, Section Head, Interdisciplinary GU-Oncology, Charité Universitätsmedizin Berlin, Berlin, Germany; Paracelsus Medizinische Privatuniversität, Salzburg, Austria; University of Warwick, Warwick, England
References:
- De Santis M, Palou Redorta J, Nishiyama H, Krawczyński M, Seyitkuliev A, Novikov A, Guerrero-Ramos F, Zukov R, Kato M, Kawahara T, Goeman L, Puente J, Hellmis E, Powles T, Radziszewski P, Gust KM, Vasey P, Bigot P, Fradet Y, Hunting J, Armstrong J, Boulos S, Hois S, Shore ND; POTOMAC Investigators. Durvalumab in combination with BCG for BCG-naive, high-risk, non-muscle-invasive bladder cancer (POTOMAC): final analysis of a randomised, open-label, phase 3 trial. Lancet. 2025 Nov 8;406(10516):2221-2234. doi: 10.1016/S0140-6736(25)01897-5. Epub 2025 Oct 17. PMID: 41115436.
- Maas M, Hilsendecker A, Pertoll A, Stühler V, Walz S, Rausch S, Stenzl A, Tsaur I, Hennenlotter J, Aufderklamm S. PD-L1 Expression in High-Risk Non-Muscle-Invasive Bladder Cancer Is Influenced by Intravesical Bacillus Calmette-Guérin (BCG) Therapy. Cancers (Basel). 2024 Mar 29;16(7):1356. doi: 10.3390/cancers16071356. PMID: 38611034; PMCID: PMC11011000.