(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a metastatic urothelial carcinoma session and a presentation by Dr. Melanie Hassler-Di Fratta discussing real-world treatment outcomes of enfortumab vedotin + pembrolizumab in lymph node–positive urothelial carcinoma patients fit for cystectomy. Enfortumab vedotin + pembrolizumab has shown promising efficacy in locally advanced or metastatic urothelial carcinoma, leading to approval as a first-line treatment.1
However, real-world data focusing specifically on lymph node–only positive patients that may be considered for multimodal treatment approaches, such as consolidative surgery, remains limited. As such, at EAU 2026, Dr. Hassler-Di Fratta and colleagues reported outcomes from a multicenter registry (n = 203) evaluating enfortumab vedotin + pembrolizumab in this population.
This retrospective analysis included 45 consecutive patients with lymph node-positive urothelial carcinoma and ECOG performance status 0 or 1 treated with enfortumab vedotin + pembrolizumab across 16 Austrian centers. Baseline clinical characteristics, treatment fitness, comorbidity (Charlson Comorbidity Index; CCI), local interventions, and response according to RECIST criteria were collected. The best overall response was determined radiographically.
The median age was 71 years (range: 27-93), and 71.1% were male. Most patients were platinum-fit (71.1%) and had low comorbidity (CCI 80%). Lymph node involvement was regional in 55.6%, non-regional in 15.5%, and both in 28.9% of cases:
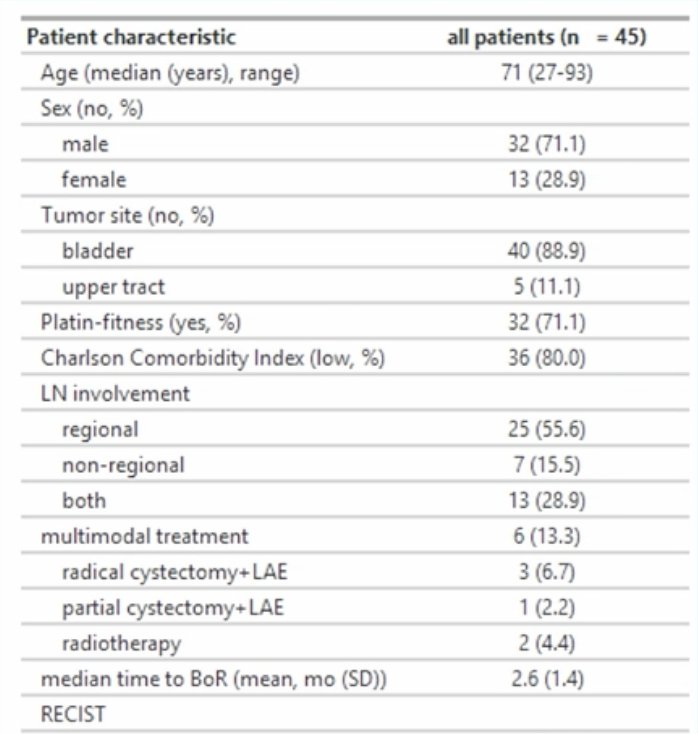
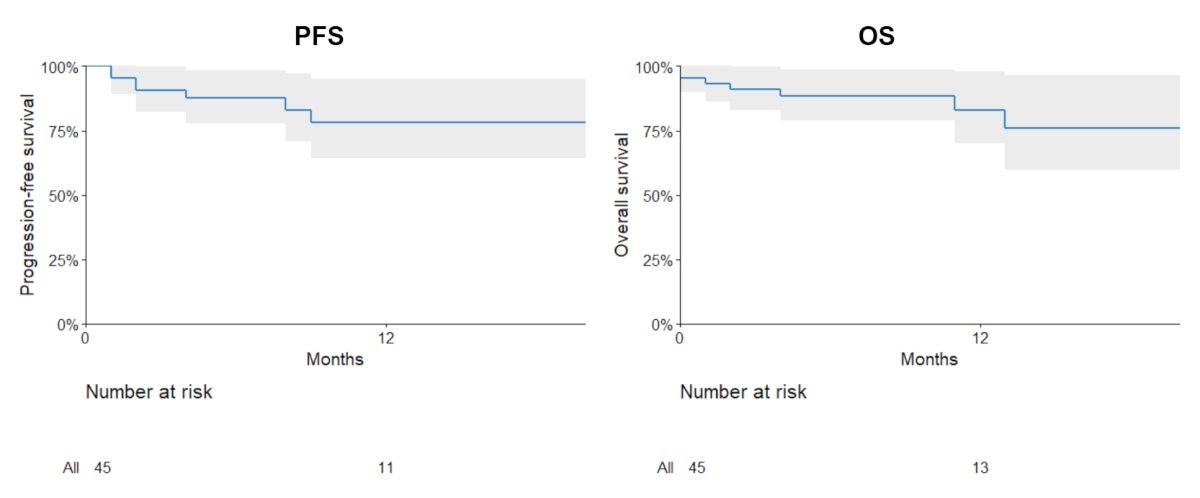
At the time of data cut-off, 84% of patients were alive, with a median time to best overall response after enfortumab vedotin + pembrolizumab initiation of 2.6 months. The objective response rate (complete response + partial response) was 80%, with 37.8% achieving complete response and 42.2% partial response. Moreover, stable disease was observed in 4.5% and progressive disease in 11.4% of patients. After a median follow-up of 7.9 months, the median overall survival and progression-free survival were not reached:
There were 6 patients (13.3%) who received multimodal treatment, of whom patients were generally younger (mean age: 61 years), and 4 patients (8.9%) who underwent consolidative surgery. Pathological downstaging was noted in 3 patients (75%), with no pathological complete responses. Overall, 3 of 4 patients had Clavien Dindo grade 3 complications. On follow-up for these 4 patients (6-12 months), 3 have had a complete response, and 1 patient had a local recurrence.
Dr. Hassler-Di Fratta concluded her presentation discussing real-world treatment outcomes of enfortumab vedotin + pembrolizumab in lymph node–positive urothelial carcinoma patients fit for cystectomy with the following take-home points:
- In this real-world cohort of lymph node-positive urothelial carcinoma patients, enfortumab vedotin + pembrolizumab demonstrated high and rapid response rates consistent with pivotal clinical trial data
- The combination yielded an objective response rate of nearly 80% and a complete response in approximately 40% of patients
- These findings support enfortumab vedotin + pembrolizumab as a highly effective first-line treatment option for lymph node-positive urothelial carcinoma in everyday clinical practice
- Further follow-up will clarify the durability of response, survival outcomes, and the oncological benefit of local consolidative interventions
Presented by: Melanie R. Hassler-Di Fratta, MD, PhD, Medical University of Vienna, Vienna, Austria
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Reference: