(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured an innovations in muscle invasive bladder cancer management session and a presentation by Dr. Vera Rutten discussing interim results of the CHASIT study assessing sequential chemo-immunotherapy in patients with locally advanced urothelial cancer. Patients with locally advanced unresectable or clinically node-positive urothelial cancer have a poor outcome.
The recommended treatment with curative intent is platinum-based induction chemotherapy, followed by radical surgery of the primary tumor and locoregional lymph nodes in patients who experience radiological response to induction chemotherapy. Long-term survival strongly depends on the absence of residual tumor in the surgical resection specimen, for example, a pathological complete response. The reported pathological complete response rate following induction chemotherapy in locally advanced or clinically node-positive urothelial cancer is quite poor at ~15%. This dictates long-term outcomes, with a 5-year overall survival rate for patients with pathological complete response of 70–80% versus 15-20% for patients who have residual disease or nodal metastases. This clearly demonstrates the unmet need to improve the clinical outcomes of these patients. The JAVELIN Bladder 100 study demonstrated an overall survival benefit of sequential chemotherapy-immunotherapy in patients with metastatic urothelial cancer.1 As such, the CHASIT study investigates the efficacy and safety of sequential chemotherapy-immunotherapy in patients with locally advanced or clinically node-positive urothelial cancer who are fit for surgery. In addition, patient biomaterials are collected to investigate mechanisms of response and resistance to chemotherapy-immunotherapy.
This multicenter, prospective phase II clinical trial includes patients with stage cT4bNxM0 or cTxN1-N3M0 urothelial cancer of the bladder, upper urinary tract, or urethra. Patients who do not experience disease progression following 3 or 4 cycles of platinum-based chemotherapy are eligible for inclusion and receive 3 cycles of avelumab (anti-PD-L1 immunotherapy) followed by radical surgery:
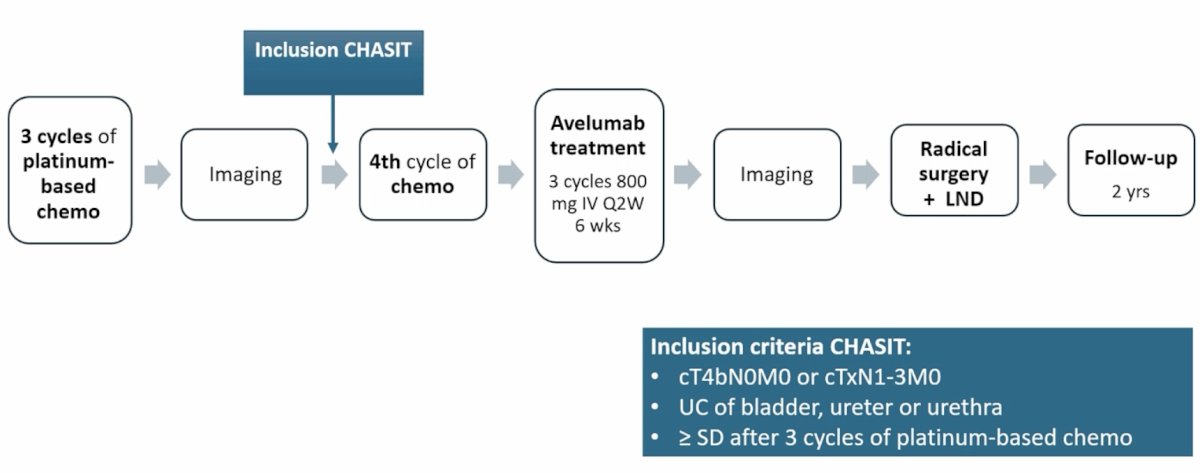
The primary endpoint is the pathological complete response rate, defined as the absence of residual tumor in the resection specimen, carcinoma in situ is allowed (ypT0N0/ypTisN0). Given the historical pathological complete response rate of 15%, the hypothesis is that pathological complete response will be > 30% in CHASIT. Secondary endpoints include: toxicity, surgical complications, progression-free survival, cancer-specific survival, and overall survival at 24 months. An interim analysis is planned after 40 inclusions, and if the pathological complete response rate is <15%, the study will terminate early due to insufficient efficacy.
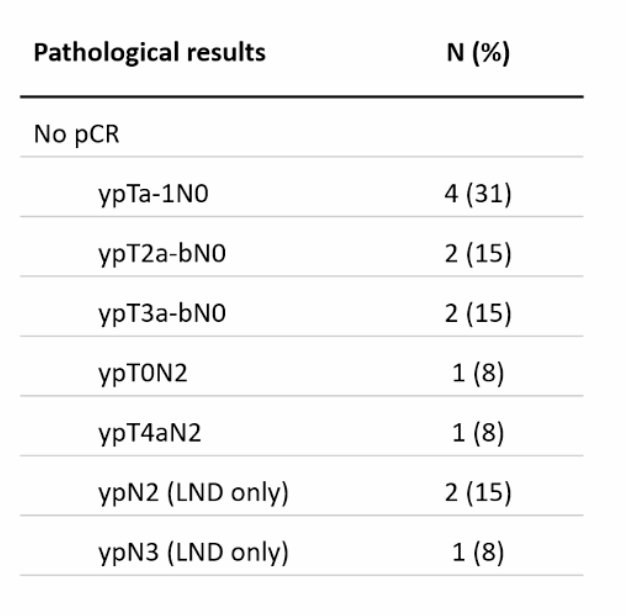
The interim analysis reports the first 40 patients included, with a mean age of 67 years, and 85% male. The primary tumor was located in the bladder (90%), upper urinary tract (8%), or urethra (3%). Most patients presented with cN2 disease (63%), followed by cN3 (18%), cN1 (15%), and cT4bN0 (5%). Induction chemotherapy was platinum-based (53% gemcitabine + cisplatin; 30% gemcitabine + carboplatin), and all patients received 3-4 cycles. Overall, 90% of patients completed 3 cycles of avelumab, and 25% of patients had disease progression during avelumab treatment, therefore precluding surgery. There were 75% of patients eligible for radical surgery, and 1 patient refused. In the intention-to-treat population, the pathological complete response rate was 40% (16/40), with the following pathological results for those who did not have a pathological complete response:
Dr. Rutten concluded her presentation discussing interim results of the CHASIT study with the following take-home points:
- The study is ongoing
- Progression after avelumab was higher than expected (25%), but consistent with the literature (2-27%)
- Biomaterial analyses will be conducted to explore differences between those having a pathological response, those without a pathological response, and those having disease progression
Presented by: Vera C. Rutten, Erasmus MC Cancer Institute, Rotterdam, The Netherlands
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Reference:
- Powles T, Park SH, Voog E, et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N Engl J Med 2020 Sept 24;383(13):1218-1230.