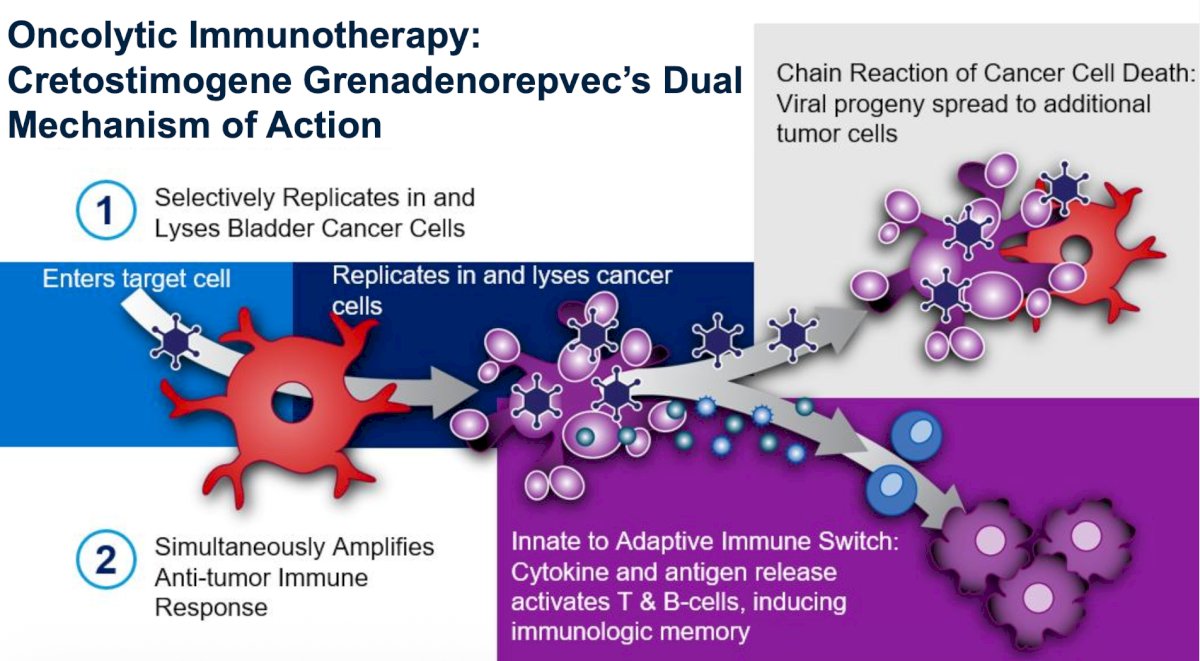
(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a urology trials in bladder and prostate cancer session and a presentation by Dr. Trinity Bivalacqua discussing CORE-008 Cohort B evaluating intravesical cretostimogene grenadenorepvec in patients with high risk BCG-exposed non muscle invasive bladder cancer. Patients with high-risk non muscle invasive bladder cancer whose disease trajectory falls outside the strict FDA guidance of BCG-unresponsive represent a significant unmet need, often lacking access to clinical trials or evidence-based treatment options. Cretostimogene grenadenorepvec is an oncolytic immunotherapy with dual mechanisms of action. It replicates in and lyses cancer cells with Rb-E2F pathway alterations, while simultaneously amplifying an anti-tumor immune response, further mediated by the GM-CSF transgene:
The CORE-008 clinical trial (NCT06567743) is a phase 2, multi-arm, multi-cohort trial that evaluates the efficacy and safety of cretostimogene in patients with high risk non muscle invasive bladder cancer, across BCG-naïve, BCG-exposed, and BCG-unresponsive disease states.

At EAU 2026, Dr. Bivalacqua and colleagues discussed Cohort B of CORE-008, which is designed in conjunction with the SUO-CTC, to examine the efficacy and safety of cretostimogene in BCG-exposed non muscle invasive bladder cancer.
Cohort B eligibility criteria include pathologic confirmation of high risk non muscle invasive bladder cancer, CIS containing and papillary only, as defined by the AUA/SUO guidelines, and recurrence after prior BCG. BCG-exposed non muscle invasive bladder cancer is defined as high-grade recurrence in patients who are BCG-resistant (recurrence after at least 5 of 6 induction doses), or who experience delayed relapse within 24 months following either adequate BCG (≥5 induction doses plus ≥2 reinduction or maintenance doses) but outside the defined BCG-Unresponsive window or following inadequate BCG (3–6 doses). Intravesical cretostimogene is instilled in combination with DDM, an excipient that enhances adenoviral delivery, for six weekly doses during the induction phase, followed by three weekly maintenance cycles quarterly through month 12, then every six months through month 36. Re-induction is permitted at month 3, if persistent HG Ta or CIS is biopsy-confirmed:
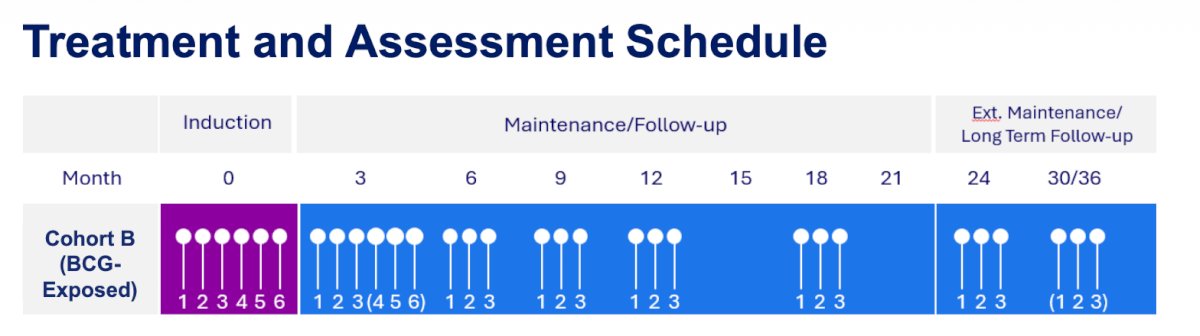
Response assessment includes cystoscopy and cytology every 3 months, with mandatory mapping biopsies at 12 months. A CT or MRU is performed every 6 months, and treatment is optional in year 3. The primary endpoint is complete response at any time for the CIS population and high grade event free survival for patients with papillary-only disease. Secondary endpoints include duration of response, all-cause event free survival, bladder cancer specific survival, progression free survival, cystectomy free survival, safety, and tolerability. Exploratory outcome measures consist of health-related quality of life, overall survival, and biomarker assessments. Cohort B is actively enrolling patients in collaboration with the SUO-CTC.
Presented by: Trinity Bivalacqua, MD, PhD, Penn Medicine, Philadelphia, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.