(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., was host to the Urothelial Cancer: Towards Integrated Therapeutic Strategies plenary session. Dr. Alexandre Zlotta delivered the state-of-the-art lecture Who Really Needs Surgery after Neo-adjuvant Chemotherapy?
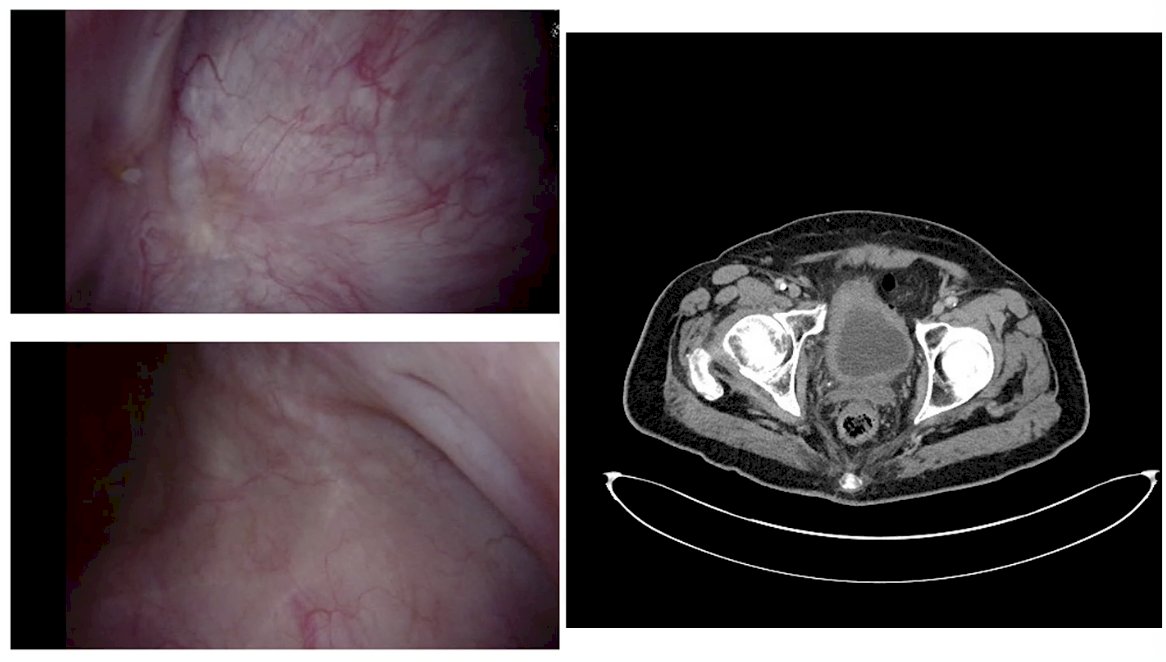
Dr. Zlotta began his presentation by presenting a case from the Princess Margaret Cancer Centre (PMCC) multidisciplinary bladder cancer clinic involving a 71-year-old gentleman with multiple comorbidities including chronic kidney disease (eGFR 46 ml/min) with muscle invasive bladder cancer treated with enfortumab vedotin plus pembrolizumab. Follow-up cystoscopy and CT imaging after treatment demonstrated a significant response, as illustrated in the images shown. The question that we aim to answer is what we offer these patients. In this case, and after multidisciplinary discussion, the team recommended consolidative treatment, and the patient elected to proceed with trimodality therapy (TMT). He remains disease-free on follow-up.
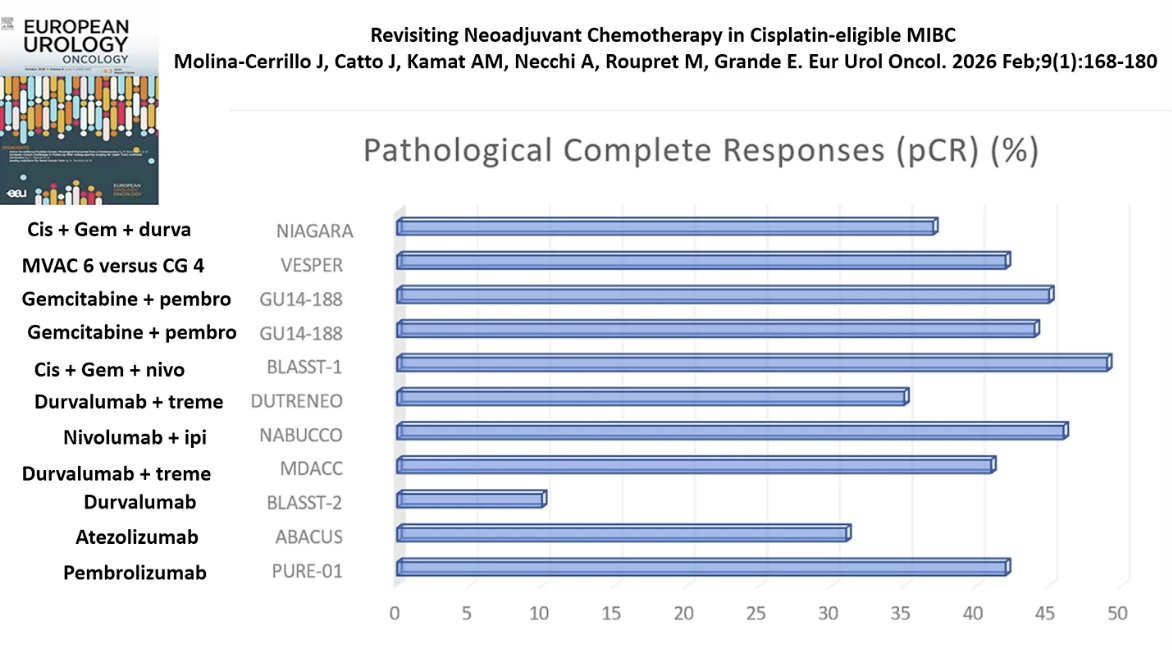
Dr. Zlotta also highlighted that adding immunotherapy to chemotherapy in the neoadjuvant setting can increase pCR rates compared with chemotherapy alone, we thought these responses most likely won’t reach 50%. He presented data across several studies combining chemotherapy with immune checkpoint inhibitors, including regimens such as cisplatin–gemcitabine with durvalumab or nivolumab, as well as gemcitabine-based combinations with pembrolizumab as illustrated below.
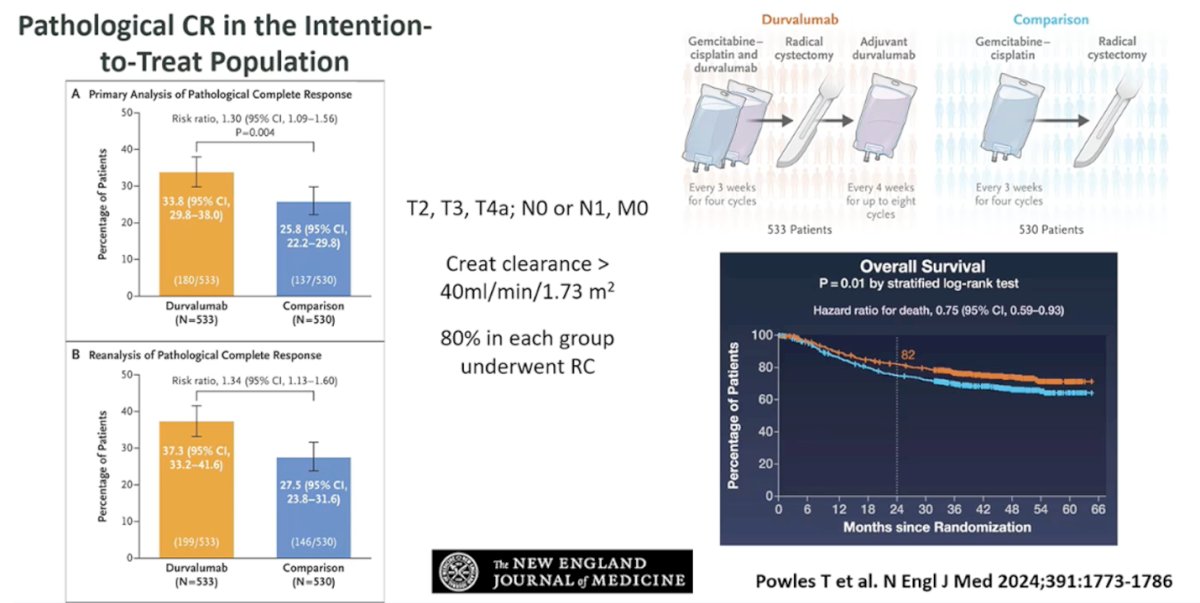
He further highlighted results from the NIAGARA trial, where the addition of durvalumab to neoadjuvant cisplatin–gemcitabine increased pathologic complete response rates by approximately 12% compared with chemotherapy alone. In the intention-to-treat population, pCR rates were 33.8% with durvalumab versus 25.8% in the control arm, reinforcing the incremental benefit of integrating immunotherapy into neoadjuvant treatment strategies for cisplatin-eligible MIBC. (1)
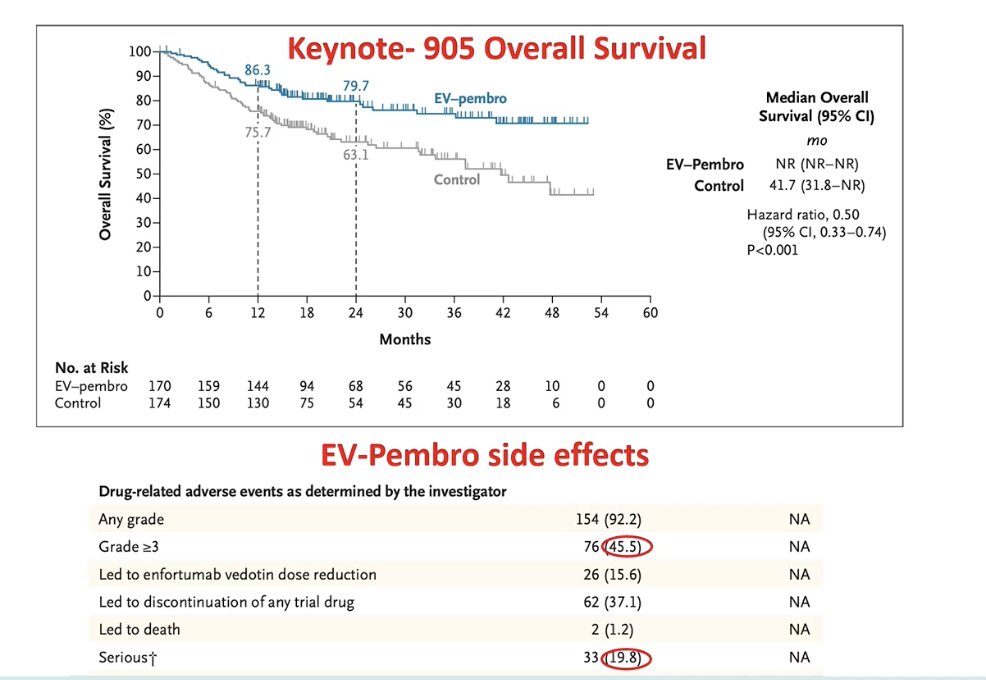
Dr. Zlotta then discussed emerging perioperative treatment combinations, beginning with the KEYNOTE-905/EV-303 study evaluating enfortumab vedotin plus pembrolizumab in patients with MIBC who were ineligible for or declined cisplatin-based chemotherapy. (2) He noted that this population reflects many patients encountered in routine practice, including those with impaired renal function. Notably, more than 40% of patients in each treatment arm had a creatinine clearance ≥60 mL/min, highlighting the heterogeneity of patients considered cisplatin-ineligible in contemporary clinical trials.
The combination of enfortumab vedotin plus pembrolizumab demonstrated a markedly higher pCR rate compared with the control arm, with pCR achieved in 57.1% of patients versus 8.6%, corresponding to an estimated difference of 48.3% (95% CI 39.5–56.5; p<0.00001). Notably, surgery was performed in the majority of patients in both groups, occurring in 87.6% of participants in the EV–pembrolizumab arm and 89.7% in the control arm. (2)

Moreover, this improvement translated into a significant overall survival benefit, with EV–pembrolizumab demonstrating superior survival compared with the control arm (HR 0.50, 95% CI 0.33–0.74; p<0.001), while the median overall survival had not yet been reached in the EV–pembrolizumab group. However, treatment-related adverse events remained considerable, with grade ≥3 events occurring in 45.5% of patients and serious adverse events reported in 19.8%, underscoring the need to carefully balance efficacy with toxicity when considering these intensified perioperative strategies. (2)
He then highlighted the recently presented KEYNOTE-B15 study, a phase III randomized trial evaluating perioperative enfortumab vedotin plus pembrolizumab in patients with cisplatin-eligible MIBC undergoing radical cystectomy and pelvic lymph node dissection. In this study, patients were randomized to receive neoadjuvant EV plus pembrolizumab followed by surgery and adjuvant EV plus pembrolizumab, versus standard neoadjuvant cisplatin–gemcitabine followed by surgery and observation. The trial design is shown below.
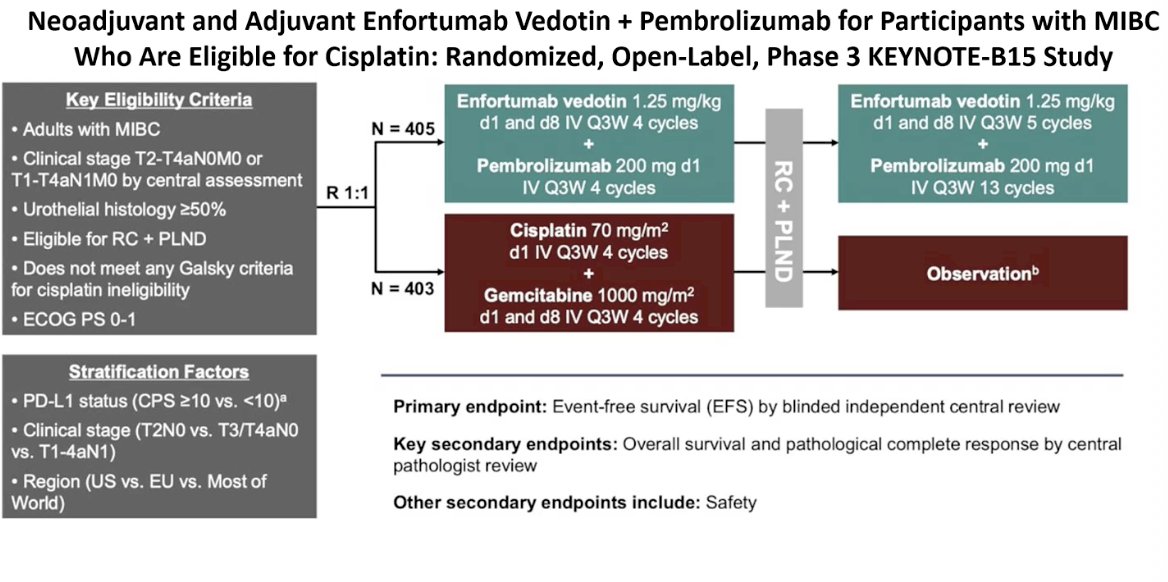
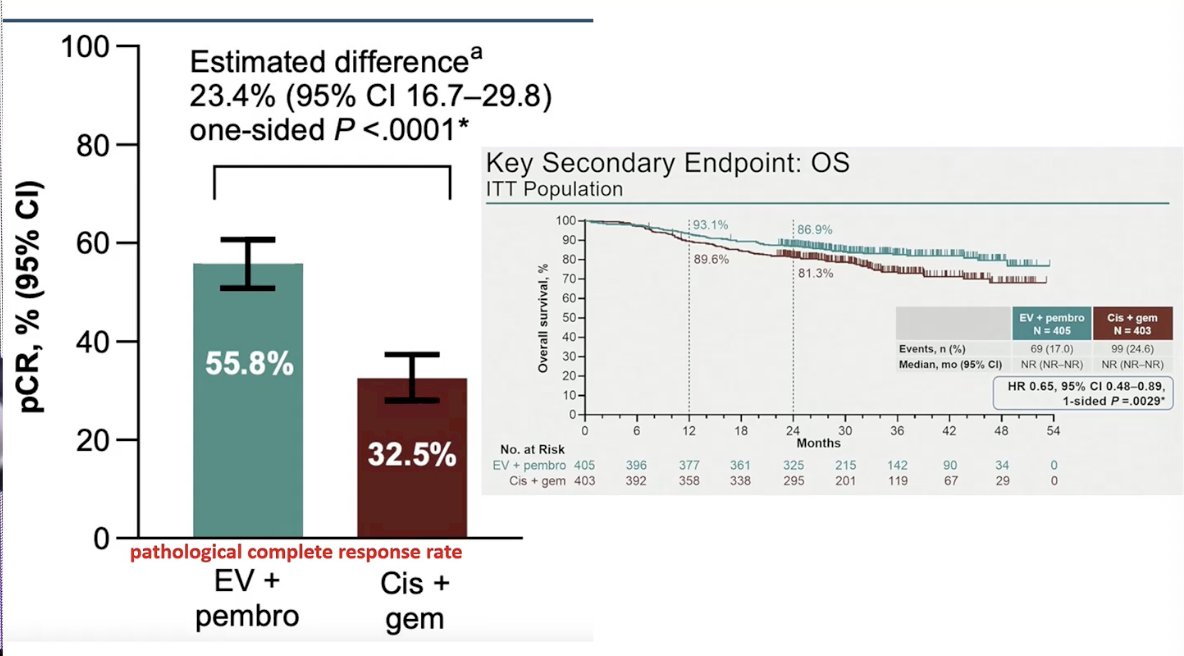
Notably, in the cisplatin-eligible population, pCR was achieved in 55.8% of patients treated with EV plus pembrolizumab compared with 32.5% in the cisplatin–gemcitabine control arm, corresponding to an estimated difference of 23.4% (95% CI 16.7–29.8; p<0.0001). This improvement also translated into a survival benefit, as reflected in the Kaplan–Meier curves demonstrating improved overall survival for the EV–pembrolizumab arm compared with standard chemotherapy.
An important question raised by these high complete response rates is whether all patients still require immediate surgery. Dr. Zlotta discussed the RETAIN-1 and RETAIN-2 studies, which explored active surveillance strategies after neoadjuvant therapy. In these studies, ctDNA appeared to discriminate between patients at higher risk of relapse and those more likely to remain cancer-free. Among patients managed with surveillance, outcomes suggested that ctDNA status could help identify those who may safely defer immediate cystectomy while closely monitoring for recurrence.
An important question raised by these high complete response rates is whether all patients still require immediate surgery. Dr. Zlotta discussed the RETAIN-1 and RETAIN-2 studies, which explored active surveillance strategies after neoadjuvant therapy. Compared to RETAIN-1, the ypT0 rate was higher at 40% and the combined rate of pT0 plus cCR reached 54% in RETAIN-2, suggesting a potential additive benefit from the addition of nivolumab to ddMVAC. Importantly, ctDNA appeared to discriminate between patients at higher risk of relapse and those more likely to remain cancer-free, highlighting its potential role in guiding surveillance strategies after neoadjuvant treatment.

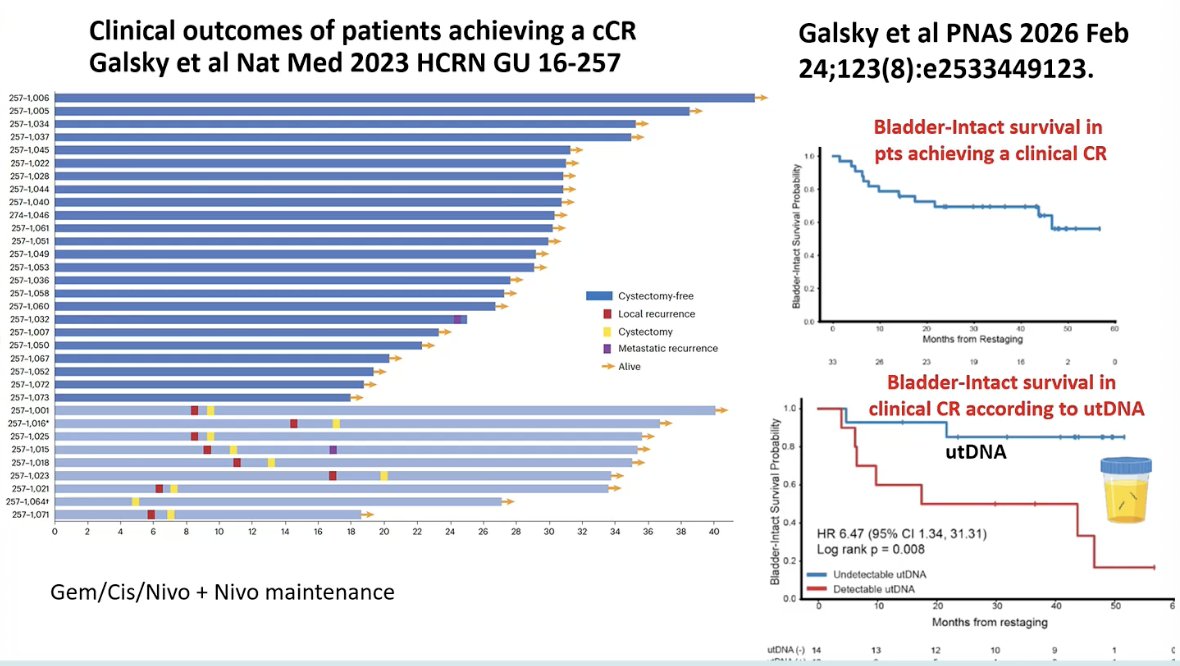
Dr. Zlotta also highlighted recently published data from Matt Galsky and colleagues evaluating outcomes among patients achieving a clinical complete response after systemic therapy. In this cohort, bladder-intact survival among patients with a cCR was approximately 47%. Importantly, outcomes differed significantly according to urinary tumor DNA (utDNA) status. As shown in the Kaplan–Meier curves, patients with undetectable utDNA demonstrated substantially better bladder-intact survival, whereas those with detectable utDNA experienced a markedly higher risk of recurrence and loss of bladder preservation (HR 6.47, 95% CI 1.34–31.31; p=0.008). (3) These findings suggest that utDNA may serve as an important biomarker to help identify which patients achieving a clinical complete response could safely pursue bladder-preserving strategies.
He then turned to where the field is heading next, noting that there remains a paucity of data on TMT after a cCR, particularly because much of the existing TMT literature comes from patients who were not managed in the context of contemporary systemic therapy or biomarker-driven selection. He highlighted several ongoing efforts aimed at improving TMT outcomes, including SWOG/NRG 1806 evaluating TMT with or without atezolizumab, KEYNOTE-992 comparing TMT plus placebo versus TMT plus pembrolizumab, and the CONsolidate trial exploring concurrent radiotherapy with enfortumab vedotin for locally advanced bladder cancer. Together, these studies reflect an effort to better integrate systemic therapy, radiation, and biomarkers such as ctDNA and utDNA into more refined bladder-preserving strategies.
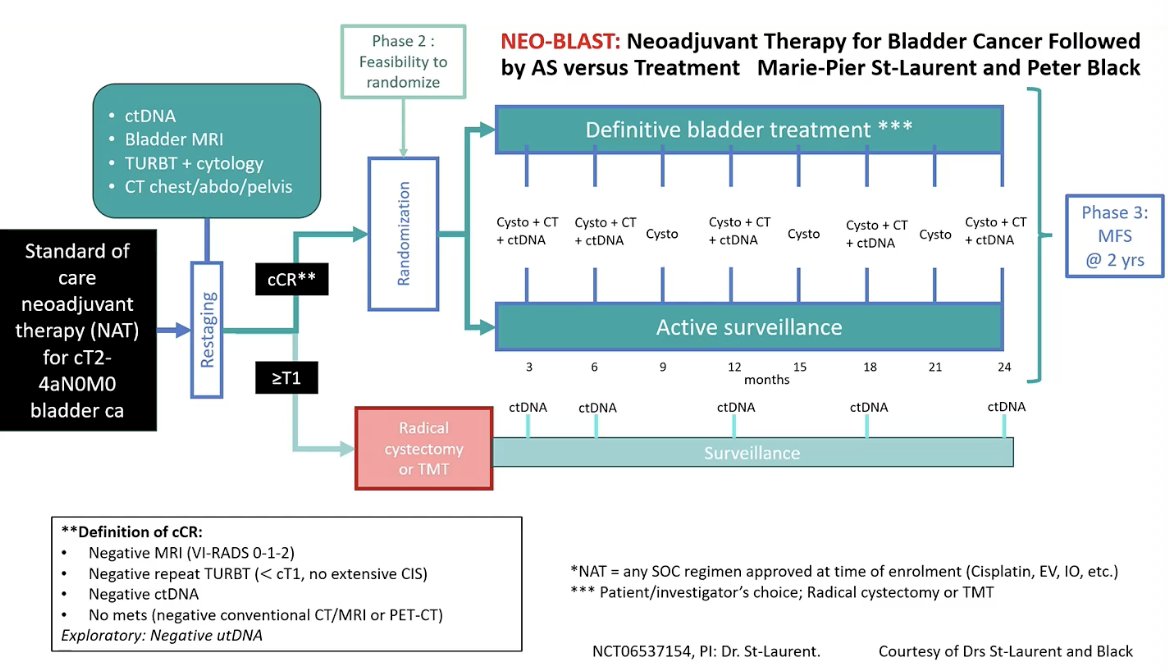
Dr. Zlotta highlighted the NeoBLAST study from Vancouver, designed to evaluate whether patients achieving a deep response after neoadjuvant therapy can safely avoid immediate surgery. Patients with cT2–T4aN0M0 disease undergo neoadjuvant treatment followed by restaging with MRI, repeat TURBT, CT imaging, and ctDNA. Those achieving a clinical complete response are randomized to definitive bladder treatment (RC or TMT) versus active surveillance with close monitoring using cystoscopy, imaging, and ctDNA. He emphasized that trials like NeoBLAST are exactly the type of prospective studies needed to define bladder-preserving strategies in the modern treatment era.
Dr. Zlotta concluded by discussing how treatment decisions after neoadjuvant therapy may increasingly be guided by comprehensive clinical restaging. The figure below highlights how the future of MIBC could potentially look. The approach integrates cystoscopy, biopsy/TURBT, urine cytology, MRI, urinary tumor DNA, and ctDNA. In patients achieving a clinical complete response with favorable biomarkers (VI-RADS <1, utDNA negative, ctDNA negative), omission of local therapy may become possible. In contrast, patients with discordant findings, such as positive utDNA despite a clinical response, may be better candidates for radiation, while those without a clinical complete response may require definitive local therapy with radiation or radical cystectomy. Patients with detectable ctDNA would likely require systemic treatment, highlighting a future paradigm in which biomarker-informed stratification guides personalized management of MIBC.

Dr. Zlotta concluded with several key takeaways:
- Is this the end of TMT and radical cystectomy? Not yet.
- Bladder preservation is feasible but remains challenging.
- Up to 57% of patients may achieve pT0 (pCR) after neoadjuvant therapy, but current methods cannot reliably identify who can safely avoid cystectomy or consolidation therapy.
- Prediction of pT0 (pCR) remains imperfect.
- Even the best available tools (ctDNA, MRI, genomic markers) have limited sensitivity (~46–59%), meaning that up to 1 in 4 patients with an apparent CR may still harbor residual muscle-invasive disease.
- Whenever possible, patients should be enrolled in clinical trials.
- Nevertheless, the field is clearly moving toward an era in which more patients may be able to safely preserve their bladder.
Presented by: Alexandre R. Zlotta, MD, PhD, FRCSC, Director, Uro-Oncology, Division of Surgical Oncology, Princess Margaret Cancer Centre, University Health Network, Mount Sinai Hospital; Professor and Howard Sokolowski Chair in Uro-Oncological Research, Department of Surgery (Urology), University of Toronto
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, Vu TQ, Antonuzzo L, Wiechno P, Atduev V, Kann AG, Kim TH, Suárez C, Chang CH, Roghmann F, Özgüroğlu M, Eigl BJ, Oliveira N, Buchler T, Gadot M, Zakharia Y, Armstrong J, Gupta A, Hois S, van der Heijden MS; NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):1773-1786. doi: 10.1056/NEJMoa2408154. Epub 2024 Sep 15. PMID: 39282910.
- Vulsteke C, Adra N, Danchaivijitr P, Sabadash M, Rodriguez-Vida A, Zhang Z, Atduev V, Göger YE, Rausch S, Kang SH, Loriot Y, Bedke J, Galsky MD, O'Donnell PH, von Amsberg G, Alimohamed N, Sulimka G, Gupta S, Paramonov V, Nakane K, Mihm M, Meng C, Huang CD, Ramamurthy C, Homet Moreno B, Ullén A; KEYNOTE-905/EV-303 Investigators. Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer. N Engl J Med. 2026 Feb 18. doi: 10.1056/NEJMoa2511674. Epub ahead of print. PMID: 41707170.
- Galsky MD, Izadmehr S, Yu M, Curtis SD, Douville C, Popoli M, Ptak J, Dobbyn L, Silliman N, Chan KG, Dorff TB, Cetnar JP, O'Neil B, D'Souza A, Mamtani R, Kyriakopoulos CE, Brody R, Sadimin E, Mehrazin R, Chowell D, Sfakianos J, Daneshmand S, Pal SK, Bettegowda C, Kinzler KW, Papadopoulos N, Vogelstein B, Wang Y. Monitoring of plasma and urine tumor-derived DNA to inform bladder-sparing approaches for patients with muscle-invasive bladder cancer. Proc Natl Acad Sci U S A. 2026 Feb 24;123(8):e2533449123. doi: 10.1073/pnas.2533449123. Epub 2026 Feb 18. PMID: 41706890; PMCID: PMC12933130.