(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., was host to the Urothelial Cancer: Towards Integrated Therapeutic Strategies plenary session. Dr. Yohann Loriot, in the case-based panel discussion of High-risk NMIBC post-BCG Failure: Spare the Bladder?, discussed bladder sparing: trial overview, intravesical gene therapy (combinations).
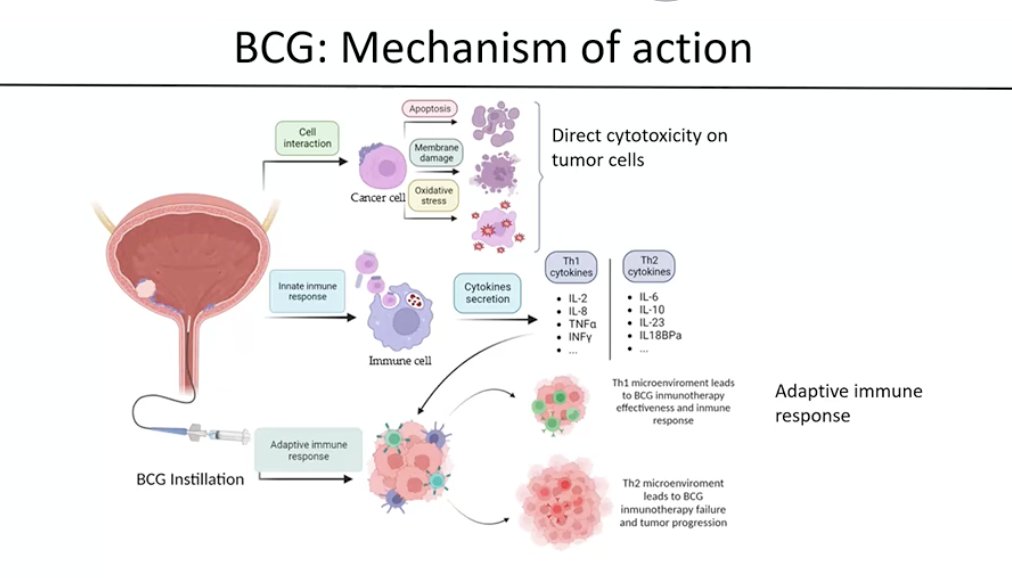
Dr. Loriot began by highlighting that intravesical immunotherapy and intravesical gene therapy combinations are an attractive strategy in patients with BCG-unresponsive, very high-risk NMIBC. He briefly reviewed the mechanism of action of BCG, noting that it induces both direct cytotoxic effects on tumor cells and a robust immune response within the bladder. BCG activates the innate immune system, leading to cytokine release and recruitment of immune cells, which subsequently promotes an adaptive immune response. A Th1-predominant immune microenvironment is associated with effective BCG activity, whereas a Th2-dominant response has been linked to treatment failure and tumor progression, as illustrated below.
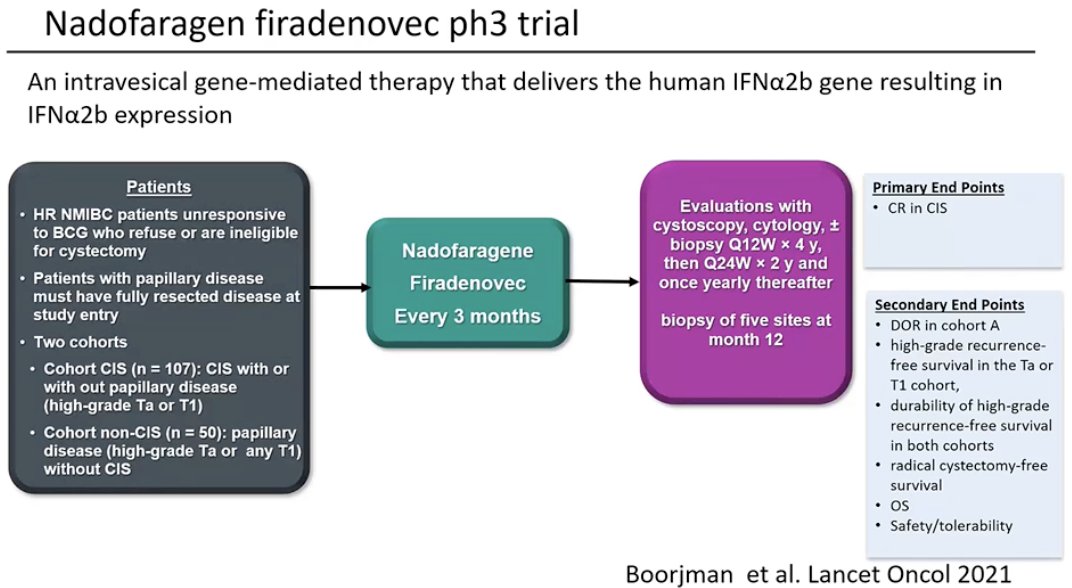
He highlighted that several important trials have shaped the treatment landscape in this setting. The first was the phase 3 trial evaluating nadofaragene firadenovec, an intravesical gene therapy that delivers the human IFNα2b gene, leading to local expression of interferon within the bladder.1 This study enrolled patients with high-risk NMIBC who were unresponsive to BCG and either refused or were ineligible for radical cystectomy, including a cohort with CIS ± papillary disease and another with papillary disease alone. Treatment was administered intravesically every three months, with the primary endpoint being complete response in the CIS cohort.
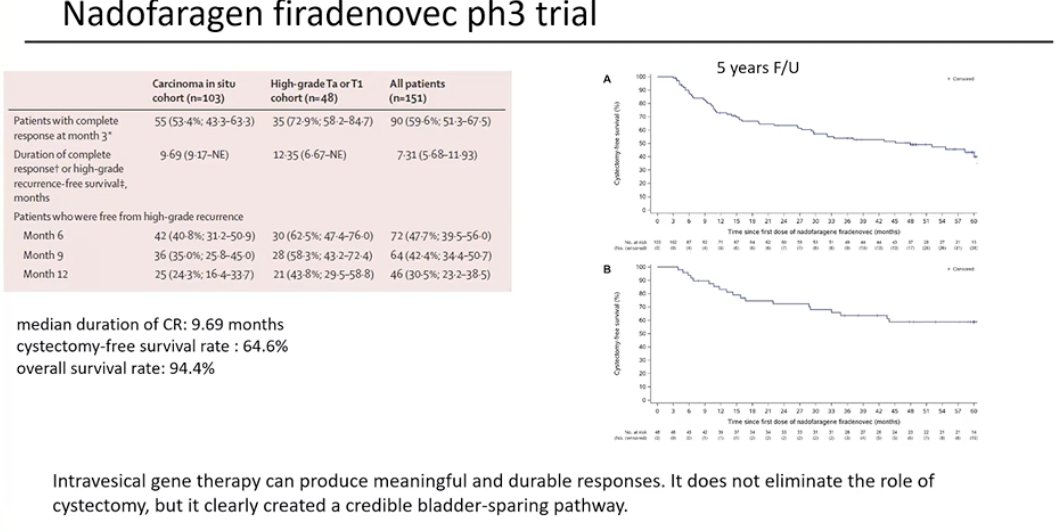
Results from this phase 3 study, published several years ago with extended follow-up (5-years), demonstrated durable responses with intravesical nadofaragene firadenovec. Among patients with CIS, the complete response rate at 3 months was approximately 55%, with a median duration of response of 9.7 months. Importantly, long-term follow-up showed durable bladder preservation, with a cystectomy-free survival rate of 64.6% and an overall survival of 94.4%. These results suggest that intravesical gene therapy can achieve meaningful and durable responses, offering a credible bladder-sparing option for selected patients, although it does not eliminate the role of radical cystectomy.1
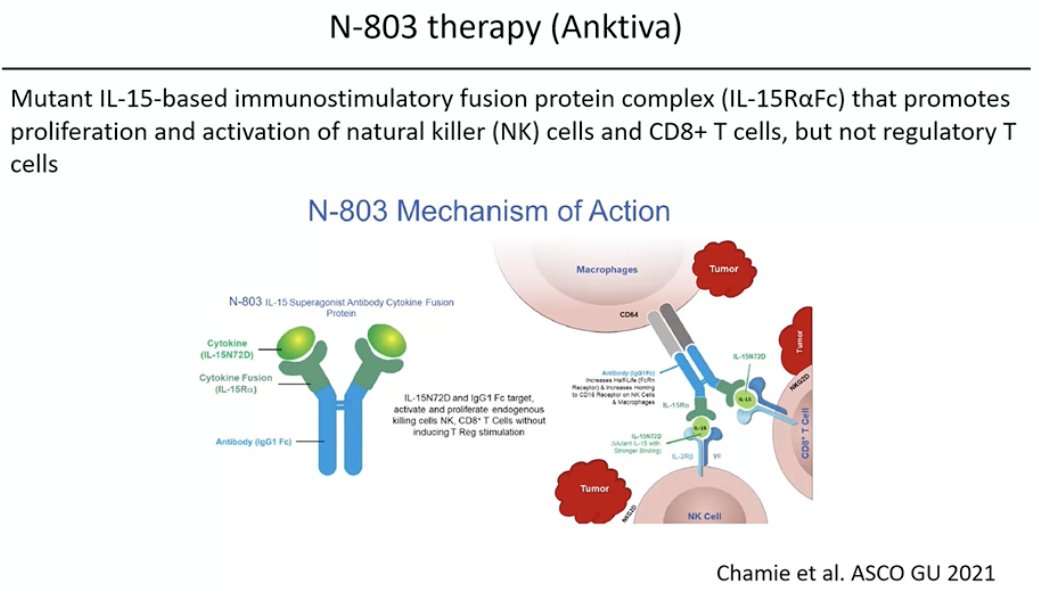
He then moved on to discuss N-803 (Anktiva), an IL-15–based immunostimulatory fusion protein designed to enhance the activation and proliferation of natural killer (NK) cells and CD8+ T cells without stimulating regulatory T cells. By amplifying the antitumor immune response within the bladder, this agent aims to strengthen immune-mediated tumor control and has been evaluated in combination with intravesical BCG in patients with BCG-unresponsive NMIBC.
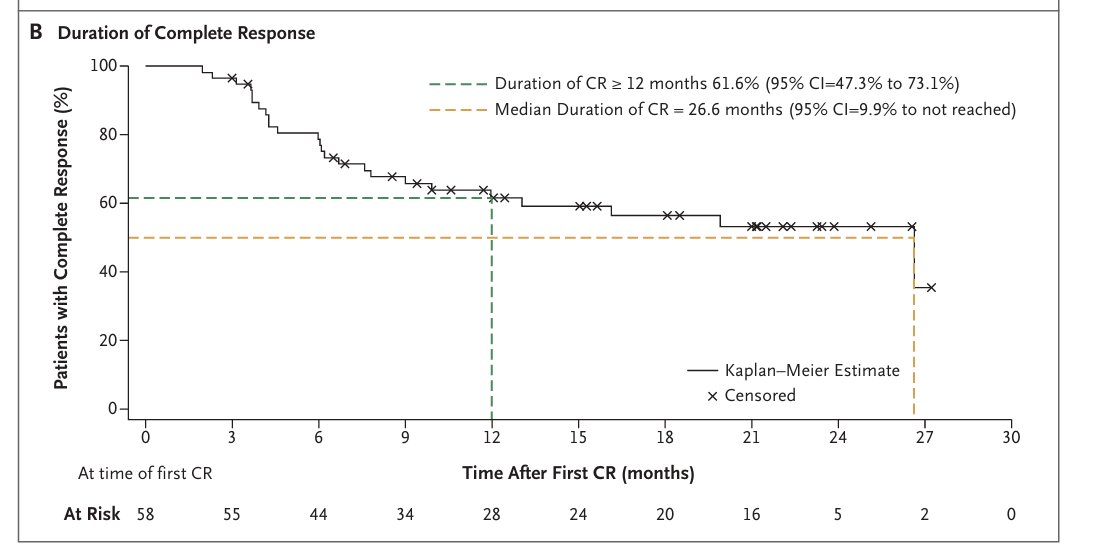
He then reviewed clinical results of N-803 in combination with BCG from the QUILT-3.032 study in patients with BCG-unresponsive NMIBC with CIS. In this cohort, 80 patients were enrolled, and 51 of 72 evaluable patients achieved a complete response at any time, corresponding to a CR rate of 71% (As illustrated in the curves below). Importantly, many of these responses were durable, with more than half of patients maintaining a response beyond 12 months, and 87.5% of patients had not progressed to radical cystectomy.2
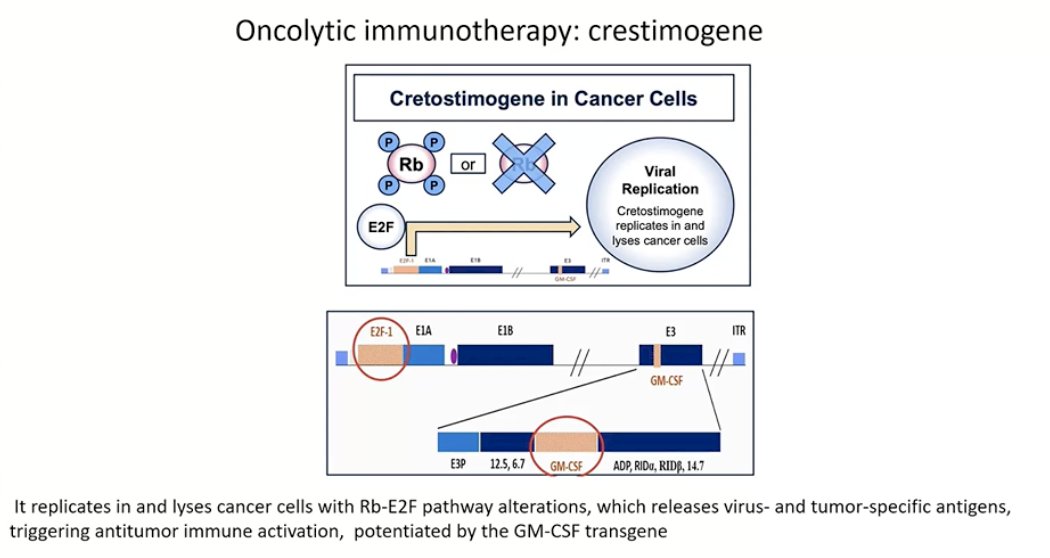
Lastly, he discussed cretostimogene, an adenovirus-based oncolytic immunotherapy. This agent selectively replicates in cancer cells with alterations in the Rb–E2F pathway, leading to tumor cell lysis and release of tumor-specific antigens. This process helps stimulate an antitumor immune response within the bladder, which is further enhanced by the GM-CSF transgene incorporated into the viral construct.
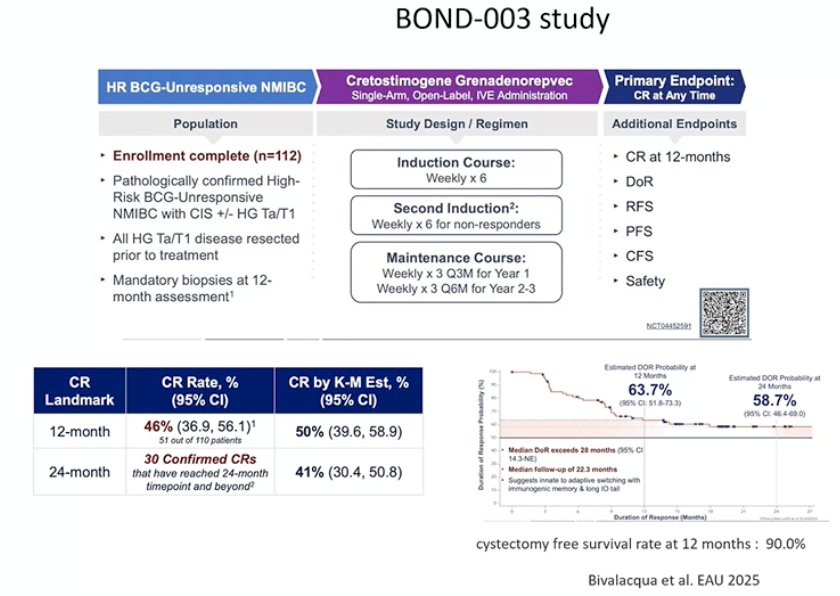
He also highlighted results from the BOND-003 study (design schema shown below) evaluating cretostimogene in patients with high-risk BCG-unresponsive NMIBC. In this single-arm study of 112 patients, the CR rate was 46% at 12 months and approximately 41% at 24 months by Kaplan–Meier estimate. Importantly, bladder preservation outcomes were notable, with a cystectomy-free survival rate of 90% at one year
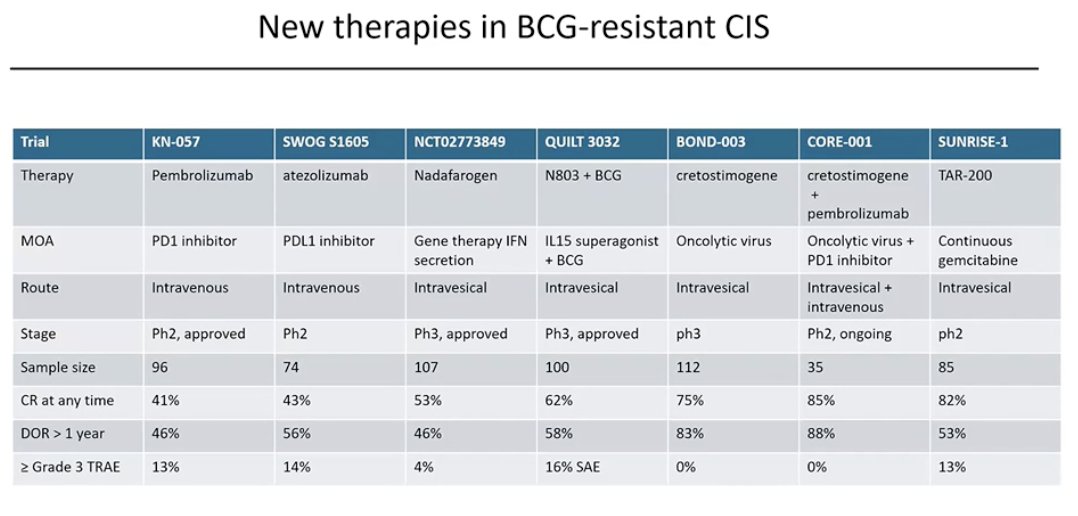
Notably, complete response rates at any time appear relatively high with several of these newer therapies in BCG-resistant CIS. As outlined in the table, multiple approaches, including systemic immunotherapy, gene therapy, IL-15–based immunotherapy combined with BCG, oncolytic viral therapy, and sustained intravesical chemotherapy, have demonstrated encouraging response rates across studies, highlighting the rapidly evolving treatment landscape for patients with BCG-unresponsive NMIBC.
He also highlighted that similar advances are being seen with new therapies for BCG-resistant papillary tumors. However, interpreting results across studies remains challenging, as key endpoints such as DFS, EFS, and RFS are defined differently across trials.

Presented by: Yohann Loriot, MD, PhD, Medical Oncology Department, Gustave Roussy, Université Paris-Saclay, Paris, France.
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:- Boorjian SA, Alemozaffar M, Konety BR, Shore ND, Gomella LG, Kamat AM, Bivalacqua TJ, Montgomery JS, Lerner SP, Busby JE, Poch M, Crispen PL, Steinberg GD, Schuckman AK, Downs TM, Svatek RS, Mashni J Jr, Lane BR, Guzzo TJ, Bratslavsky G, Karsh LI, Woods ME, Brown G, Canter D, Luchey A, Lotan Y, Krupski T, Inman BA, Williams MB, Cookson MS, Keegan KA, Andriole GL Jr, Sankin AI, Boyd A, O'Donnell MA, Sawutz D, Philipson R, Coll R, Narayan VM, Treasure FP, Yla-Herttuala S, Parker NR, Dinney CPN. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: a single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021 Jan;22(1):107-117. doi: 10.1016/S1470-2045(20)30540-4. Epub 2020 Nov 27. PMID: 33253641; PMCID: PMC7988888.
- Chamie K, Chang SS, Kramolowsky E, Gonzalgo ML, Agarwal PK, Bassett JC, Bjurlin M, Cher ML, Clark W, Cowan BE, David R, Goldfischer E, Guru K, Jalkut MW, Kaffenberger SD, Kaminetsky J, Katz AE, Koo AS, Sexton WJ, Tikhonenkov SN, Trabulsi EJ, Trainer AF, Spilman P, Huang M, Bhar P, Taha SA, Sender L, Reddy S, Soon-Shiong P. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid. 2023 Jan;2(1):EVIDoa2200167. doi: 10.1056/EVIDoa2200167. Epub 2022 Nov 10. PMID: 38320011.