(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., between March 13th and 16th 2026, was host to the Urothelial Cancer: Towards Integrated Therapeutic Strategies plenary session. Dr. Michiel Simon Van Der Heijden, in the Case-based panel discussion of High-risk Non-muscle Invasive Bladder Cancer (NMIBC) Post-BCG Failure: Spare the Bladder?, discussed why cystectomy is still relevant.
Dr. van der Heijden began by posing two key questions: whether radical cystectomy remains the best treatment for patients who fail BCG, and whether the timing of cystectomy influences outcomes.
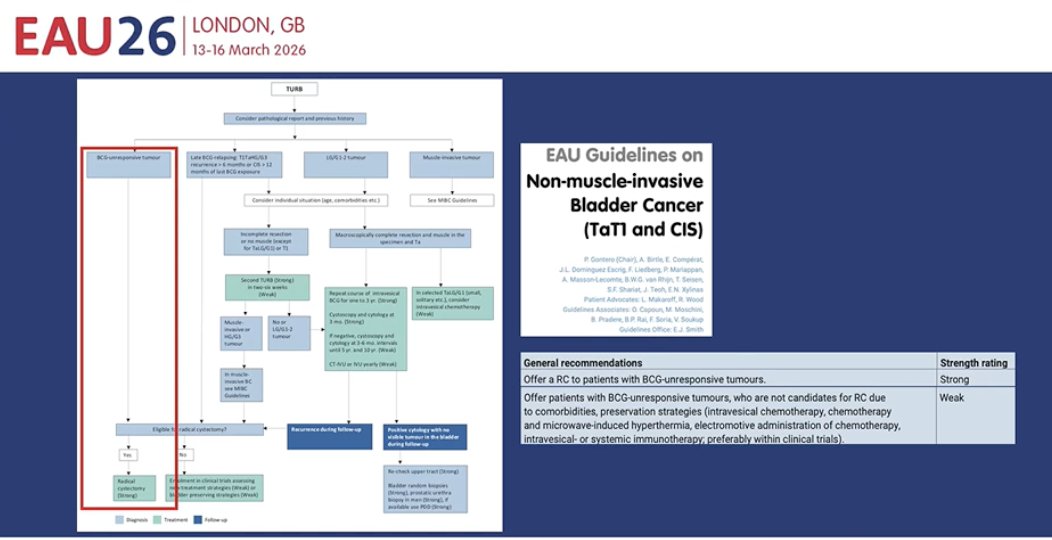
He noted that according to the EAU guidelines, patients with BCG-unresponsive tumors should be offered radical cystectomy as the recommended treatment with strong evidence. Other bladder-preserving strategies, including intravesical chemotherapy, device-assisted therapy, or systemic or intravesical immunotherapy, may be considered for selected patients, but these approaches carry only a weak recommendation in the current guidelines.
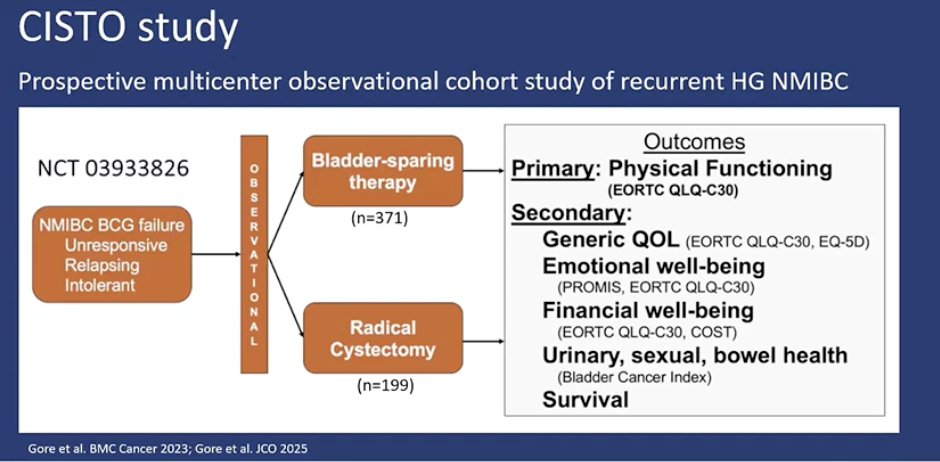
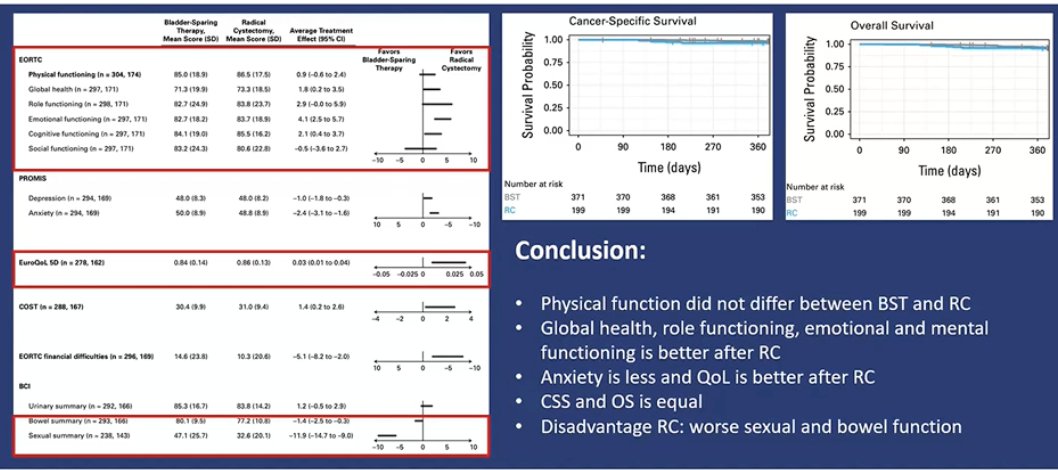
He noted that these recommendations are largely based on oncologic outcomes; however, the CISTO study evaluated this question from the patient’s perspective. CISTO was a prospective, multicenter observational cohort study that enrolled patients with recurrent high-grade NMIBC after BCG failure, including those who were BCG-unresponsive, relapsing, or intolerant. Patients underwent either bladder-sparing therapy or radical cystectomy according to real-world clinical decision-making. The primary endpoint was physical functioning measured by the EORTC QLQ-C30, while secondary endpoints included overall quality of life, emotional well-being, financial toxicity, urinary, sexual, and bowel health, as well as survival outcomes.1 The study design is highlighted below.

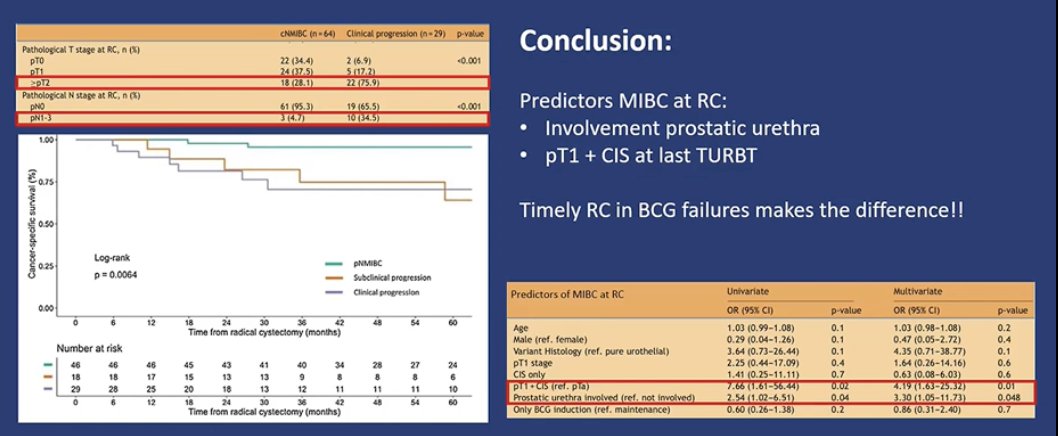
He concluded by discussing predictors of muscle-invasive disease at the time of radical cystectomy. In this analysis (figures below), involvement of the prostatic urethra and the presence of pT1 disease with concomitant CIS at the last TURBT were identified as important predictors of upstaging to MIBC at cystectomy. Referring back to the case presented earlier, he noted that the patient’s prostatic urethral involvement represents a high-risk feature and an ideal scenario where progression to muscle-invasive disease can occur. Overall, he emphasized that timely radical cystectomy in patients with BCG failure can make a significant difference, reinforcing that timing matters.
Presented by: Michiel Simon Van Der Heijden, MD, PhD, Medical Oncologist, Trial Group Leader, Department of Medical Oncology, Netherlands Cancer Institute, Amsterdam, Netherlands
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Nathan KK, Follmer KM, Nash MG, Wolff EM, Lee JR, Mecham S, Yano M, Kim SM, Comstock BA, Gore JL, Smith AB. The Comparison of Intravesical Therapy and Surgery as Treatment Options for Bladder Cancer (CISTO) study: Lessons learned about management and patient enrollment in a large, pragmatic, patient-centered trial. Cancer. 2025 Jan 1;131(1):e35600. doi: 10.1002/cncr.35600. Epub 2024 Oct 14. PMID: 39400910.
- Farré A, Huguet J, Basile G, Diéguez L, Izquierdo P, Sánchez R, Gavrilov P, Gallioli A, Rodríguez Faba O, Gaya JM, Palou J, Breda A. Oncological outcomes for patients with European Association of Urology definitions of BCG failure treated with radical cystectomy. Actas Urol Esp (Engl Ed). 2025 Nov;49(9):501834. English, Spanish. doi: 10.1016/j.acuroe.2025.501834. Epub 2025 Sep 12. PMID: 40947056.