(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., between March 13th and 16th 2026, was host to the Urothelial Cancer: Towards Integrated Therapeutic Strategies plenary session. Dr. Jeremy Teoh presented the state-of-the-art lecture, Bladder-sparing in MIBC: The Real-world Evidence.
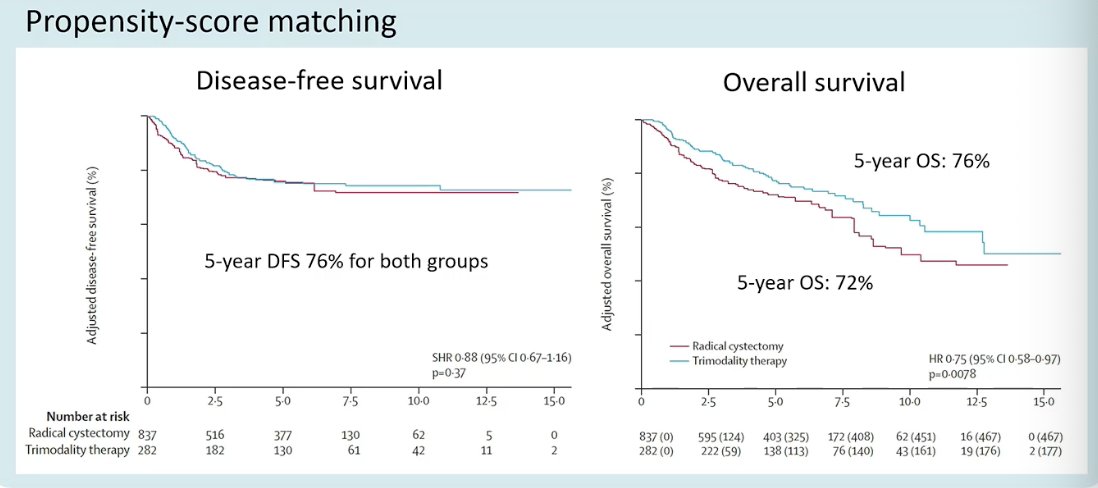
Dr. Teoh began by highlighting what he described as a key study that should be discussed in any conversation about bladder-sparing strategies for MIBC: the propensity score–matched analysis by Zlotta and colleagues comparing radical cystectomy and trimodality therapy. This retrospective study included 1,119 patients with cT2–T4N0M0 disease treated between 2005 and 2017. Using a 3:1 propensity score matching strategy and inverse probability of treatment weighting, the investigators compared oncologic outcomes between radical cystectomy and trimodality therapy. In the matched analysis, disease-free survival was nearly identical between groups, with a 5-year DFS of 76% for both strategies. Overall survival, however, favored trimodality therapy, with a 5-year OS of 76% compared with 72% for radical cystectomy (HR 0.75, 95% CI 0.58–0.97; p=0.0078).1
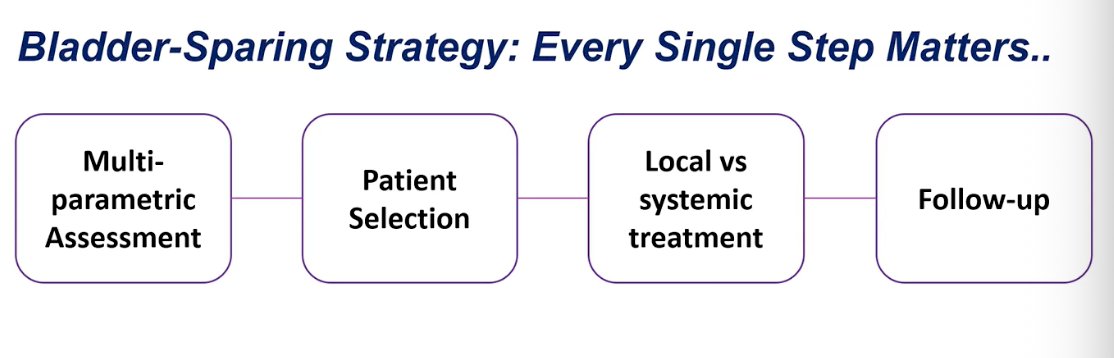
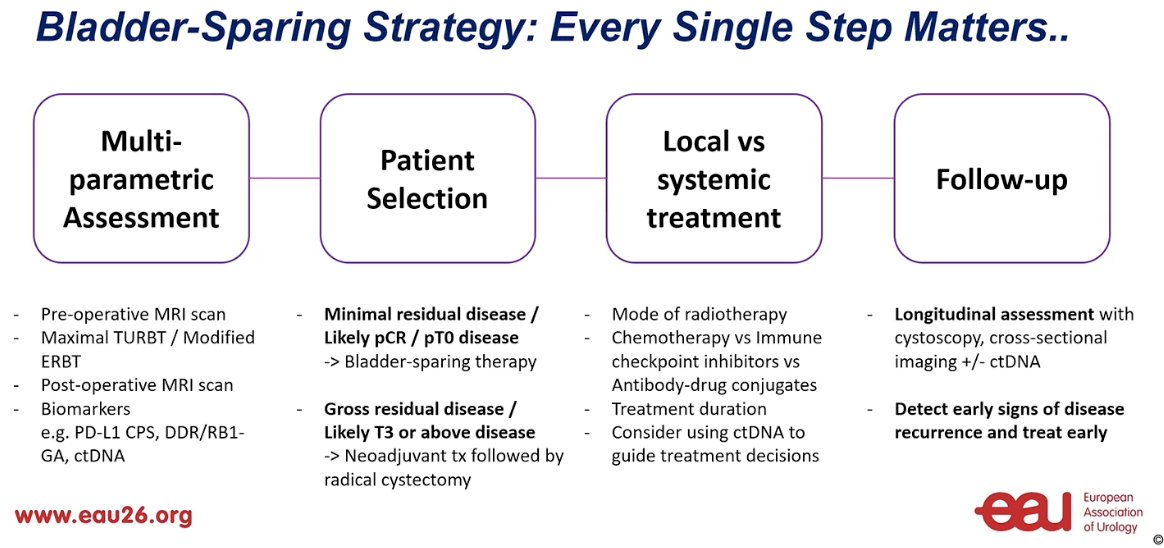
He emphasized that bladder preservation is not defined by a single intervention, but by a series of critical steps along the entire pathway. These include multiparametric assessment at diagnosis, careful patient selection, appropriate integration of local and systemic treatment, and structured follow-up. He then framed the discussion around what real-world data can teach us and how each of these components can be optimized to improve outcomes with bladder-sparing strategies.
Dr. Teoh then highlighted the importance of maximal TURBT as an early and critical step in the bladder preservation pathway. He referenced a large retrospective multi-institutional study that included 785 patients with MIBC who received neoadjuvant chemotherapy followed by radical cystectomy.2 In this cohort, 74% of patients underwent maximal TURBT prior to systemic therapy. Notably, maximal TURBT was associated with higher rates of pathologic downstaging at cystectomy, with 24% of patients achieving pT0 and an additional 25% having pTis/Ta/T1 disease, highlighting the potential oncologic impact of optimal local tumor resection before definitive treatment.
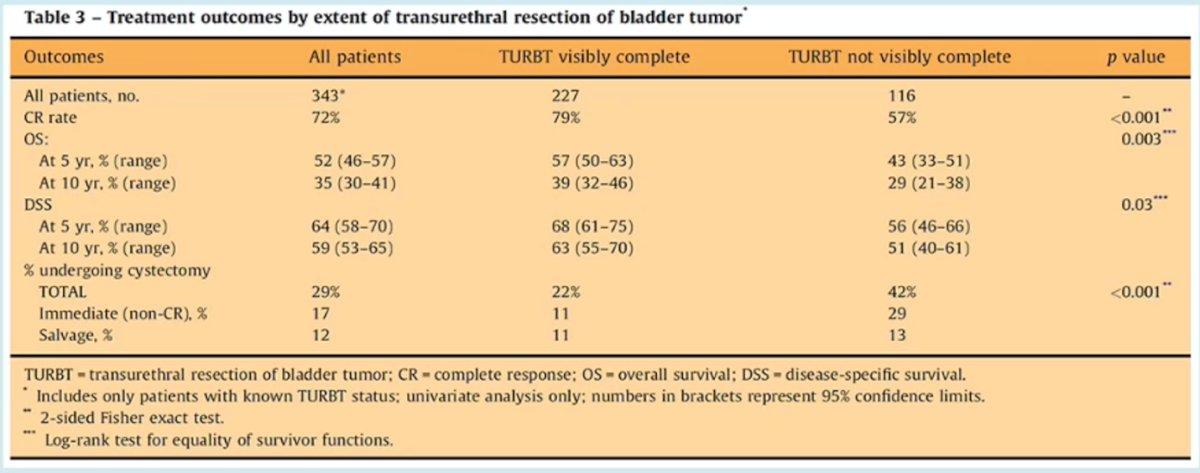
Similarly, he referenced the experience from the Massachusetts General Hospital group, which evaluated outcomes of selective bladder preservation using combined-modality therapy. In this cohort of 348 patients with cT2–T4aN0M0 MIBC treated with chemoradiation, a visibly complete TURBT was achieved in 65.2% of patients. Importantly, the extent of TURBT had a clear impact on oncologic outcomes: patients who underwent a visibly complete resection had significantly higher complete response rates and improved long-term outcomes, including both overall survival and disease-specific survival, compared with those with incomplete resections.3
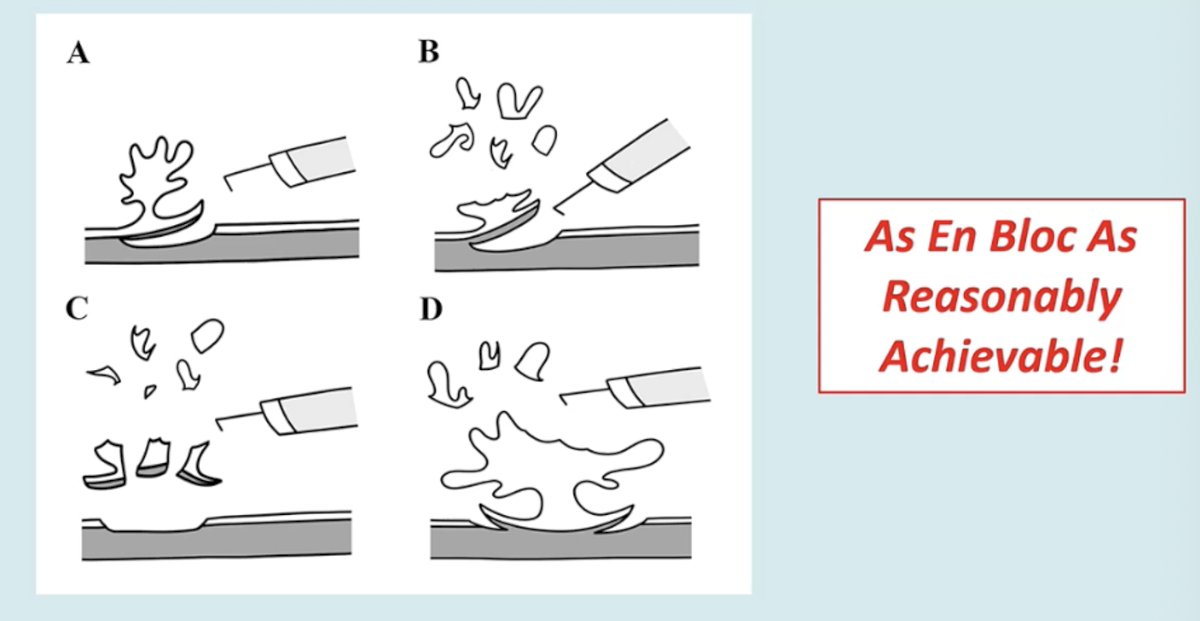
Dr. Teoh noted that achieving a maximal TURBT may also be facilitated through modified en bloc resection techniques. This approach aims to remove the tumor in a more controlled and intact fashion, minimizing tumor fragmentation while allowing a more complete and precise resection of the lesion and its underlying layers. As he emphasized, the goal is to perform the resection “as en bloc as reasonably achievable,” which may improve pathologic assessment and help optimize the quality of the initial local treatment in bladder-preserving strategies.4
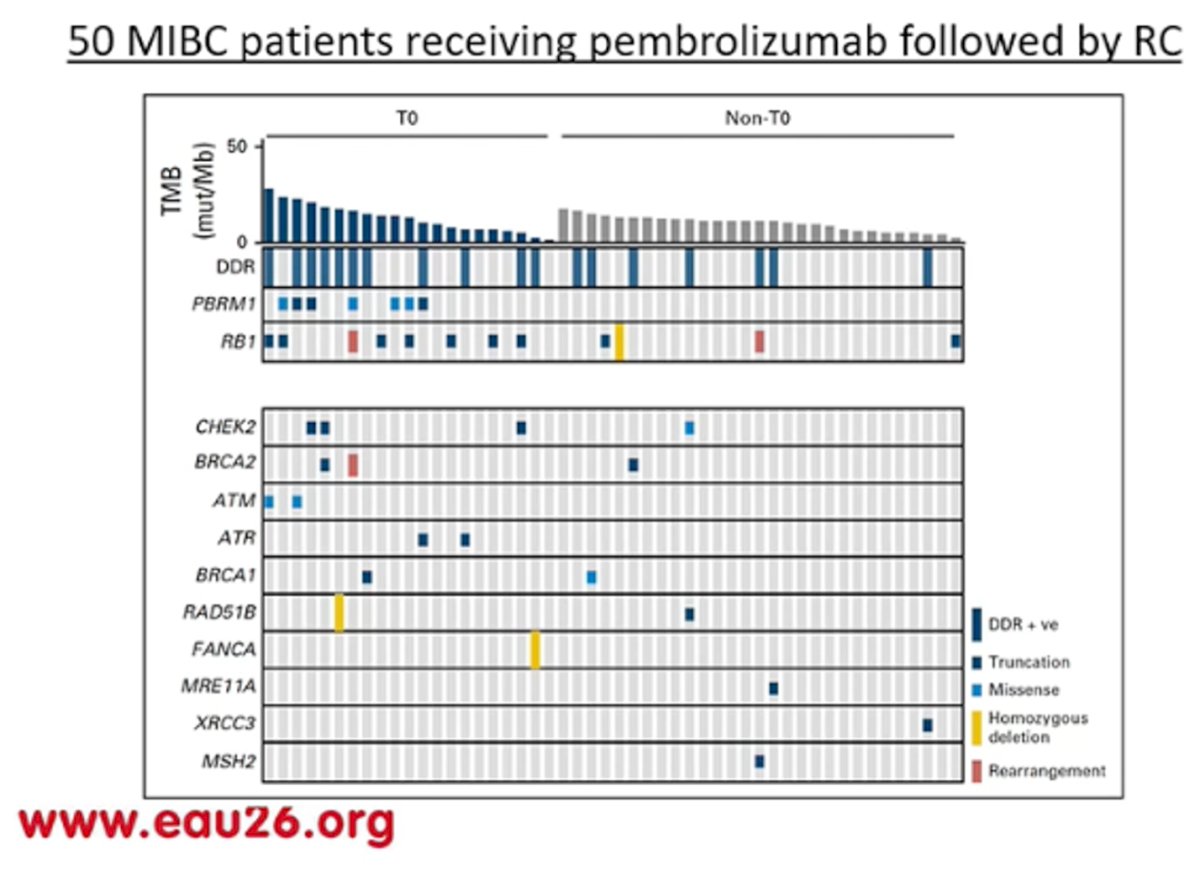
Dr. Teoh also highlighted the ongoing need to better identify predictive biomarkers that can help select patients most likely to respond to systemic therapy. He referenced the phase II PURE-01 study evaluating neoadjuvant pembrolizumab prior to radical cystectomy in 50 patients with MIBC. Although relatively small, this study provided important insights into potential molecular predictors of response, including tumor mutational burden and alterations in DNA damage response genes. These findings suggest that biomarker-driven patient selection may help refine bladder-preserving and systemic treatment strategies in the future, though further validation in larger cohorts is still needed.5
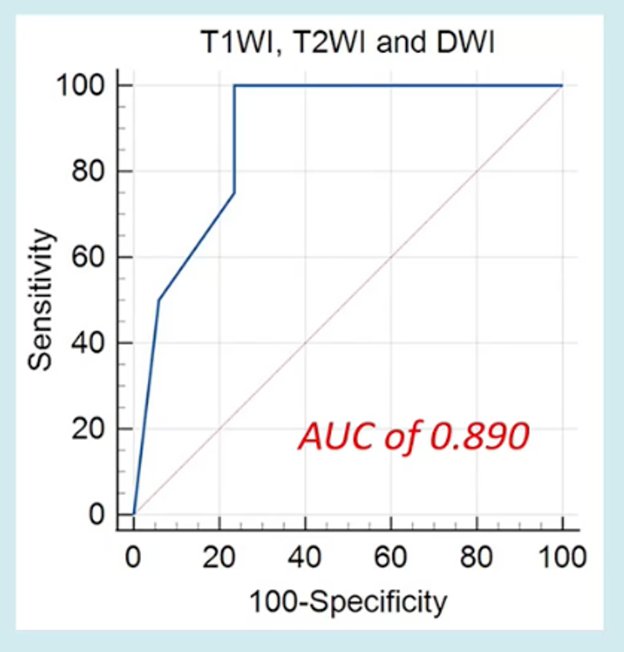
Dr. Teoh also discussed whether imaging could help refine patient selection for bladder-preserving approaches. He cited a study evaluating the role of MRI performed after TURBT to detect residual disease. In this retrospective analysis of 41 patients, post-TURBT multiparametric MRI demonstrated high sensitivity (100%) and a negative predictive value of 100% for detecting residual tumor, with an overall AUC of 0.89. Although specificity was lower (76.5%) and overestimation of residual disease occurred more frequently than underestimation, the absence of detectable disease on MRI following TURBT may represent a reassuring finding when considering a bladder-sparing strategy.
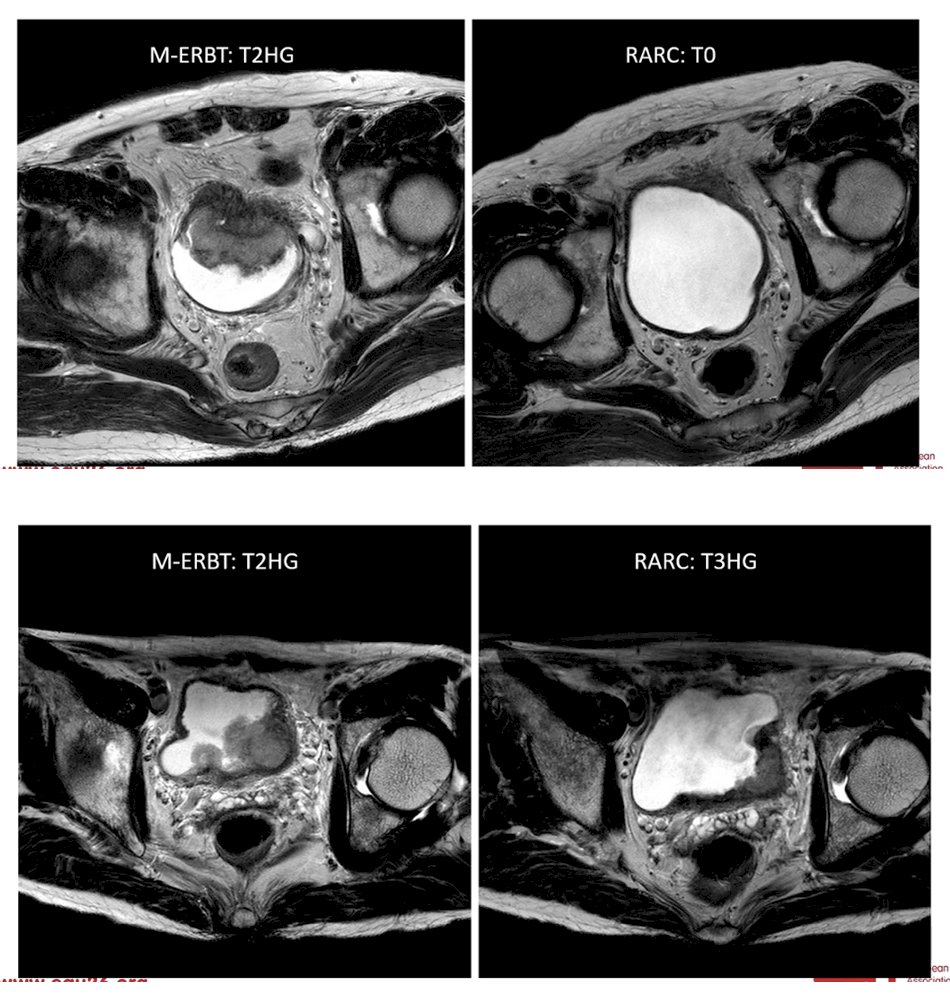
Dr. Teoh also presented illustrative clinical examples demonstrating how post-TURBT MRI may assist in staging and treatment planning. In one case, he performed an en bloc maximal TURBT, and subsequent MRI showed no evidence of residual disease; the patient later underwent robot-assisted radical cystectomy (RARC) and final pathology confirmed pT0 disease. In contrast, in another seemingly similar case, post-TURBT MRI demonstrated signs suggestive of extravesical extension, and surgical pathology ultimately confirmed pT3 disease. These examples highlight the potential role of MRI in improving post-resection staging and helping guide decisions between bladder-preserving strategies and definitive surgery.
Moreover, he briefly touched on the emerging role of antibody–drug conjugates (ADCs) with or without immune checkpoint inhibitors (ICI) in bladder-sparing strategies. Dr. Teoh cited two small real-world studies evaluating disitamab vedotin (DV) ± ICI in patients with MIBC. Notably, one of these studies included nine patients who received DV ± ICI, with five achieving a complete response (55.6%) and an overall response rate of 88.9%; only one patient ultimately proceeded to radical cystectomy after a median follow-up of 12 months.6 Although these cohorts remain small, these early data suggest that ADC-based combinations may represent a promising strategy to further expand bladder-preserving.
Finally, Dr. Teoh discussed the potential role of ctDNA dynamics in patients undergoing bladder-preserving TMT. He cited a study evaluating ctDNA patterns and recurrence after organ-sparing TMT in 84 patients with MIBC, the majority of whom had T2 and cN0 disease.7 Among the 46 patients with available pre- and post-TMT ctDNA assessments, 15 were ctDNA-positive prior to treatment, with 73% converting to ctDNA-negative after TMT. Conversely, among the 31 patients who were ctDNA-negative before treatment, 94% remained negative following therapy. Importantly, detectable ctDNA after TMT was strongly associated with metastatic recurrence, suggesting that ctDNA dynamics may provide valuable prognostic information and could potentially help guide surveillance or treatment intensification in bladder-preserving strategies in the future.
To conclude, Dr. Teoh emphasized that successful bladder preservation requires optimization at every step of the treatment pathway. Key takeaways included:
- Multiparametric assessment: pre-operative MRI, maximal TURBT/modified en bloc resection, post-TURBT MRI, and biomarkers (PD-L1 CPS, DDR/RB1 alterations, ctDNA)
- Patient selection: minimal residual disease or likely pCR/pT0 as candidates for bladder-sparing therapy
- Gross residual disease or likely ≥T3 disease: neoadjuvant treatment followed by radical cystectomy
- Treatment strategy: evolving systemic options including chemotherapy, immune checkpoint inhibitors, and antibody–drug conjugates; ctDNA may help guide decisions
- Follow-up: longitudinal assessment with cystoscopy, cross-sectional imaging ± ctDNA to detect recurrence early.
A summary slide of important steps for bladder-preservation is outlined below.
Presented by: Jeremy Teoh, MBBS, FRCSEd (Urol), FCSHK, FHKAM (Surgery), Associate Professor, The Chinese University of Hong Kong, Hong Kong
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Zlotta AR, Ballas LK, Niemierko A, Lajkosz K, Kuk C, Miranda G, Drumm M, Mari A, Thio E, Fleshner NE, Kulkarni GS, Jewett MAS, Bristow RG, Catton C, Berlin A, Sridhar SS, Schuckman A, Feldman AS, Wszolek M, Dahl DM, Lee RJ, Saylor PJ, Michaelson MD, Miyamoto DT, Zietman A, Shipley W, Chung P, Daneshmand S, Efstathiou JA. Radical cystectomy versus trimodality therapy for muscle-invasive bladder cancer: a multi-institutional propensity score matched and weighted analysis. Lancet Oncol. 2023 Jun;24(6):669-681. doi: 10.1016/S1470-2045(23)00170-5. Epub 2023 May 12. PMID: 37187202.
- Kirk PS, Lotan Y, Zargar H, Fairey AS, Dinney CP, Mir MC, Krabbe LM, Cookson MS, Jacobson NE, Montgomery JS, Vasdev N, Yu EY, Xylinas E, Kassouf W, Dall'Era MA, Sridhar SS, McGrath JS, Aning J, Shariat SF, Thorpe AC, Morgan TM, Holzbeierlein JM, Bivalacqua TJ, North S, Barocas DA, Grivas P, Garcia JA, Stephenson AJ, Shah JB, Daneshmand S, Spiess PE, van Rhijn BWG, Mertens L, Black P, Wright JL. Impact of Maximal Transurethral Resection on Pathological Outcomes at Cystectomy in a Large, Multi-institutional Cohort. J Urol. 2023 May;209(5):882-889. doi: 10.1097/JU.0000000000003193. Epub 2023 Feb 16. PMID: 36795962.
- Efstathiou JA, Spiegel DY, Shipley WU, Heney NM, Kaufman DS, Niemierko A, Coen JJ, Skowronski RY, Paly JJ, McGovern FJ, Zietman AL. Long-term outcomes of selective bladder preservation by combined-modality therapy for invasive bladder cancer: the MGH experience. Eur Urol. 2012 Apr;61(4):705-11. doi: 10.1016/j.eururo.2011.11.010. Epub 2011 Nov 12. PMID: 22101114.
- Teoh JY, Cheng CH, Tsang CF, Kai-Man Li J, Kwun-Chung Cheng B, Hoi-Chak Chan W, Kwun-Wai Chan W, Churk-Fai Li T, Chiu Y, Law MC, Lok-Hei Leung C, Sze-Ho Ho B, Yue-Kit Lee C, Cheong-Kin Chan R, Shu-Yin Chan E, Chan MT, Hok-Leung Tsu J, Tam HM, Lam KM, So HS, Cho CL, Ng CM, Chan CK, Liu PL, Wing-Hong Chu R, Tsui-Lin Ng A, Chu SK, Yee CH, Yiu MK, Lo KL, Au WH, Ma WK, Ka-Fung Chiu P, Sze-Wan Kwok H, Yip SY, Leung CH, Ng CF; EB-StaR Study Group. Transurethral En Bloc Resection Versus Standard Resection of Bladder Tumour: A Randomised, Multicentre, Phase 3 Trial. Eur Urol. 2024 Aug;86(2):103-111. doi: 10.1016/j.eururo.2024.04.015. Epub 2024 Apr 30. PMID: 38692956.
- Necchi A, Anichini A, Raggi D, Briganti A, Massa S, Lucianò R, Colecchia M, Giannatempo P, Mortarini R, Bianchi M, Farè E, Monopoli F, Colombo R, Gallina A, Salonia A, Messina A, Ali SM, Madison R, Ross JS, Chung JH, Salvioni R, Mariani L, Montorsi F. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J Clin Oncol. 2018 Dec 1;36(34):3353-3360. doi: 10.1200/JCO.18.01148. Epub 2018 Oct 20. PMID: 30343614.
- Wei Y, Zhang R, Yu C, Hong Z, Lin L, Li T, Chen J. Disitamab vedotin in combination with immune checkpoint inhibitors for locally and locally advanced bladder urothelial carcinoma: a two-center's real-world study. Front Pharmacol. 2023 Aug 14;14:1230395. doi: 10.3389/fphar.2023.1230395. PMID: 37645442; PMCID: PMC10461006.
- Epstein IB, Odogiyon A, Berg S, Otani Y, Mantia C, Pompa IR, Mossanen M, Wan J, Saraf A, Preston M, Ravi A, Carvalho F, Herberts C, ElNaggar A, Clinton T, Roberts D, Peng L, McGregor B, Bellmunt J, Kamran SC, Berchuck JE, Efstathiou JA, Miyamoto DT, Mouw KW. ctDNA dynamics and recurrence patterns after organ-sparing trimodality therapy for bladder cancer. Clin Cancer Res. 2026 Jan 26. doi: 10.1158/1078-0432.CCR-25-3712. Epub ahead of print. PMID: 41587110.