(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., was host to the Urothelial Cancer: Towards Integrated Therapeutic Strategies plenary session. Dr. James Catto, in the Case-based panel discussion of High-risk NMIBC post-BCG Failure: Spare the bladder?, discussed bladder sparing: trial overview and other intravesical options.
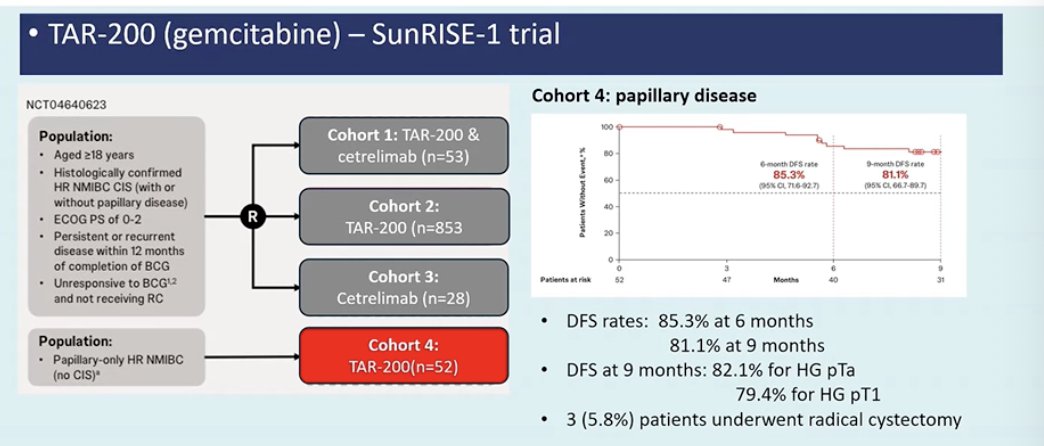
Dr. Catto noted that there are currently five potential intravesical options in this setting, although many are not yet widely available outside of clinical trials; however, several are already accessible in the United States. The first he reviewed was TAR-200, a sustained intravesical drug delivery system that continuously releases gemcitabine within the bladder. In the SunRISE-1 trial, TAR-200 demonstrated encouraging activity in patients with BCG-unresponsive disease, with a complete response rate of 82.4% in the cohort with CIS ± papillary disease and a median duration of response of approximately 25.8 months.1

Moreover, he also discussed the papillary cohort (cohort 4) from the SunRISE-1 study evaluating TAR-200. He highlighted the disease-free survival results observed in this group but noted that longer-term outcomes will be critical, particularly 1- and 3-year durable response rates. Overall, he described this as an exciting bladder-sparing option, with further data anticipated from the ongoing SunRISE-3 trial in BCG-naïve high-risk NMIBC and the SunRISE-5 trial in BCG-experienced disease.1
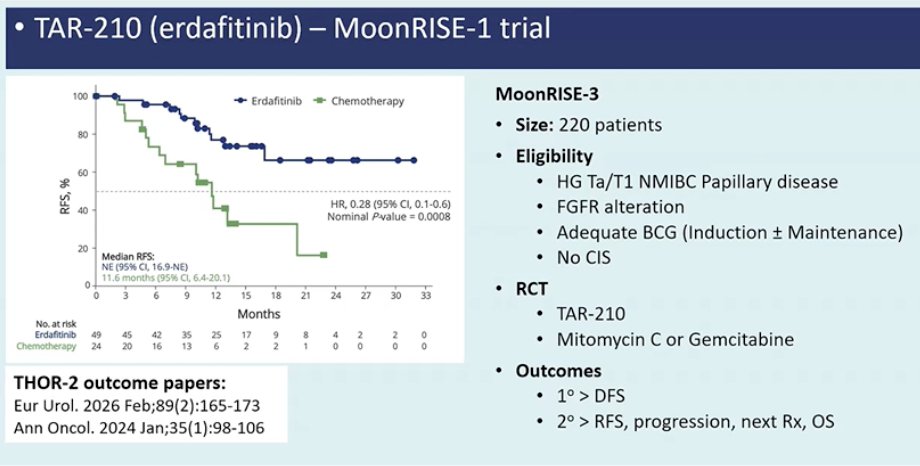
He next discussed TAR-210, which uses the same drug-delivery device as TAR-200 but is loaded with erdafitinib, targeting tumors with FGFR alterations. Early data from the MoonRISE-1 study suggest promising activity with this approach. He noted that the phase 3 MoonRISE-3 trial is currently recruiting patients with high-grade Ta/T1 papillary NMIBC harboring FGFR alterations after adequate BCG, comparing TAR-210 with intravesical chemotherapy. He emphasized that this strategy may become an exciting new option and could potentially change how and when we test for FGFR alterations in NMIBC.
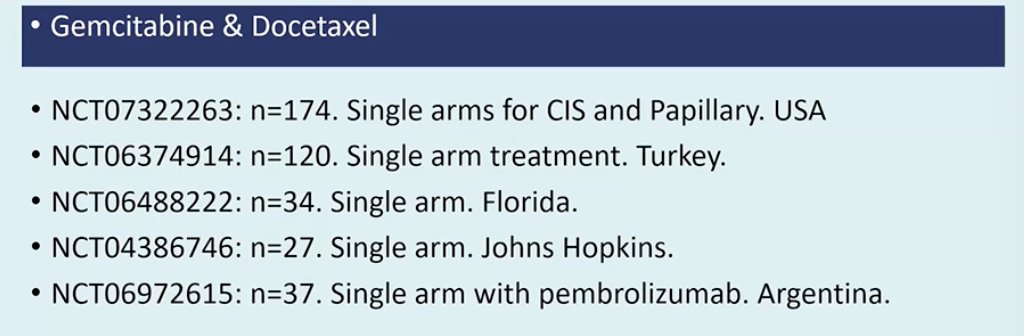
Dr. Catto also discussed intravesical gemcitabine plus docetaxel, noting that this is a regimen many centers could realistically afford, although it is still not widely used in some regions. Several single-arm studies evaluating this combination have been or are underway across different countries, including the United States, Turkey, Argentina, and other centers, showing encouraging activity in both CIS and papillary disease (figure below). In the UK, he noted that the COBRA trial is now being initiated to further evaluate this approach.
He also highlighted hyperthermic intravesical mitomycin C (HIVEC), evaluated in the HIVEC-HEAT study. This trial aims to enroll 238 patients with BCG-unresponsive NMIBC, including those with CIS ± papillary disease and those with high-grade papillary tumors without CIS. Treatment consists of a six-week induction course of mitomycin C with hyperthermia, followed by monthly maintenance for nine months. He noted that this is currently being evaluated in the UK in a nationwide effort, representing another bladder-sparing approach under active investigation.
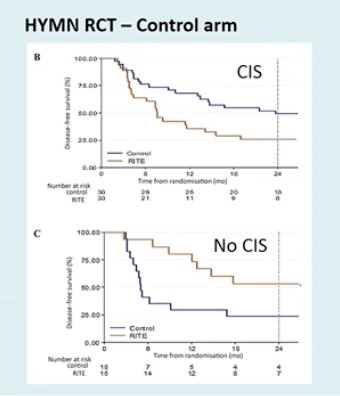
Finally, he noted that one option often overlooked is simply re-challenging with additional BCG. He presented data from the MD Anderson experience showing that a subset of patients can still achieve durable responses with further BCG therapy, with 75% remaining disease-free and a median duration of response of 83 months in selected cases. Similarly, in the control arm of the HYMN randomized trial, disease-free survival at 24 months was approximately 35–41%, suggesting that repeat BCG may still provide meaningful benefit for some patients.2
Presented by: James W.F. Catto, PhD, Professor, University of Sheffield, Sheffield, UK
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:- Daneshmand S, Van der Heijden MS, Jacob JM, Guerrero-Ramos F, Bögemann M, Simone G, Pieczonka CM, Casco NC, Zainfeld D, Spiegelhalder P, Xylinas E, Cahn D, Lotan Y, Murray KS, Kawahara T, Stromberg K, Martin J, Shukla A, Cutie CJ, Bertzos K, Hampras S, Sweiti H, Necchi A; SunRISe-1 Study. TAR-200 for Bacillus Calmette-Guérin-Unresponsive High-Risk Non-Muscle-Invasive Bladder Cancer: Results From the Phase IIb SunRISe-1 Study. J Clin Oncol. 2025 Nov 20;43(33):3578-3588. doi: 10.1200/JCO-25-01651. Epub 2025 Jul 30. Erratum in: J Clin Oncol. 2025 Oct 10;43(29):3231. doi: 10.1200/JCO-25-02053. PMID: 40737582; PMCID: PMC12622271.
- Tan WS, Panchal A, Buckley L, Devall AJ, Loubière LS, Pope AM, Feneley MR, Cresswell J, Issa R, Mostafid H, Madaan S, Bhatt R, McGrath J, Sangar V, Griffiths TRL, Page T, Hodgson D, Datta SN, Billingham LJ, Kelly JD. Radiofrequency-induced Thermo-chemotherapy Effect Versus a Second Course of Bacillus Calmette-Guérin or Institutional Standard in Patients with Recurrence of Non-muscle-invasive Bladder Cancer Following Induction or Maintenance Bacillus Calmette-Guérin Therapy (HYMN): A Phase III, Open-label, Randomised Controlled Trial. Eur Urol. 2019 Jan;75(1):63-71. doi: 10.1016/j.eururo.2018.09.005. Epub 2018 Sep 28. PMID: 30274699.