(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., was host to the Urothelial Cancer: Towards Integrated Therapeutic Strategies plenary Session. Dr. Roberto Contieri discussed Treatment De-intensification in NMIBC.
The rationale for deintensification in recurrent Ta low-grade NMIBC is based on several factors. These tumors generally have an excellent long-term prognosis, characterized by frequent recurrences but a very low risk of progression and negligible cancer-specific mortality. At the same time, NMIBC represents a costly disease, with expenses driven largely by repeated recurrences and potentially excessive surveillance in low-risk patients. Additionally, interventions such as TURBT are not without morbidity, particularly in an aging and often frail patient population, with risks including anesthesia-related complications and urinary tract infections. Importantly, urologists are often able to recognize low-grade recurrences with reasonable accuracy, estimated at around 85% even without urinary cytology, although the main concern remains the potential for missing high-grade disease.
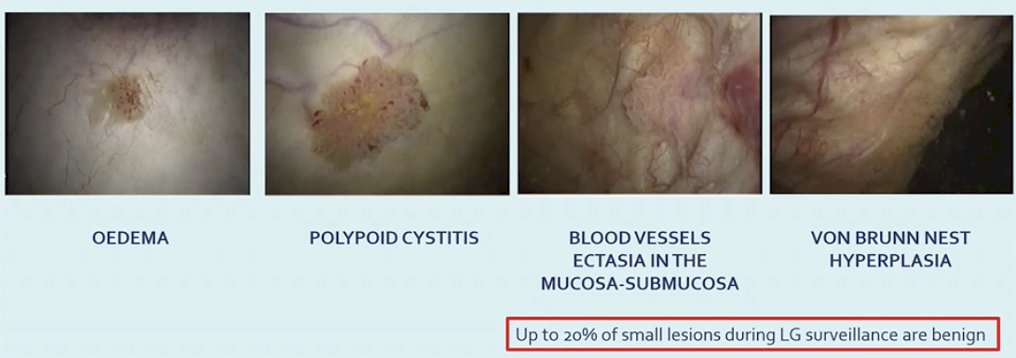
Dr. Contieri focused on the rationale for treatment deintensification, emphasizing that not all lesions observed during surveillance cystoscopy represent true tumor recurrence. Several benign conditions can mimic tumor growth in the bladder, including edema, polypoid cystitis, vascular ectasia of the mucosa and submucosa, and Von Brunn nest hyperplasia. Importantly, up to 20 percent of small lesions identified during surveillance of low-grade disease are ultimately benign, highlighting the potential risk of overtreatment in this setting.
The EAU guidelines support several deintensification strategies in appropriately selected patients. These include office fulguration or laser ablation of small recurrent lesions, active surveillance for carefully selected low grade tumors, and chemoablation approaches. These strategies aim to reduce treatment burden and avoid unnecessary procedures while maintaining oncologic safety in patients with low-risk disease.
There is also long-term evidence supporting office fulguration and laser ablation as established and oncologically safe deintensification strategies. Office fulguration has been used for many years, with data supporting both its safety and efficacy in appropriately selected patients. He also noted that patients tend to prefer outpatient laser ablation, with one study showing that 98 percent favored outpatient PDD guided photocoagulation over TURBT under general anesthesia. In addition, long term outcomes suggest that office-based management of selected Ta low grade recurrences can result in meaningful healthcare cost savings compared with repeat TURBT.1
Active surveillance has also been explored for several decades. Early work by Dr. Soloway and colleagues demonstrated that small, recurrent, low grade appearing bladder tumors tend to grow slowly and carry minimal risk.2 Based on these observations, surveillance was proposed as an alternative to immediate intervention, suggesting that in carefully selected patients, it may not be necessary to remove these lesions promptly at the time of recurrence, thereby reducing morbidity and costs associated with repeated transurethral resections.
He also highlighted the Bladder Cancer Italian Active Surveillance (BIAS) study, which evaluated outcomes of active surveillance in patients with low grade NMIBC. In this cohort, 251 active surveillance events were reported, with a median follow up of 38.8 months and a median time on surveillance of 13 months. Importantly, the probability of remaining treatment free at 12 months was approximately 60 percent, supporting the feasibility of active surveillance as a strategy to delay or avoid intervention in carefully selected patients.3

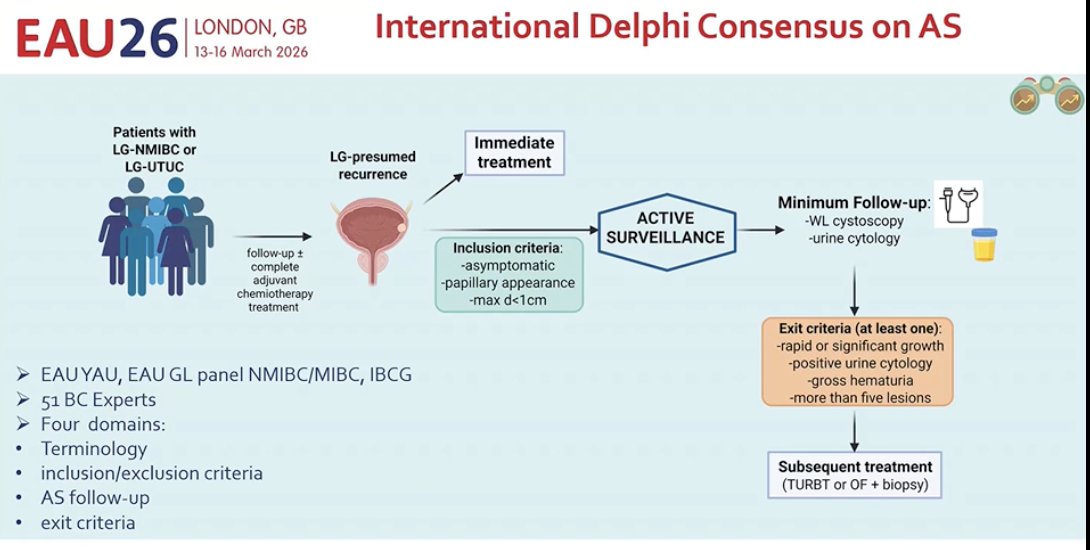
Dr. Contieri noted that an international Delphi consensus process has now been conducted to further define the role of active surveillance in this setting, with the manuscript currently in press. This effort brought together experts from the EAU Young Academic Urologists, the EAU NMIBC and MIBC guideline panels, and the International Bladder Cancer Group, involving 51 bladder cancer experts. The consensus addressed four key domains, including terminology, inclusion and exclusion criteria, active surveillance follow up, and exit criteria, helping to standardize the selection and monitoring of patients considered for this deintensified approach.
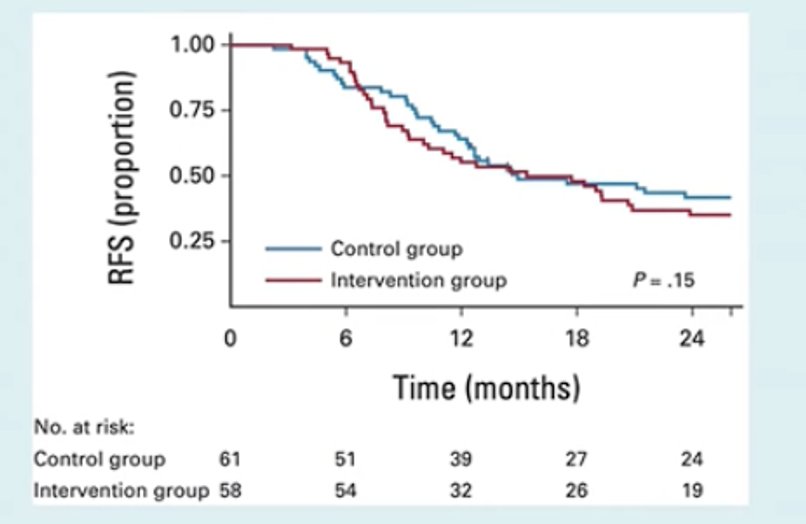
Another deintensification strategy discussed was chemoablation. Data from the DaBlaCa-13 study evaluated short term intensive chemo-ressection with intravesical mitomycin C in patients with recurrent Ta low or high grade NMIBC. In this trial, mitomycin C was administered three times per week for two weeks, with TURBT or office biopsy reserved for patients with an incomplete response. The complete response rate in the intervention group was 57 percent, with 12-month recurrence free survival rates of approximately 36 to 43 percent. However, it was noted that this approach still represents a relatively intensive treatment strategy for this patient population.4
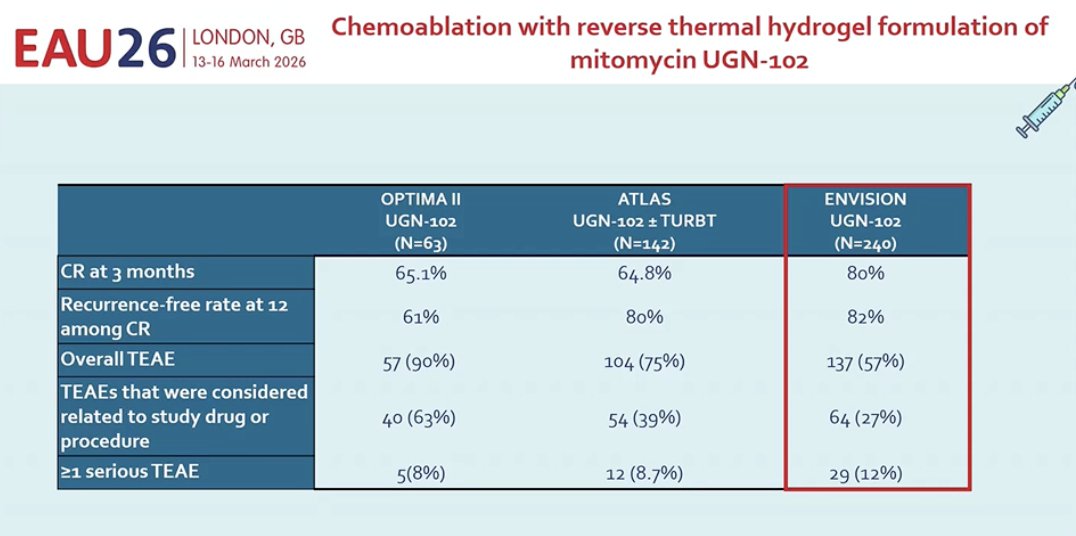
Moreover, he discussed newer chemoablation strategies using the reverse thermal hydrogel formulation of mitomycin C, UGN 102. This formulation allows prolonged exposure of the urothelium to mitomycin by transitioning from a liquid to a gel at body temperature, thereby enhancing local drug delivery. Data from recent studies including OPTIMA II, ATLAS, and ENVISION have demonstrated promising complete response rates at three months, reaching up to 80 percent in the ENVISION trial. UGN 102 received FDA approval last year and represents an emerging chemoablative option for selected patients with NMIBC.5
Lastly, he discussed emerging chemoablation approaches using new technologies such as TAR 210. This device is designed to provide sustained local release of erdafitinib within the bladder for several months while limiting systemic exposure. Early data from patients with intermediate risk NMIBC harboring FGFR alterations demonstrated encouraging activity, with 31 patients evaluable for response and a complete response rate of approximately 90 percent at week 12. These technologies may further shift the management of selected patients toward non-surgical treatment strategies.
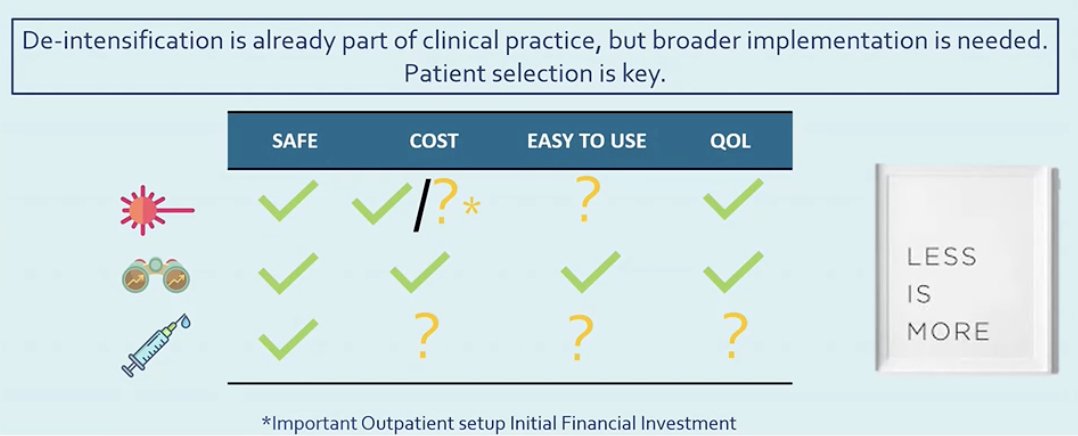
Dr. Contieri concluded his presentation emphasizing that treatment deintensification is already part of clinical practice, although broader implementation is still needed. He highlighted that careful patient selection remains critical when applying these strategies. Approaches such as office fulguration, active surveillance, and chemoablation may offer safe alternatives that reduce treatment burden, costs, and impact on quality of life in appropriately selected patients. Ultimately, these strategies reflect a growing recognition that in certain clinical scenarios, less intensive management may provide meaningful benefits for patients.
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:- Vitug C, Lajkosz K, Chavarriaga J, Llano A, Din S, Villegas E, Kuk C, Chan A, Gao B, Hemminki O, Kot D, Misurka J, van der Kwast TH, Wallis C, Jewett MAS, Soloway MS, Fleshner NE, Kulkarni GS, Zlotta AR. Long-term outcomes and cost savings of office fulguration of papillary Ta low-grade bladder cancer. BJU Int. 2024 Mar;133(3):289-296. doi: 10.1111/bju.16269. Epub 2024 Jan 5. PMID: 38105525.
- Soloway MS. Active Surveillance or Office Fulguration for Low Grade Ta Bladder Tumors: A Win-Win for Patients and Urologists. J Urol. 2018 May;199(5):1120-1122. doi: 10.1016/j.juro.2017.09.123. Epub 2017 Oct 5. PMID: 28987859.
- Contieri R, Paciotti M, Lughezzani G, Buffi NM, Frego N, Diana P, Fasulo V, Saita A, Casale P, Lazzeri M, Guazzoni G, Hurle R. Long-term Follow-up and Factors Associated with Active Surveillance Failure for Patients with Non-muscle-invasive Bladder Cancer: The Bladder Cancer Italian Active Surveillance (BIAS) Experience. Eur Urol Oncol. 2022 Apr;5(2):251-255. doi: 10.1016/j.euo.2021.05.002. Epub 2021 May 28. PMID: 34059485.
- Lindgren MS, Bue P, Azawi N, Blichert-Refsgaard L, Sundelin MO, Dyrskjøt L, Jensen JB. The DaBlaCa-13 Study: Short-term, Intensive Chemoresection Versus Standard Adjuvant Intravesical Instillations in Non-muscle-invasive Bladder Cancer-A Randomised Controlled Trial. Eur Urol. 2020 Dec;78(6):856-862. doi: 10.1016/j.eururo.2020.07.009. Epub 2020 Jul 28. PMID: 32736928.
- Prasad SM, Shishkov D, Mihaylov NV, Khuskivadze A, Genov P, Terzi V, Kates M, Huang WC, Louie MJ, Raju S, Burger B, Meads A, Schoenberg M. Primary Chemoablation of Recurrent Low-Grade Intermediate-Risk Nonmuscle-Invasive Bladder Cancer With UGN-102: A Single-Arm, Open-Label, Phase 3 Trial (ENVISION). J Urol. 2025 Feb;213(2):205-216. doi: 10.1097/JU.0000000000004296. Epub 2024 Oct 24. PMID: 39446087; PMCID: PMC12708048.