(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., was host to the Urothelial Cancer: Towards integrated therapeutic strategies: Plenary Session. Dr. Kathryn Gessner, in the case-based panel discussion of High-risk NMIBC Post-BCG Failure: Spare the Bladder?, discussed how cystectomy and bladder sparing compare when we ask patients.
Dr. Gessner began by noting that, as highlighted throughout the session, NMIBC carries a high risk of recurrence, with approximately 24–61% of patients recurring despite BCG therapy. While radical cystectomy remains the standard of care for appropriate patients, many individuals are reluctant to undergo this procedure. As a result, patients often weigh the risks and benefits between bladder-sparing therapy, accepting a potential risk of disease progression and loss of opportunity for cure, and radical cystectomy, which carries significant morbidity and potential impacts on quality of life. This balance raises an important question: do bladder-sparing approaches truly translate into better patient-reported outcomes compared with cystectomy?
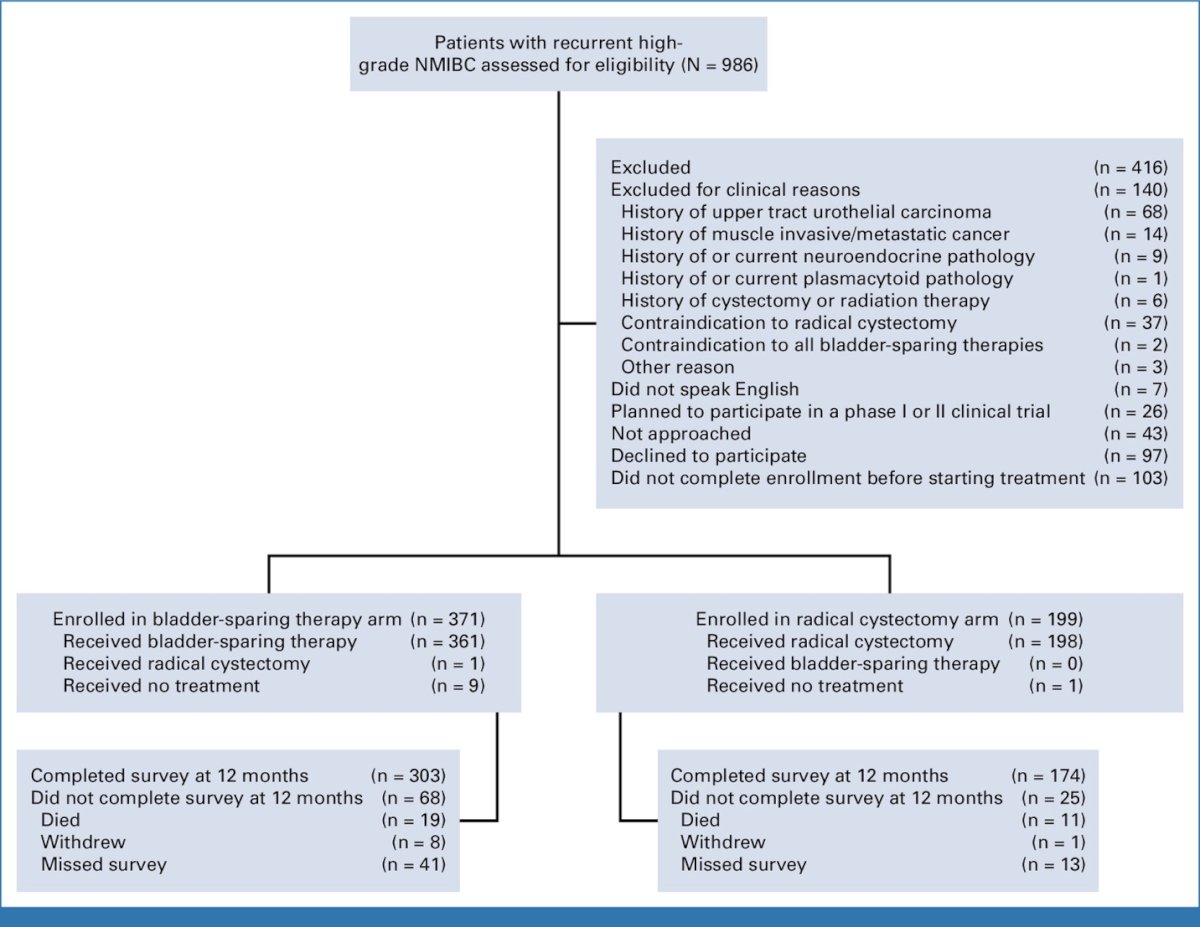
Dr. Gessner highlighted the CISTO study as the highest level of evidence currently available addressing this question. This was the first prospective clinical study directly comparing bladder-sparing therapy (BST) and radical cystectomy (RC) while focusing on patient-reported outcomes. The pragmatic, prospective observational cohort study was conducted across 36 academic and community sites in the United States, and notably, patients selected their own treatment approach. Eligible patients had recurrent high-grade NMIBC, had previously received at least induction BCG, and had undergone their last NMIBC treatment within the prior 12 months.
The primary endpoint was physical functioning at 12 months, measured using the EORTC QLQ-C30 scale. Secondary endpoints included other quality-of-life domains, depression and anxiety measures, bladder cancer–specific quality of life, financial burden, and oncologic outcomes. In total, 570 patients were enrolled, with the majority opting for bladder-sparing therapy (n=371) compared with radical cystectomy (n=199).1
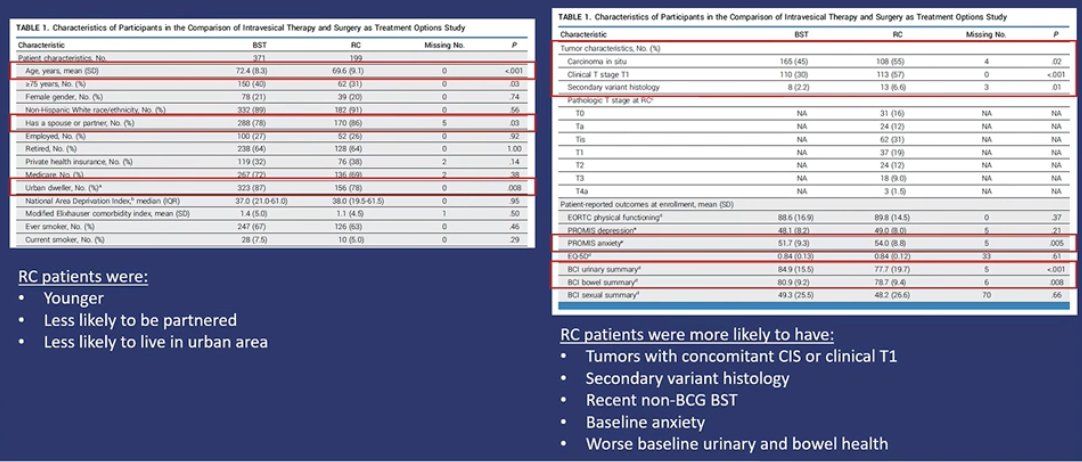
In the CISTO study, the treatment groups were generally well balanced, although some differences were noted. Patients who underwent radical cystectomy tended to be younger, less likely to have a partner, and less likely to live in urban areas. Clinically, RC patients were more likely to present with higher-risk features, including tumors with concomitant CIS or clinical T1 disease and secondary variant histology, and were more likely to have received recent non-BCG bladder-sparing therapy. At baseline, they also reported higher levels of anxiety and worse urinary and bowel function compared with patients who opted for bladder-sparing therapy.
Notably, the CISTO study showed no significant difference in physical functioning at 12 months between patients undergoing bladder-sparing therapy and those treated with radical cystectomy. However, radical cystectomy was associated with better emotional functioning, improved general health-related quality of life, and lower financial burden, with patients also reporting lower levels of depression and anxiety. In contrast, bladder-sparing therapy was associated with better bowel and sexual health outcomes.1
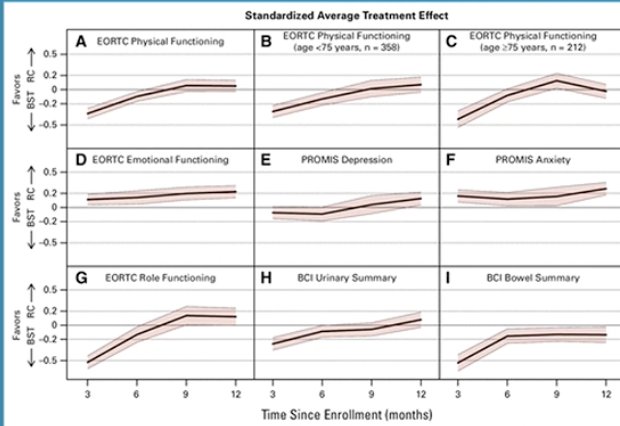
Time plots from the CISTO study demonstrated that patient-reported outcomes evolved over the first 12 months after treatment. While physical functioning remained similar between bladder-sparing therapy and radical cystectomy over time, several quality-of-life domains increasingly favored radical cystectomy, including emotional functioning, role functioning, depression, and anxiety. Urinary outcomes showed modest improvement over time in both groups, whereas bowel outcomes consistently favored bladder-sparing therapy. Overall, these longitudinal analyses supported the main study findings, highlighting comparable physical function but differences across specific quality-of-life domains depending on treatment strategy.
Notably, there was no difference in cancer-specific survival between treatment strategies, with rates of 99% for bladder-sparing therapy and 96% for radical cystectomy (WRR 0.99; 95% CI 0.97–1.01). Overall survival was also similar between groups. However, bladder-sparing therapy was associated with lower recurrence-free survival. In contrast, radical cystectomy carried a higher risk of adverse events and serious adverse events, with a reported 90-day mortality rate of 2.5%.1
In summary, outcomes were largely comparable between radical cystectomy and bladder-sparing therapy, with each strategy offering distinct advantages. Bladder-sparing therapy was associated with better bowel health, improved sexual quality of life, and fewer adverse events. Physical function at 12 months, cancer-specific survival, social functioning, and bladder-specific urinary quality of life were similar between groups. However, radical cystectomy was associated with better emotional functioning, lower depression and anxiety scores, improved financial well-being and global health, as well as lower recurrence rates at 12 months. Overall, these findings may help alleviate patient concerns about the impact of radical cystectomy on quality of life and highlight the importance of comprehensive patient counseling to support shared decision-making.

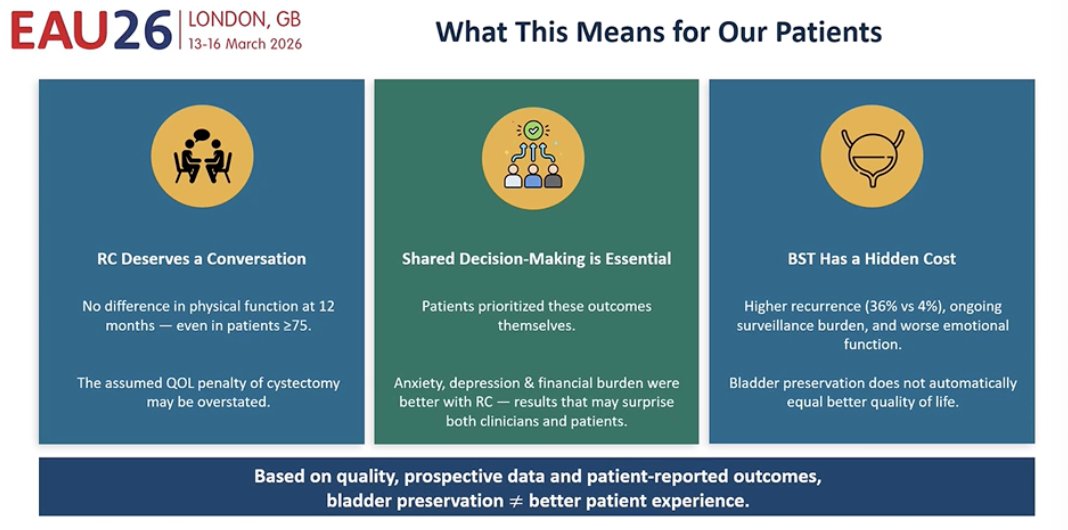
Dr. Gessner concluded by discussing what these findings mean for patients. Importantly, bladder-sparing therapy does not necessarily translate into a better patient experience. Physical functioning at 12 months was similar between strategies, even among older patients, suggesting that the commonly assumed quality-of-life penalty of radical cystectomy may be overstated. The results also emphasize the importance of shared decision-making, as patients themselves prioritized outcomes such as anxiety, depression, and financial burden, which were actually better among those undergoing radical cystectomy. At the same time, bladder-sparing therapy carries a hidden cost, including higher recurrence rates and the burden of ongoing surveillance, highlighting that bladder preservation does not automatically equate to better quality of life.
Presented by: Kathryn Hacker Gessner, MD, PhD, Urologic Oncologist at University of North Carolina School of Medicine, Chapel Hill, NC
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References: