(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., was host to the Urothelial Cancer: Towards Integrated Therapeutic Strategies: Plenary Session. Dr. Trinity Bivalacqua, in a case-based panel discussion, presented a bladder-sparing trial overview.
Dr. Yasmin Abu Ghanem then presented a clinical case of a 68-year-old male with a history of former tobacco use, hypertension, and type 2 diabetes who initially presented with recurrent painless visible hematuria over a three-month period. The patient had no prior history of bladder cancer and maintained an ECOG performance status of 0.
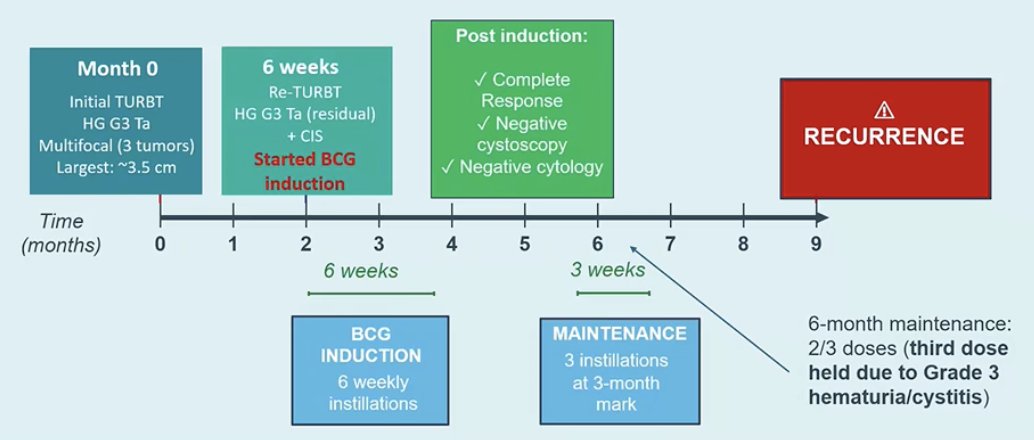
Initial TURBT revealed multifocal high grade G3 pTa disease with three tumors, the largest measuring approximately 3.5 cm. Cross sectional imaging with CT urography and chest imaging showed no evidence of metastatic disease. A repeat TURBT demonstrated residual high grade G3 pTa disease along with concomitant CIS. The patient subsequently initiated BCG induction therapy and expressed a strong preference for bladder preservation.
The patient subsequently received BCG induction followed by maintenance according to the SWOG protocol, for a total of 11 instillations, fulfilling the EAU criteria for adequate BCG exposure. Following induction therapy, he achieved a complete response with negative cystoscopy and negative cytology. Maintenance therapy was initiated with three instillations at the three-month mark, although the third dose during the six month maintenance cycle was held due to grade 3 hematuria and cystitis, and he developed a recurrence at the 9-month mark. The timeline of the patient’s treatment course is illustrated below.
Subsequent TURBT pathology revealed a papillary tumor classified as high grade T1 measuring 1.5 cm. Random bladder biopsies demonstrated CIS in multiple sites, including involvement of the prostatic urethra. Detrusor muscle was present in the specimen with no evidence of muscle invasive disease, and no variant histology was identified. Based on these findings, the patient met EAU criteria for very high risk NMIBC and was considered to have BCG unresponsive disease despite having received adequate BCG exposure
Dr. Bivalacqua began by noting that the presence of prostatic urethral involvement in this patient would exclude him from the major trials evaluating immune checkpoint inhibitors in combination with BCG. He then reviewed the evidence from three large randomized trials investigating the addition of immune checkpoint inhibition to BCG in BCG naïve high risk NMIBC, including the CREST, POTOMAC, and ALBAN studies, all of which evaluated combination strategies of ICI plus BCG in patients with high risk disease.1-3 The trials are summarized below.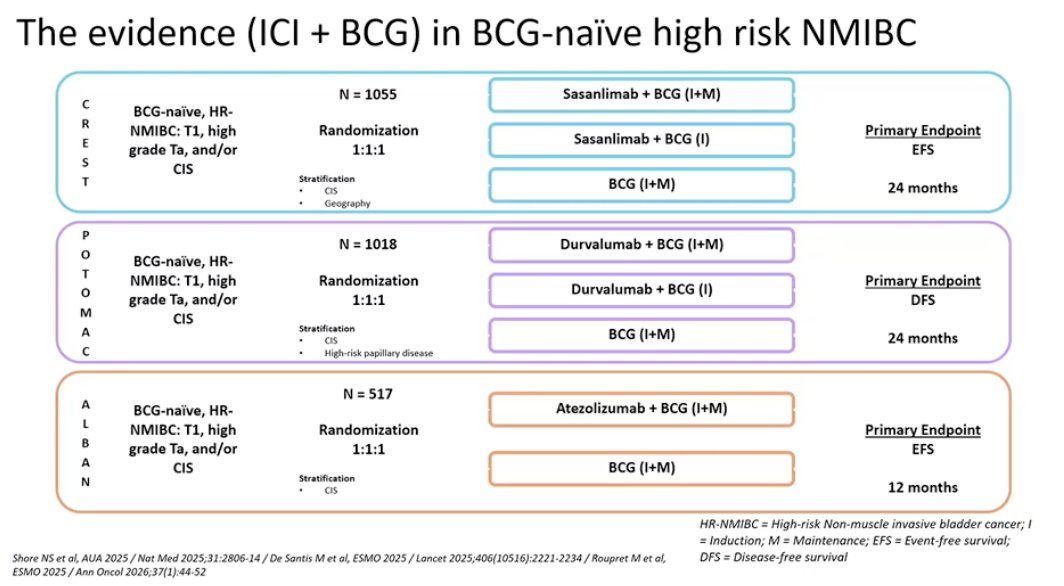
He highlighted two key takeaways from these trials. First, level 1 evidence now supports the addition of immune checkpoint inhibition to intravesical BCG in the treatment of BCG naïve high risk NMIBC. Second, the combination of immune checkpoint inhibitors with BCG appears to provide meaningful clinical benefit with an acceptable safety profile in patients with BCG naïve high-risk disease who are at the greatest risk of progression and metastasis. He noted, however, that the patient discussed in this case would not fall into this category, as he has BCG unresponsive disease.1-3
Notably, these three trials were well designed, randomized, international studies that collectively enrolled more than 2,500 patients. Importantly, differences in trial design and patient populations mean that each study addressed slightly different clinical questions. The CREST and POTOMAC trials enrolled a higher risk NMIBC population, with approximately 58 percent of patients having T1 disease, and a control arm that included adequate BCG maintenance. Both trials demonstrated nearly identical improvements in high grade event free or disease-free survival, supporting the addition of PD-1 inhibition to adequate BCG therapy in this higher risk population. In contrast, the ALBAN trial enrolled a lower risk high risk population, with only 39 percent of patients having T1 disease and a truncated BCG maintenance schedule of 12 months. This study did not demonstrate an event free survival benefit and included low grade recurrences as events, highlighting how differences in study design and patient selection can influence trial outcomes.1-3
He also reviewed the biological rationale underlying BCG unresponsive disease, highlighting the concept of adaptive immune resistance following intravesical BCG therapy. Studies have demonstrated that BCG exposure can lead to increased PD-L1 expression within the tumor microenvironment, particularly among nonresponders. This adaptive upregulation of immune checkpoint pathways may contribute to resistance to BCG (As shown below), providing a biological rationale for investigating immune checkpoint inhibition in this disease setting.

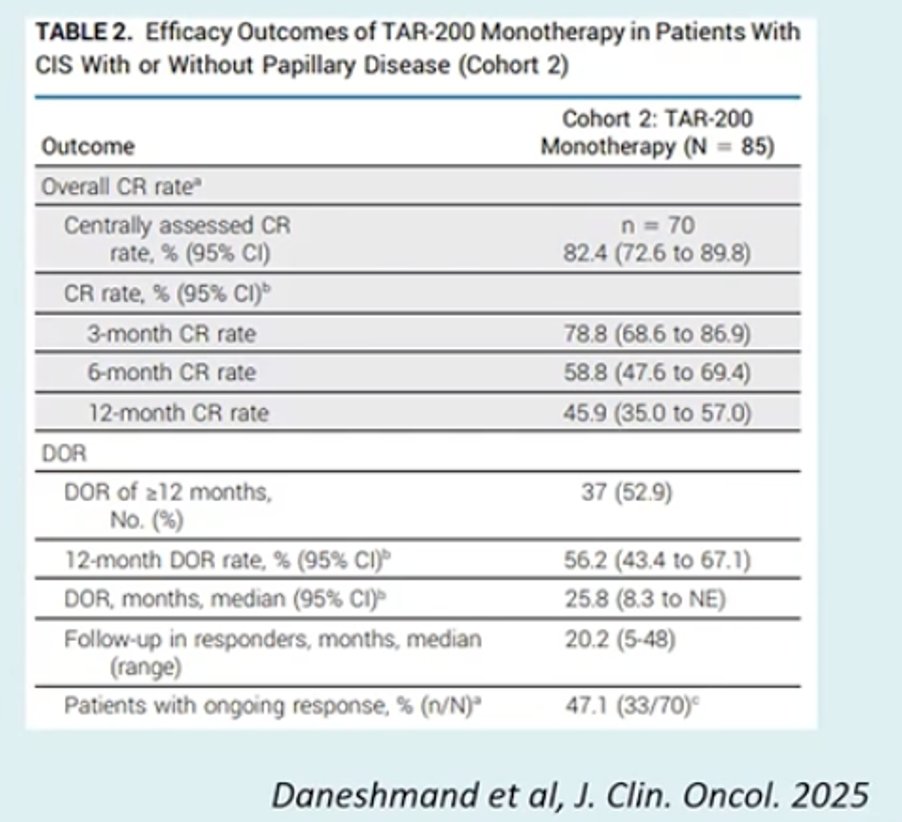
Dr. Bivalacqua reviewed the role of immune checkpoint inhibitor monotherapy in BCG unresponsive NMIBC with CIS. Several studies have evaluated this approach, including KEYNOTE 057 with pembrolizumab,4 SWOG S1605 with atezolizumab and cetrelimab,5 and the GU16 243 ADOPT BLADDER trial with durvalumab. Across these trials, the complete response rate at twelve months in the CIS population has been approximately 20 percent. He also reviewed currently available FDA approved therapies for BCG unresponsive CIS with or without papillary disease, including systemic pembrolizumab, intravesical nadofaragene firadenovec, and the combination of N 803 with BCG. In addition, newer intravesical therapies such as TAR 200 delivering gemcitabine are emerging as potential treatment options in this space.
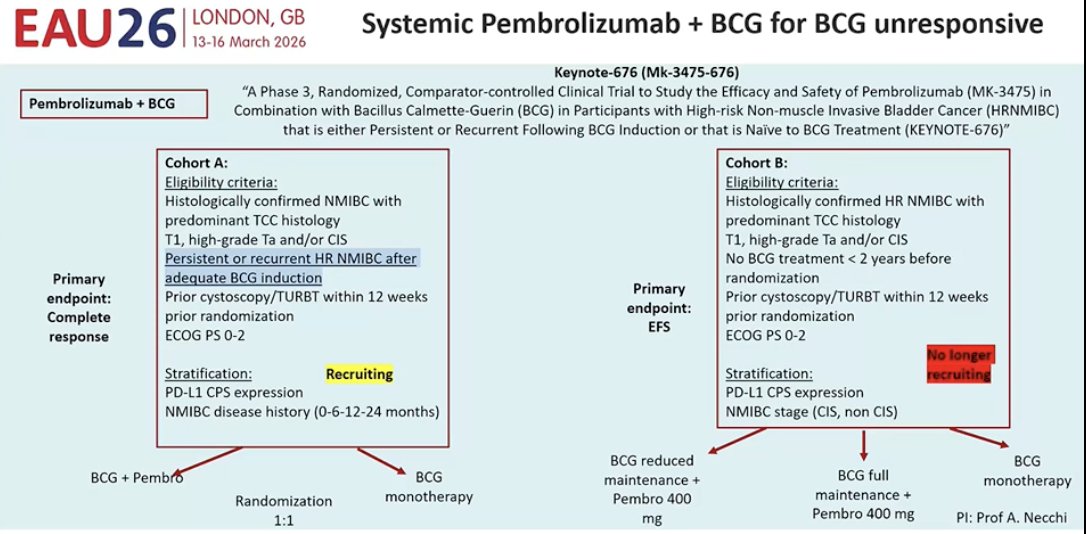
He also noted that one ongoing study is currently evaluating this strategy in the BCG unresponsive setting. The phase 3 KEYNOTE 676 trial is investigating systemic pembrolizumab in combination with intravesical BCG in patients with high risk NMIBC that is persistent or recurrent following BCG induction. In this study, patients are randomized to receive pembrolizumab plus BCG or BCG alone, with complete response as the primary endpoint for the BCG unresponsive cohort. This trial is still recruiting, and results are not yet available. The trial design is shown below.
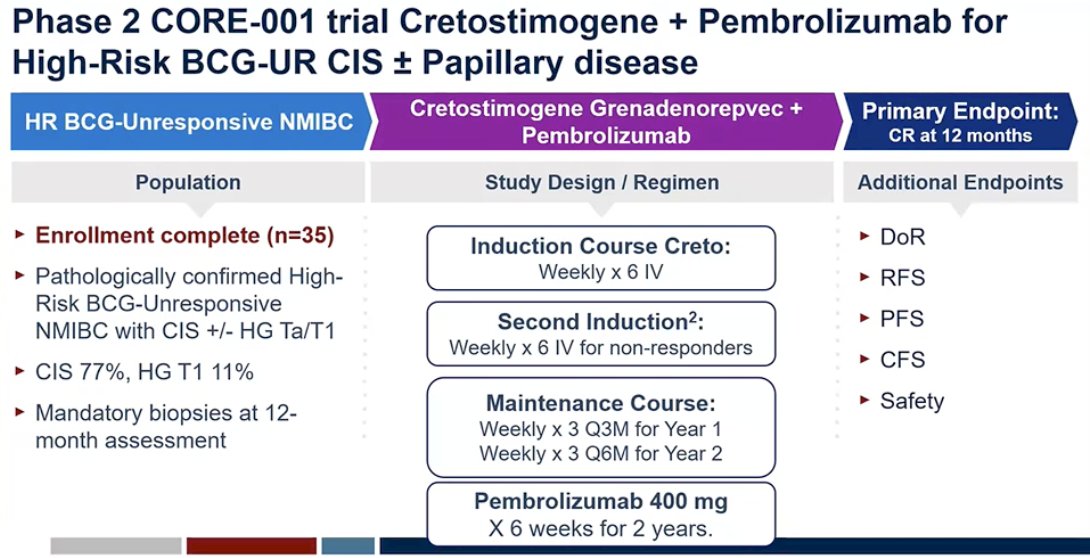
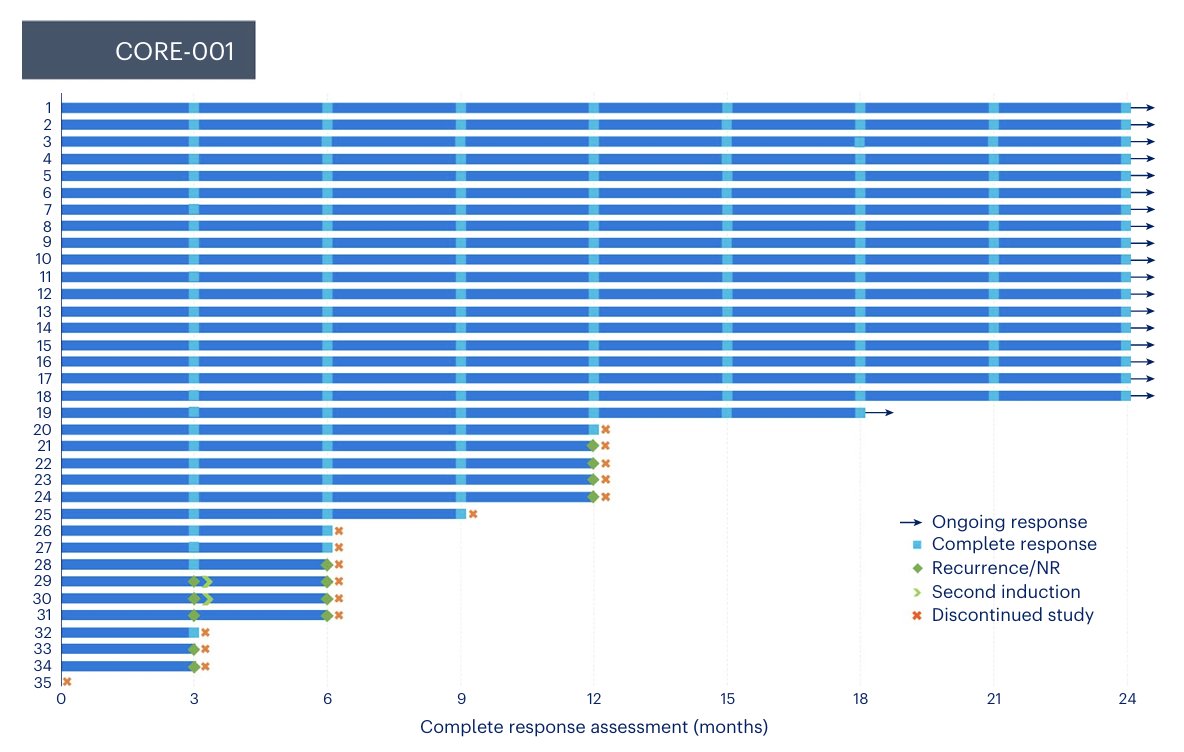
Moreover, he went on to discuss the phase 2 CORE-001 trial evaluating cretostimogene grenadenorepvec in combination with pembrolizumab in patients with high-risk BCG-unresponsive NMIBC with CIS ± papillary disease.8 The study enrolled 35 patients, the majority with CIS, and required mandatory biopsies at the 12-month assessment. The treatment regimen included intravesical cretostimogene administered weekly for six weeks as induction, with a second induction for non-responders, followed by maintenance therapy, together with pembrolizumab given every six weeks for up to two years. The primary endpoint of the study was complete response at 12 months. The study design is shown below.8
Dr. Bivalacqua concluded with several key points:
- Combination intravesical + ICI strategies, which may have synergistic effects, are likely needed to achieve more durable responses and meaningfully impact quality of life and bladder preservation in patients with NMIBC.
- When evaluating new therapies, attention should be placed on complete response rates at 24 months and durability of response rather than early response alone.
- Cost considerations, along with the overall risk–benefit profile of these emerging combination approaches, will also be critical when selecting future treatment strategies.
Presented by: Trinity Bivalacqua, MD, PhD, Director of Urologic Oncology, Co-Director of the Genitourinary Cancer Service Line, Abramson Cancer Center, Professor of Surgery at the Hospital of the University of Pennsylvania, Philadelphia, PA
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:- Roupret M, Bertaut A, Pignot G, Neuzillet Y, Houede N, Mathieu R, Corbel L, Besson D, Seisen T, Jaffrelot L, Lebacle C, Champiat S, Lebdai S, Timsit MO, Thibault C, Goeman L, Juárez Soto Á, La C, Léger C, Loriot Y. ALBAN (GETUG-AFU 37): a phase III, randomized, open-label international trial of intravenous atezolizumab and intravesical Bacillus Calmette-Guérin (BCG) versus BCG alone in BCG-naive high-risk, non-muscle-invasive bladder cancer (NMIBC). Ann Oncol. 2026 Jan;37(1):44-52. doi: 10.1016/j.annonc.2025.09.017. Epub 2025 Oct 17. PMID: 41110692.
- Steinberg GD, Shore ND, Redorta JP, Galsky MD, Bedke J, Ku JH, Kretkowski M, Hu H, Penkov K, Vermette JJ, Tarazi JC, Randall AE, Pierce KJ, Saltzstein D, Powles TB. CREST: phase III study of sasanlimab and Bacillus Calmette-Guérin for patients with Bacillus Calmette-Guérin-naïve high-risk non-muscle-invasive bladder cancer. Future Oncol. 2024 May;20(14):891-901. doi: 10.2217/fon-2023-0271. Epub 2024 Jan 8. PMID: 38189180.
- De Santis M, Palou Redorta J, Nishiyama H, Krawczyński M, Seyitkuliev A, Novikov A, Guerrero-Ramos F, Zukov R, Kato M, Kawahara T, Goeman L, Puente J, Hellmis E, Powles T, Radziszewski P, Gust KM, Vasey P, Bigot P, Fradet Y, Hunting J, Armstrong J, Boulos S, Hois S, Shore ND; POTOMAC Investigators. Durvalumab in combination with BCG for BCG-naive, high-risk, non-muscle-invasive bladder cancer (POTOMAC): final analysis of a randomised, open-label, phase 3 trial. Lancet. 2025 Nov 8;406(10516):2221-2234. doi: 10.1016/S0140-6736(25)01897-5. Epub 2025 Oct 17. PMID: 41115436.
- Necchi A, Roumiguié M, Kamat AM, Shore ND, Boormans JL, Esen AA, Lebret T, Kandori S, Bajorin DF, Krieger LEM, Niglio SA, Uchio EM, Seo HK, de Wit R, Singer EA, Grivas P, Nishiyama H, Li H, Baranwal P, Van den Sigtenhorst-Fijlstra M, Kapadia E, Kulkarni GS. Pembrolizumab monotherapy for high-risk non-muscle-invasive bladder cancer without carcinoma in situ and unresponsive to BCG (KEYNOTE-057): a single-arm, multicentre, phase 2 trial. Lancet Oncol. 2024 Jun;25(6):720-730. doi: 10.1016/S1470-2045(24)00178-5. Epub 2024 May 10. PMID: 38740030.
- Black PC, Tangen CM, Singh P, McConkey DJ, Lucia MS, Lowrance WT, Koshkin VS, Stratton KL, Bivalacqua TJ, Kassouf W, Porten SP, Bangs R, Plets M, Thompson IM Jr, Lerner SP. Phase 2 Trial of Atezolizumab in Bacillus Calmette-Guérin-unresponsive High-risk Non-muscle-invasive Bladder Cancer: SWOG S1605. Eur Urol. 2023 Dec;84(6):536-544. doi: 10.1016/j.eururo.2023.08.004. Epub 2023 Aug 16. PMID: 37596191; PMCID: PMC10869634.
- Daneshmand S, Van der Heijden MS, Jacob JM, Guerrero-Ramos F, Bögemann M, Simone G, Pieczonka CM, Casco NC, Zainfeld D, Spiegelhalder P, Xylinas E, Cahn D, Lotan Y, Murray KS, Kawahara T, Stromberg K, Martin J, Shukla A, Cutie CJ, Bertzos K, Hampras S, Sweiti H, Necchi A; SunRISe-1 Study. TAR-200 for Bacillus Calmette-Guérin-Unresponsive High-Risk Non-Muscle-Invasive Bladder Cancer: Results From the Phase IIb SunRISe-1 Study. J Clin Oncol. 2025 Nov 20;43(33):3578-3588. doi: 10.1200/JCO-25-01651. Epub 2025 Jul 30. Erratum in: J Clin Oncol. 2025 Oct 10;43(29):3231. doi: 10.1200/JCO-25-02053. PMID: 40737582; PMCID: PMC12622271.
- Hahn NM, O'Donnell MA, Efstathiou JA, Zahurak M, Rosner GL, Smith J, Kates MR, Bivalacqua TJ, Tran PT, Song DY, Baras AS, Matoso A, Choi W, Smith KN, Pardoll DM, Marchionni L, McGuire B, Grace Phelan M, Johnson BA 3rd, O'Neal T, McConkey DJ, Rose TL, Bjurlin M, Lim EA, Drake CG, McKiernan JM, Deutsch I, Anderson CB, Lamm DL, Geynisman DM, Plimack ER, Hallman MA, Horwitz EM, Al-Saleem E, Chen DYT, Greenberg RE, Kutikov A, Guo G, Masterson TA, Adra N, Kaimakliotis HZ. A Phase 1 Trial of Durvalumab in Combination with Bacillus Calmette-Guerin (BCG) or External Beam Radiation Therapy in Patients with BCG-unresponsive Non-muscle-Invasive Bladder Cancer: The Hoosier Cancer Research Network GU16-243 ADAPT-BLADDER Study. Eur Urol. 2023 Jun;83(6):486-494. doi: 10.1016/j.eururo.2023.01.017. Epub 2023 Jan 28. PMID: 36717286; PMCID: PMC10192088.
- Li R, Shah PH, Stewart TF, Nam JK, Bivalacqua TJ, Lamm DL, Uchio EM, Geynisman DM, Jacob JM, Meeks JJ, Dickstein R, Pearce SM, Kang SH, Jung SI, Kamat AM, Burke JM, Keegan KA, Steinberg GD. Publisher Correction: Oncolytic adenoviral therapy plus pembrolizumab in BCG-unresponsive non-muscle-invasive bladder cancer: the phase 2 CORE-001 trial. Nat Med. 2024 Aug;30(8):2377. doi: 10.1038/s41591-024-03157-6. Erratum for: Nat Med. 2024 Aug;30(8):2216-2223. doi: 10.1038/s41591-024-03025-3. PMID: 38956199.