(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to "Common Problems and Controversies in Bladder Cancer: Rapid-Fire Debates" session, developed and led by Dr. Ashish Kamat. Kamat presented a case study of a young gentleman with EAU high-risk non-muscle invasive bladder cancer (NMIBC), following which Drs. Neal Shore and Ekaterina Laukhtina argued whether BCG + immuno-oncology (IO) therapy is the ‘bold’ new standard or remains an ‘overreach’ in this setting.
Dr. Kamat presented a case of a 49-year-old marathon runner who presented with gross hematuria and was found to have a 4 cm bladder tumor on a CT urogram. He underwent a TURBT that demonstrated high-grade (HG) Ta disease + carcinoma in situ (CIS), with muscle present and uninvolved. No intravesical chemotherapy was instilled post-operatively.

The patient presented to the clinic asking for the ‘BEST’ treatment for his cancer. In other words, do I need BCG alone or BCG plus systemic checkpoint inhibition?
Arguing in favor of BCG + IO, Dr. Neal Shore began by explicitly anchoring his position in levels of evidence. His opening slide contrasted randomized controlled trials as level 1 evidence with progressively weaker forms of data, making clear that his argument rested not on retrospective enthusiasm or single-arm signal seeking, but on three fully accrued phase III randomized studies in the BCG-naïve, high-risk NMIBC space: CREST, POTOMAC, and ALBAN.1-3

He noted that all three studies asked broadly similar questions but did so in somewhat different populations and with different treatment backbones, which is critical when interpreting why two were positive and one was not.
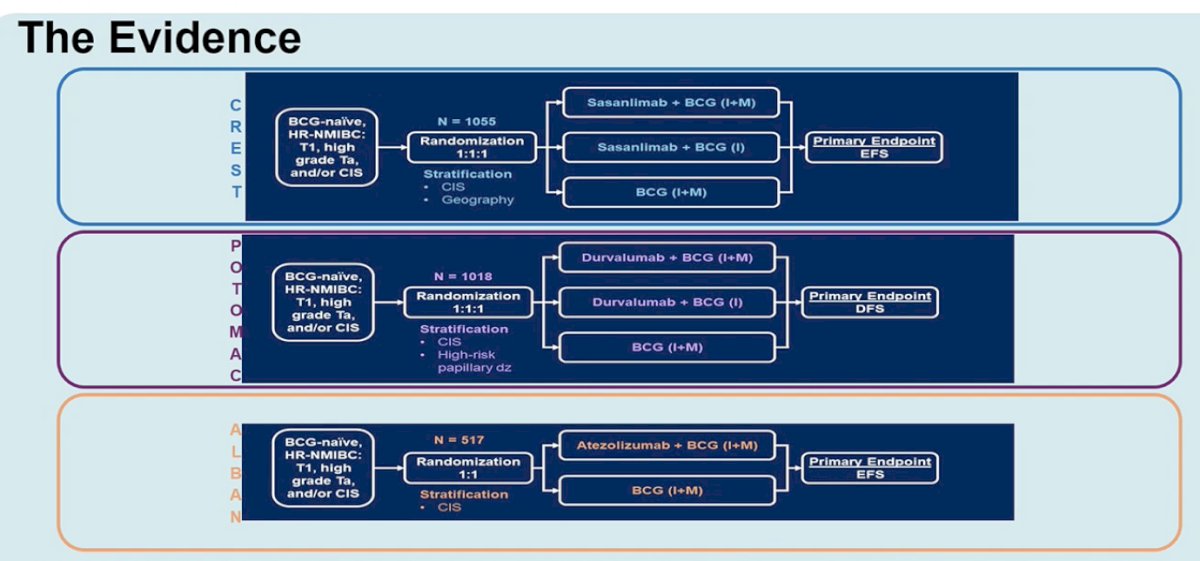
In CREST, 1,055 patients were randomized 1:1:1 to sasanlimab plus BCG induction and maintenance, sasanlimab plus BCG induction alone, or BCG induction and maintenance alone, with event-free survival (EFS) as the primary endpoint. In POTOMAC, 1,018 patients were similarly randomized to durvalumab plus BCG induction and maintenance, durvalumab plus BCG induction only, or BCG induction and maintenance alone, with disease-free survival (DFS) as the primary endpoint. In ALBAN, 517 patients were randomized 1:1 to atezolizumab plus 1 year of BCG versus BCG alone, with EFS as the primary endpoint.
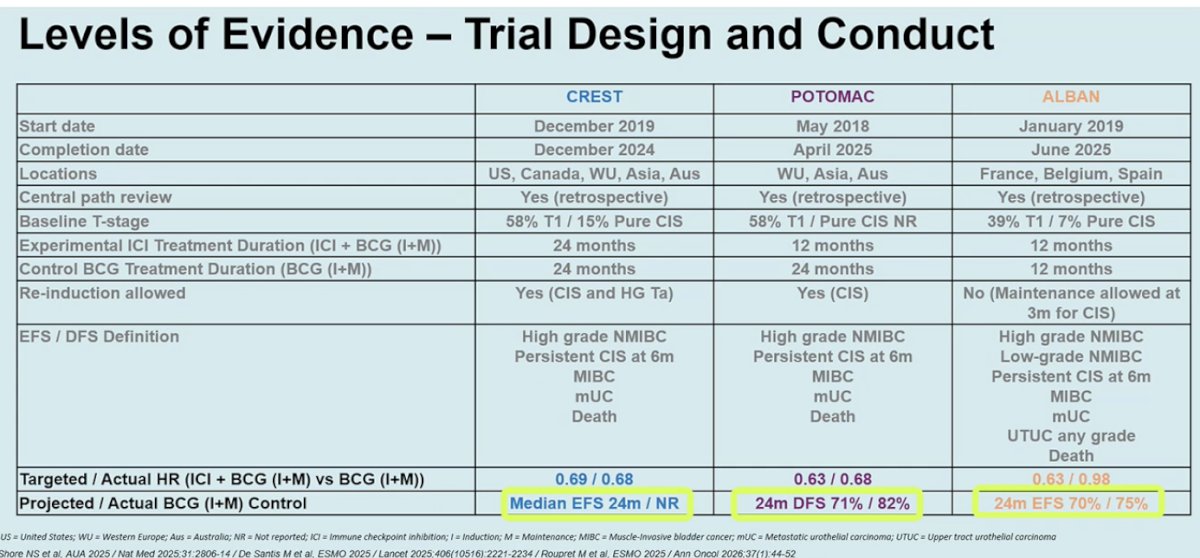
Dr. Shore’s most important comparative slide addressed trial design and conduct. He highlighted that CREST and POTOMAC enrolled what he characterized as “higher-risk” BCG-naïve populations, with 58% T1 disease in each study, whereas ALBAN enrolled a somewhat lower-risk cohort, with 39% T1 disease. He also stressed that the BCG backbone matters. In CREST and POTOMAC, the control arm received induction plus maintenance BCG over 24 months, whereas ALBAN used a 12-month backbone. Re-induction policies and endpoint definitions also differed, further underscoring that these trials were not interchangeable. His synthesis was straightforward: CREST and POTOMAC asked whether adding systemic checkpoint inhibition to adequate induction-plus-maintenance BCG improves outcomes in a high-risk population, and both answered yes; ALBAN asked a somewhat different question in a somewhat different population and answered no. Consistent with that framing, CREST met its primary endpoint with a hazard ratio for EFS of 0.68, with 36-month EFS estimates of 82.1% for sasanlimab plus BCG induction and maintenance versus 74.8% for BCG alone. POTOMAC likewise demonstrated a 32% reduction in the risk of recurrence of high-risk disease or death, with a hazard ratio of 0.68 for durvalumab plus BCG induction and maintenance versus BCG alone. By contrast, ALBAN failed to improve EFS, with a hazard ratio of 0.98.
From there, Dr. Shore shifted the discussion from hazard ratios to clinical consequences. One of his more practical slides focused on what recurrence actually means for a patient with high-risk NMIBC. He reminded the audience that recurrence is not a trivial bookkeeping event; rather, it often initiates an entirely new and more burdensome therapeutic pathway. The slide below summarizes the familiar downstream consequences of recurrent or newly BCG-unresponsive disease: additional salvage therapies such as gemcitabine/docetaxel, nadofaragene firadenovec; more frequent cystoscopies; repeated biopsies and TURBTs; ongoing urinary symptoms; greater cost; and, not infrequently, eventual cystectomy. In other words, his argument was that preventing the first high-risk recurrence has value beyond the primary endpoint because it may prevent the entire cascade of subsequent procedures, treatments, symptoms, and anxiety that follows.

This point was reinforced by a subsequent slide mapping the broad implications of high-risk recurrence and progression, including risk of muscle-invasive disease, metastases, death, additional anesthesia exposure, repeated resections, more intravesical treatments, worsening urinary symptoms, potential incontinence, and possible deterioration of bladder function.

Dr. Shore then connected these recurrence consequences to contemporary guideline language for BCG-unresponsive disease. He showed that once a patient enters that state, the threshold for recommending radical cystectomy becomes much lower. His slide quoted both AUA and EAU guidance to emphasize that persistent or recurrent high-risk disease after adequate BCG frequently leads to a recommendation for cystectomy, with the EAU explicitly describing radical cystectomy as the standard and preferred option in BCG-unresponsive disease. His underlying point was that if BCG plus IO can reduce the risk of those high-risk recurrence events upfront, it may spare some patients from ever entering a disease state in which radical surgery becomes the default recommendation.

Dr. Shore acknowledged that IO intensification in this setting is associated with increased toxicity.
In CREST, the addition of sasanlimab to BCG increased grade 3–4 adverse events from 26% to 49%, grade 3–4 treatment-related adverse events from 6% to 29%, grade 3–4 immune-related adverse events from 0% to 16%, corticosteroid use from less than 1% to 20%, and treatment discontinuation due to TRAEs from 9% to 26%.
In POTOMAC, durvalumab plus BCG increased grade 3–4 treatment-related adverse events from 4% to 21%, and in ALBAN the atezolizumab combination also produced higher rates of TRAEs and grade 3 or higher TRAEs than BCG alone. Nonetheless, Dr. Shore noted that these added risks were ‘acceptable’ in a carefully selected population at the highest risk of progression and metastasis, particularly when weighed against the clinical impact of recurrence, BCG-unresponsive disease, and eventual cystectomy, and that many of these toxicities can be safely managed in the outpatient setting by either experienced urologists or medical oncologists.

But what really matters to patients such as the one in the initial case study? Dr. Shore showed a patient-preference slide indicating that bladder preservation is highly valued by this population, with 76% of patients rating bladder preservation as “extremely important” and another 18% rating it “very important.”4 He used this not to argue against evidence-based care, but to frame why shared decision-making matters so much in this disease state. If a patient places enormous value on bladder preservation, and if level 1 evidence now suggests that adding checkpoint inhibition to BCG can improve event-free or disease-free outcomes in a subset of high-risk BCG-naïve patients, then that combination deserves to be part of the conversation rather than reserved as a fringe option.

His final arguments therefore moved away from a one-size-fits-all recommendation and toward a personalized treatment framework. He showed a decision-making schema centered on disease characteristics, efficacy profile, safety and tolerability, treatment schedule and duration, access and cost, patient comorbidities, patient preferences and quality of life, and the importance of management by informed specialists. This was an important refinement of his “pro” position: he was not arguing that every patient with high-risk BCG-naïve NMIBC must receive BCG + IO, but rather that the field now has sufficiently strong evidence to justify offering it to appropriate patients, especially those at the highest biologic risk.

Dr. Shore concluded his argument in favor of BCG+IO for BCG-naïve, high-risk NMIBC patients as follows:
- Level 1 evidence now supports the addition of immune checkpoint inhibition to intravesical BCG in BCG-naïve high-risk NMIBC
- This combination provides meaningful clinical benefit with an acceptable risk profile in patients at the highest risk of recurrence, progression, and metastasis
- Shared decision-making remains the standard of care
Taken together, he argued that BCG+IO should no longer be viewed as speculative intensification, but as a logical next step in the management of select patients with BCG-naïve high-risk NMIBC.
Arguing against the routine use of BCG plus immune checkpoint inhibition in BCG-naïve, high-risk NMIBC, Dr. Ekaterina Laukhtina began her presentation with a clear message: “Not so fast — BCG + IO is overkill.” Her argument centered on the balance between undertreatment and overtreatment in high-risk NMIBC and questioned whether the emerging enthusiasm for systemic immunotherapy in this disease state is justified based on the current evidence.
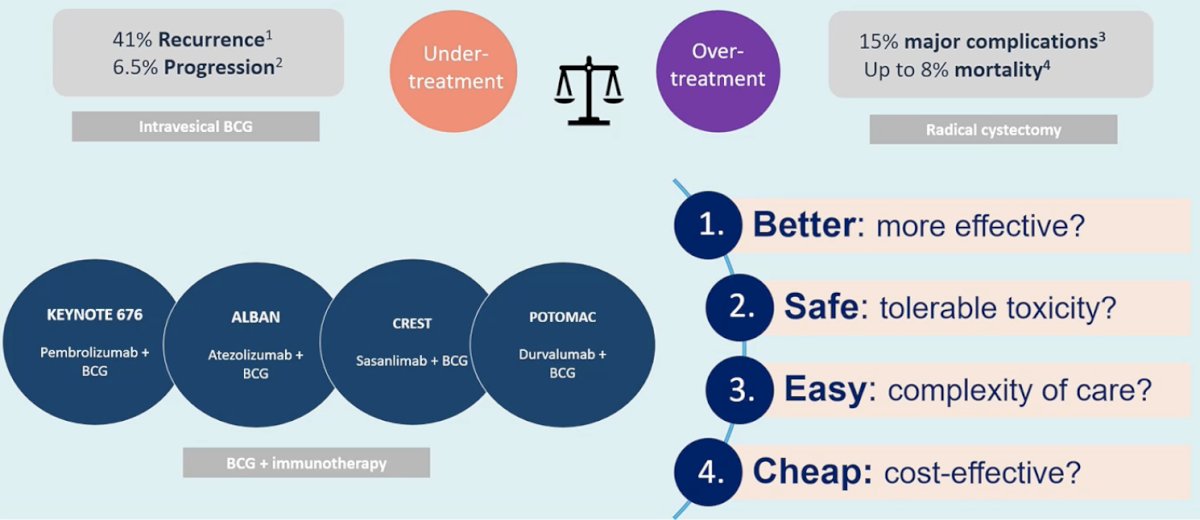
She opened by framing the broader therapeutic dilemma in high-risk NMIBC. Despite optimal intravesical BCG therapy, recurrence rates remain substantial, with approximately 41% of patients experiencing recurrence and about 6.5% progressing to muscle-invasive disease. At the same time, radical cystectomy—often the definitive treatment for BCG-unresponsive disease—carries considerable morbidity, including major complication rates approaching 15% and perioperative mortality of up to 8%. Thus, clinicians must constantly balance the risks of undertreatment against the risks of overtreatment.5-8
Against this background, multiple trials have explored the addition of immune checkpoint inhibition to BCG in BCG-naïve disease, including KEYNOTE-676 (pembrolizumab + BCG), ALBAN (atezolizumab + BCG), CREST (sasanlimab + BCG), and POTOMAC (durvalumab + BCG). However, Dr. Laukhtina emphasized that the existence of trials does not automatically justify broad adoption of combination therapy.
She structured her argument around four practical questions clinicians should ask before embracing BCG plus IO: Is it better (more effective)? Is it safe (tolerable toxicity)? Is it easy (complexity of care)? And is it cheap (cost-effective)?
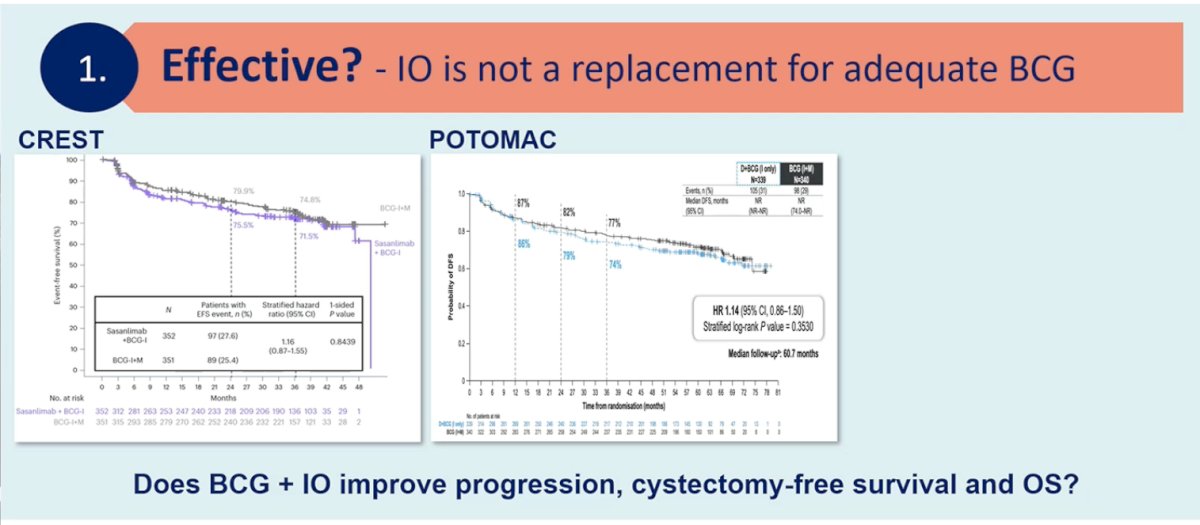
First, she challenged the assumption that adding checkpoint inhibition clearly improves meaningful outcomes. Her central point was that immune checkpoint inhibitors are not a replacement for adequate BCG therapy. She presented Kaplan–Meier curves from the CREST and POTOMAC trials demonstrating improvements in recurrence-related endpoints. However, she emphasized that these benefits largely relate to recurrence-based endpoints rather than hard oncologic outcomes such as progression, cystectomy-free survival, metastasis-free survival, or overall survival. A meta-analysis including 1,899 patients across available trials showed a hazard ratio of 0.77 (95% CI 0.60–0.97) for recurrence-related time-to-event endpoints, corresponding to a number needed to treat of approximately 25 patients at two years to prevent one recurrence event. While statistically significant, she argued that this magnitude of benefit may be modest when weighed against the broader implications of systemic immunotherapy.
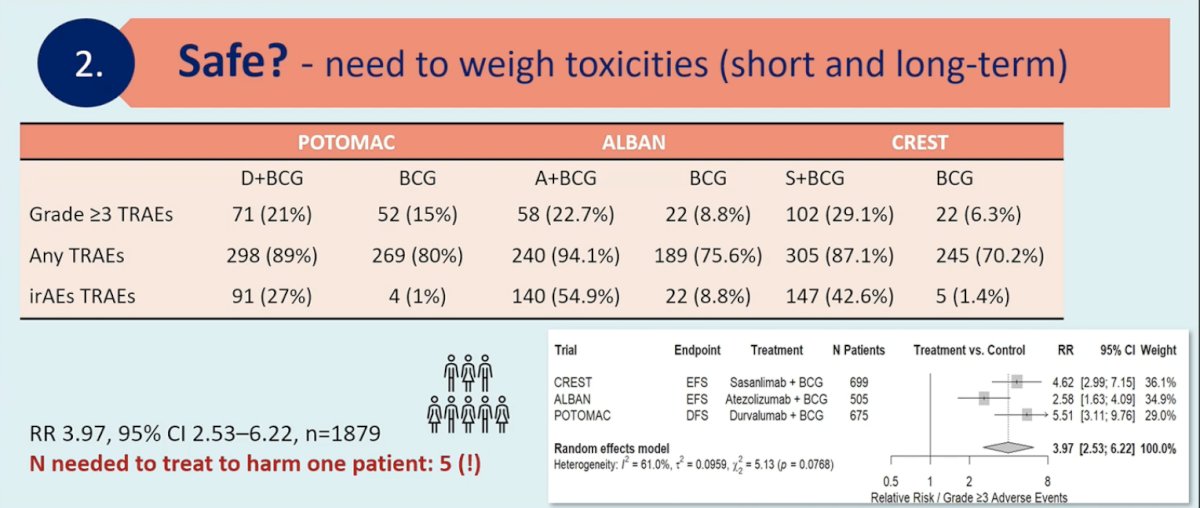
Her second major argument focused on toxicity. Using pooled data from POTOMAC, ALBAN, and CREST, she demonstrated consistently higher rates of adverse events with the addition of checkpoint inhibition.
- In POTOMAC, grade ≥3 treatment-related adverse events occurred in 21% of patients receiving durvalumab plus BCG compared with 15% receiving BCG alone.
- In ALBAN, grade ≥3 events occurred in 22.7% with atezolizumab plus BCG versus 8.8% with BCG alone.
- In CREST, grade ≥3 events were reported in 29.1% of patients receiving sasanlimab plus BCG compared with 6.3% with BCG alone.
The incidence of immune-related adverse events was also substantially higher with combination therapy, reaching as high as 54.9% in the atezolizumab arm of ALBAN compared with 8.8% with BCG alone.
A pooled meta-analysis of approximately 1,879 patients demonstrated nearly a fourfold increase in the risk of grade ≥3 adverse events (RR 3.97, 95% CI 2.53–6.22). Importantly, she highlighted that the number needed to harm for one patient experiencing a severe adverse event was approximately five.9 In her view, exposing five patients to severe toxicity to prevent a single recurrence event raises important questions about the overall therapeutic balance.
Dr. Laukhtina then turned to the issue of the complexity of care. She argued that introducing systemic immunotherapy into a disease traditionally managed by urologists fundamentally alters the care ecosystem. Intravesical BCG therapy is typically delivered and monitored by urologists, whereas systemic checkpoint inhibitors are usually administered and managed by medical oncologists. This shift may fragment care pathways and potentially delay key decision points, such as early referral for radical cystectomy in patients with high-risk disease. She emphasized that multidisciplinary care is valuable but warned that the addition of systemic immunotherapy could inadvertently complicate clinical workflows and blur responsibility for longitudinal disease management.
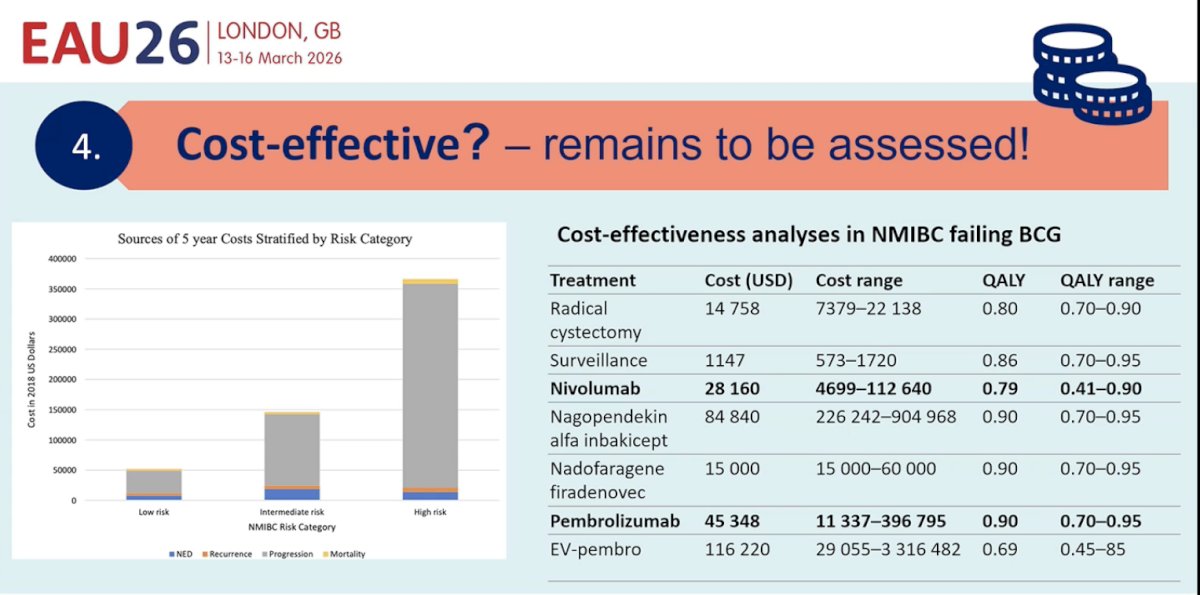
Her fourth concern related to cost-effectiveness. Systemic immunotherapies remain expensive, and robust cost-effectiveness analyses in the BCG-naïve NMIBC setting are lacking. She presented comparative cost data from NMIBC treatment strategies, noting that immunotherapy-based regimens such as pembrolizumab or nivolumab-based approaches can cost tens of thousands of dollars annually. For example, pembrolizumab-based strategies have been estimated at approximately $45,000 per year, with ranges extending well beyond that depending on the duration of therapy. Similarly, nivolumab-based regimens may approach $28,000 annually, while novel agents such as nogapendekin alfa inbakicept can exceed $80,000. In contrast, surveillance strategies or even radical cystectomy may be substantially less costly in certain models.10,11 Because long-term survival advantages have not yet been demonstrated for BCG plus IO combinations in the BCG-naïve setting, she argued that widespread adoption before robust cost-effectiveness analyses may be premature.
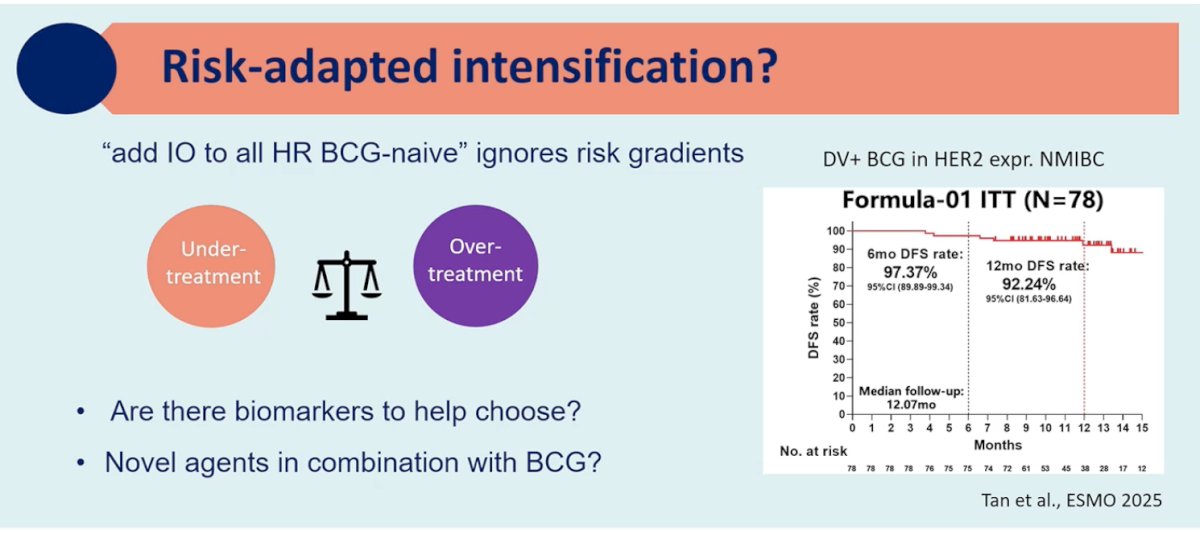
Dr. Laukhtina highlighted the heterogeneity of risk within the high-risk NMIBC category. She argued that the concept of adding immune checkpoint inhibition to all BCG-naïve high-risk patients ignores important risk gradients within this population. Some patients may indeed benefit from early treatment intensification, whereas others may be adequately managed with standard BCG therapy alone. Rather than universal escalation, she advocated for a risk-adapted intensification strategy that incorporates biomarkers, improved molecular risk stratification, and the development of more targeted intravesical or combination approaches. She also highlighted ongoing research exploring novel combinations with BCG, including HER2-targeted antibody–drug conjugates such as disitamab vedotin in HER2-expressing NMIBC, which demonstrated promising early disease-free survival rates in exploratory cohorts.
Her final slide summarized the core argument succinctly: BCG plus IO is not clearly more effective in terms of meaningful long-term outcomes, it introduces substantially higher toxicity, it complicates care delivery, and its cost-effectiveness remains uncertain. Until these issues are better addressed and risk-adapted strategies are developed, she argued that routine use of BCG plus checkpoint inhibition for all patients with BCG-naïve high-risk NMIBC represents overtreatment rather than a new standard of care.
Presented by:
- Ashish M. Kamat, MD, MBBS, Endowed Professor of Urologic Oncology (Surgery) and Cancer Research, Department of Urology, University of Texas MD Anderson Cancer Center, Houston, TX
- Neal D. Shore, MD, FACS, Medical Director, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC, USA
- Ekaterina Laukhtina, MD, Medical University of Vienna, Vienna, Austria
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026
References:- Shore ND, Powles TB, Bedke J, et al. Sasanlimab plus BCG in BCG-naive, high-risk non-muscle invasive bladder cancer: the randomized phase 3 CREST trial. Nat Med. 2025;31(8):2815.
- De Santis M, Palou Redorta J, Nishiyama N, et al. Durvalumab in combination with BCG for BCG-naive, high-risk, non-muscle-invasive bladder cancer (POTOMAC): final analysis of a randomised, open-label, phase 3 trial. Lancet. 2025;406(10516):2221-2234.
- Roupret M, Bensalah K, Pfister C, et al. ALBAN (GETUG-AFU 37): a phase III, randomized, open-label international trial of intravenous atezolizumab and intravesical Bacillus Calmette-Guérin (BCG) versus BCG alone in BCG-naive high-risk, non-muscle-invasive bladder cancer (NMIBC). Ann Oncol. 2026;37(1):12-23.
- Kopenhafer L, Thompson A, Chang J, et al. Patient experience and unmet needs in high-risk nonmuscle-invasive bladder cancer: Insights from qualitative interviews and a cross-sectional survey. Urol Oncol. 2024;42(3):70.e1-70.e10.
- Subiela JD, Rodriguez-Faba O, Breda A, et al. Diagnostic accuracy of urinary biomarkers compared with cystoscopy for surveillance of non-muscle-invasive bladder cancer: a systematic review and meta-analysis. BJU Int. 2025;135(1):17-31.
- Pijpers OM, Vriesema JLJ, Kiemeney LALM, et al. Patient preferences for surveillance strategies in non-muscle-invasive bladder cancer: balancing diagnostic certainty with procedural burden. Eur Urol Oncol. 2025;8(2):285-293.
- Katsimperis S, Bruins HM, Veskimäe E, et al. Urinary biomarkers for the surveillance of non-muscle-invasive bladder cancer: ready to replace cystoscopy? Urol Focus. 2023;9(2):328-336.
- Zakaria AS, Santos F, Dragomir A, et al. Cost-effectiveness of surveillance strategies for non-muscle-invasive bladder cancer using urinary biomarkers. Can Urol Assoc J. 2014;8(11-12):E801-E809.
- Roessler N, Mariorano BA, Miszczyk M, et al. First-line treatments for BCG-naïve non-muscle invasive bladder cancer: a systematic review and meta-analysis. World J Urol. 2026;44(1):76.
- Mossanen M, Wang Y, Szymaniak J, et al. Evaluating the cost-effectiveness of surveillance schedules in patients with non–muscle-invasive bladder cancer. World J Urol. 2019;37(12):2699-2706.
- D’Andrea D, Soria F, Abufaraj M, et al. Novel urinary biomarkers and the future of surveillance in non–muscle-invasive bladder cancer. Eur Urol Oncol. 2025;8(1):12-21.