(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to a session on risk stratification for non-muscle invasive bladder cancer (NMIBC). Dr. Trinity Bivalacqua presented translational and early clinical findings from Cohort A of the CORE-008 study evaluating intravesical cretostimogene grenadenorepvec in patients with high-risk, BCG-naïve NMIBC.
Guidelines currently recommend intravesical BCG therapy or radical cystectomy (RC) for patients with high-risk NMIBC. However, important challenges exist with both approaches. Intravesical BCG demonstrates variable durability across studies, may lead to treatment-limiting adverse effects, and has been affected by ongoing global supply shortages. Radical cystectomy, while effective oncologically, carries substantial morbidity and complication risk.
Cretostimogene is an oncolytic immunotherapy with dual mechanisms of action. It selectively replicates in and lyses cancer cells while simultaneously amplifying the immune response against bladder tumors. CORE-008 is a phase 2, multi-arm, multi-cohort, open-label clinical trial designed to evaluate the safety and efficacy of cretostimogene across a broad population of patients with high-risk NMIBC.
CORE-008 Cohort A evaluates patients with high-risk, BCG-naïve NMIBC with carcinoma in situ (CIS). Eligible patients include those with no prior BCG exposure, BCG exposure greater than 24 months earlier, or patients who received only 1–2 BCG doses within the preceding 24 months.
Participants were randomized 1:1 to one of two administration strategies:
- Original administration (5-step protocol): Saline wash, DDM wash, DDM dwell, Saline wash, Cretostimogene dwell
- Optimized administration (2-step protocol): DDM Cretostimogene dwell
Treatment response assessments include urine cytology, serial cystoscopy with directed biopsy, and axial imaging, when clinically indicated. The primary endpoint of the study is complete response (CR) at any time.
Patient demographics demonstrate that the study population largely reflects a typical high-risk NMIBC cohort. The majority of patients were male (90.7%), White (92.6%), and older than 65 years (88.8%).
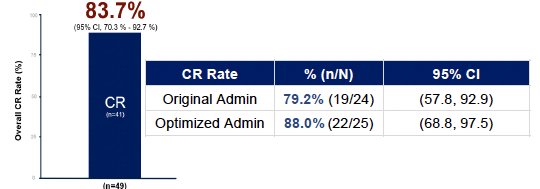
As of September 1, 2025, the median follow-up was 4.6 months, with an overall complete response rate of 83.7%. Importantly, treatment activity was consistent across patient subgroups.
Notably, no patients required radical cystectomy, and there were no treatment-related progressions to muscle-invasive bladder cancer or metastatic urothelial carcinoma. Three patients experienced stage reclassification within the NMIBC spectrum.
From a safety standpoint, there were no grade ≥3 treatment-related adverse events, no serious adverse events, and no treatment-related deaths. Furthermore, there were no treatment discontinuations attributed to therapy.
When stratified by administration strategy, the complete response rates were:
- Original administration protocol: 79.2% (19/24)
- Optimized administration protocol: 88% (22/25)
These findings suggest robust response rates with both administration strategies, with numerically higher responses observed with the optimized two-step protocol.
The study also incorporated translational biomarker analyses evaluating viral replication and transgene expression.
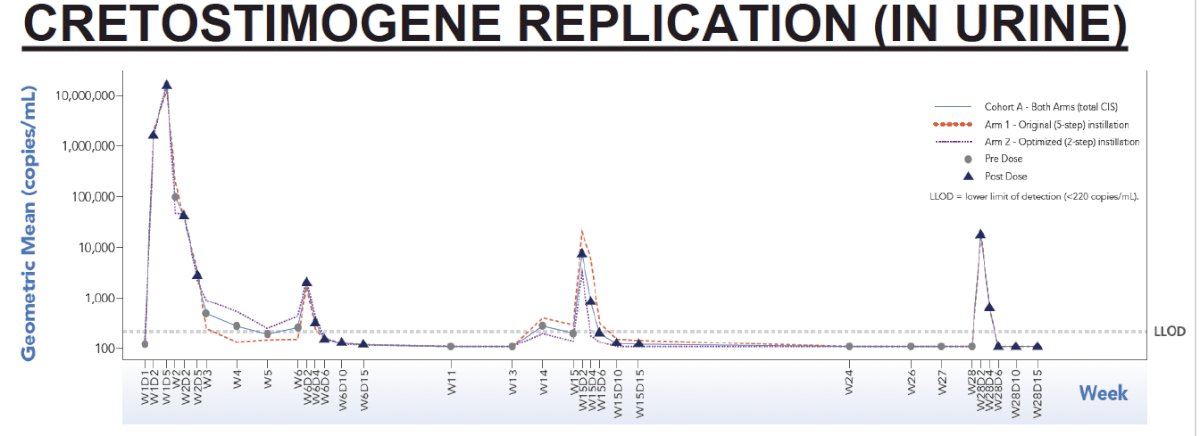
Cretostimogene replication in urineBaseline urine samples from 53 patients demonstrated no detectable cretostimogene levels and low endogenous GM-CSF concentrations. During induction therapy, transient increases in viral levels were observed, followed by declines below the limit of detection after induction and maintenance dosing. Importantly, there was no evidence of latent or prolonged viral replication. Viral levels were similar between the two administration arms. These findings are consistent with prior observations from the BOND-003 Cohort C study in BCG-unresponsive NMIBC with CIS.
The observed effective viral clearance also supports the possibility of relaxed close-contact precautions for treated patients.
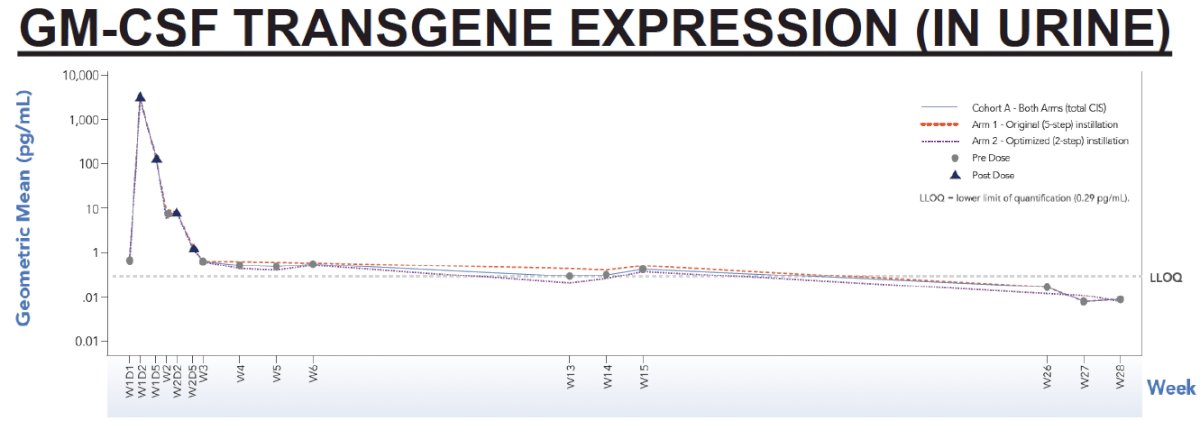
Urinary GM-CSF levels increased robustly following the first induction dose and declined to near-baseline levels within approximately one week, confirming successful transgene expression. GM-CSF levels during maintenance therapy remained close to baseline, consistent with transient expression and the timing of pre-dose sampling.
Importantly, there were no substantial differences in GM-CSF expression between the two treatment arms. The transient expression pattern aligns with the intended mechanism of action of cretostimogene as an oncolytic viral immunotherapy.
Dr. Bivalacqua noted that these early clinical and translational results from CORE-008 Cohort A demonstrate encouraging activity of intravesical cretostimogene in patients with high-risk BCG-naïve NMIBC, with an overall complete response rate of 83.7% and a favorable safety profile characterized by the absence of grade ≥3 treatment-related adverse events.
Importantly, translational biomarker analyses support the mechanistic basis of this therapy, demonstrating transient viral replication, effective viral clearance, and robust but transient GM-CSF transgene expression consistent with the drug’s intended immunotherapeutic mechanism.
Presented by: Trinity Bivalacqua, MD, PhD, Professor, Department of Urology, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Related content: Translational Insights for Cretostimogene Grenadenorepvec for BCG-Naïve Bladder Cancer - Trinity Bivalacqua