(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a late-breaking abstracts session and a presentation by Dr. Maykon Pereira discussing safety and mid-term oncological outcomes from a prospective randomized trial assessing holmium laser en bloc resection versus conventional TURBT for large non-muscle invasive bladder tumors.
Monopolar TURBT fragments specimens and introduces thermal artifacts that may impair pathological assessment and contribute to understaging, particularly in large tumors. En bloc resection with holmium laser has been proposed to improve specimen integrity and perioperative safety. However, previous randomized trials predominantly enrolled small tumors and often used 3 cm as a feasibility threshold; evidence in tumors >3 cm remains limited. Dr. Pereira and colleagues conducted a prospective, randomized trial comparing holmium laser en bloc resection with monopolar TURBT in patients with bladder tumors >3 cm to evaluate perioperative safety, specimen quality, pathological staging, and oncological outcomes.
This prospective, two-center, single-blind, randomized (1:1) trial enrolled patients with bladder tumors >3 cm confirmed by CT or MRI (January 2020 – December 2025). Patients were randomized to holmium laser en bloc resection or monopolar TURBT. Patients undergoing holmium laser en bloc resection had laser settings of 0.4-0.6 J and 20-30 Hz, with a circumferential resection including a 5-10 mm safety margin, and deep dissection until clear visualization of detrusor fibers was encountered:

Holmium laser en bloc resection specimens were extracted based on their size:
- <3.5 cm: intact extraction through the sheath or with grasping forceps
- >3.5 cm: morcellation with preservation of the tumor base

Exclusion criteria included prior bladder cancer, radiological suspicion of ≥pT2 disease, nodal or distant metastases, or prior chemo- or radiotherapy. Central pathology review was predefined, and patients with pT1 disease underwent re-TURBT at 30–60 days. The primary endpoint was detrusor muscle representativeness in the surgical specimen, and secondary endpoints included perioperative complications, bladder perforation, catheterization time, length of stay, residual tumor at re-TURBT, and oncological outcomes.
Ninety-seven patients were analyzed (holmium laser en bloc resection n = 46; TURBT n = 51):

Tumors were larger in the holmium laser en bloc resection group (median 3.5 cm versus 3.1 cm; p=0.031), while patients undergoing TURBT were older (67 years versus 63 years p = 0.066):

Bladder perforation was significantly lower with holmium laser en bloc resection (2.2% versus 21.6%; p = 0.004):
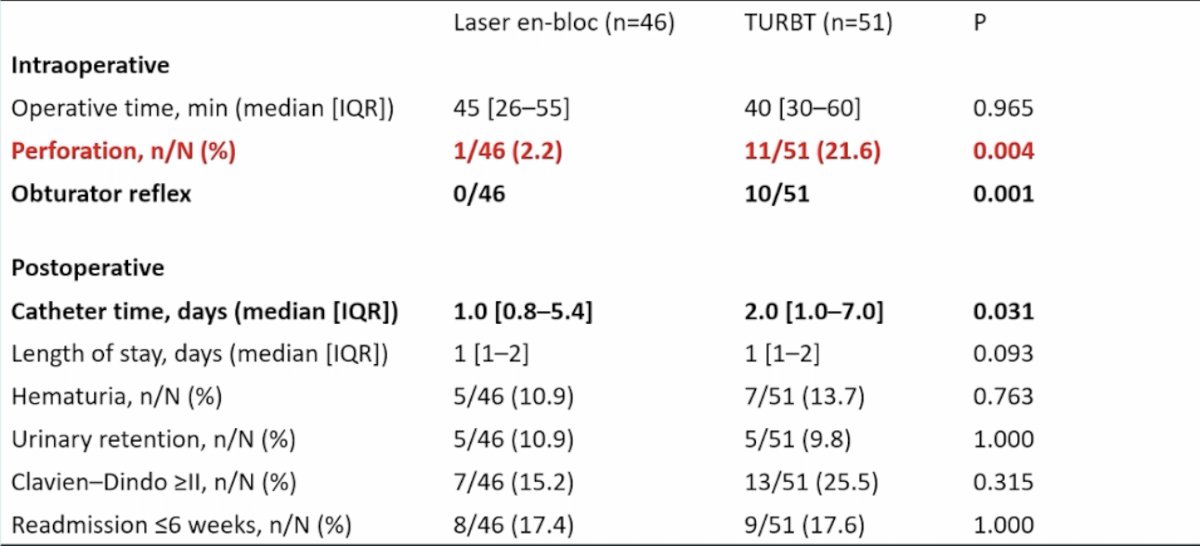
All bladder perforations were defined by visualization of perivesical fat and were managed conservatively. Catheterization time was also shorter (median 24 versus 48 hours; p = 0.031) in the holmium laser en bloc resection group. Operative time, specimen weight, and length of stay were comparable. Detrusor muscle was present in 89.1% of holmium laser en bloc resection and 78.4% of TURBT specimens (p = 0.25). Pathological staging differed significantly, with a higher proportion of T1 tumors after holmium laser en bloc resection (p = 0.01). Overall postoperative complications and Clavien–Dindo distribution were similar between groups. Re-TURBT was performed in 76.1% of holmium laser en bloc resection and 58.8% of TURBT patients (p = 0.08), with no significant difference in residual tumor rates (p = 0.29):

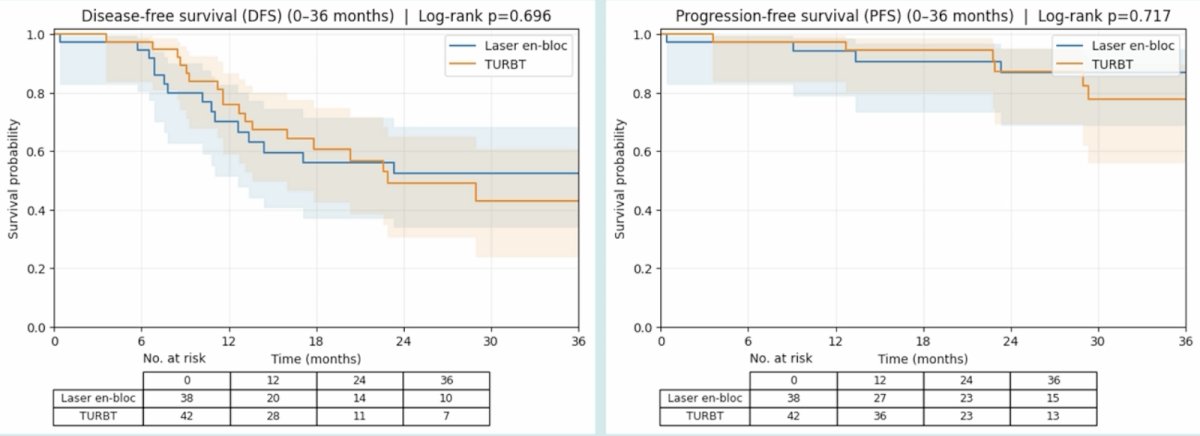
At a mean follow-up of 35 months, disease-free survival and overall survival were comparable between holmium laser en bloc resection and TURBT (disease-free survival log-rank p = 0.696; overall survival log-rank p = 0.717):
Dr. Pereira concluded his presentation discussing safety and mid-term oncological outcomes from a prospective randomized trial assessing holmium laser en bloc resection versus conventional TURBT for large non-muscle invasive bladder tumors with the following take-home points:
- Holmium laser en bloc resection is safe and feasible for bladder tumors >= 3 cm
- En bloc resection reduces bladder perforation and obturator reflex compared with TURBT
- Holmium laser en bloc resection improved pathological staging
- Oncological outcomes were comparable at 35 months
- Holmium laser en bloc resection represents a promising alternative to conventional TURBT for large non-muscle invasive bladder cancer
Presented by: Maykon Pereira, MD, Instituto do Câncer do Estado de São Paulo, São Paulo, Brazil
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.