(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a late-breaking abstracts session and a presentation by Dr. Antoni Vilaseca discussing the final analysis of the phase 1 first-in-human study of an erdafitinib intravesical drug-releasing system in patients with non-muscle invasive bladder cancer harboring select FGFR alterations.
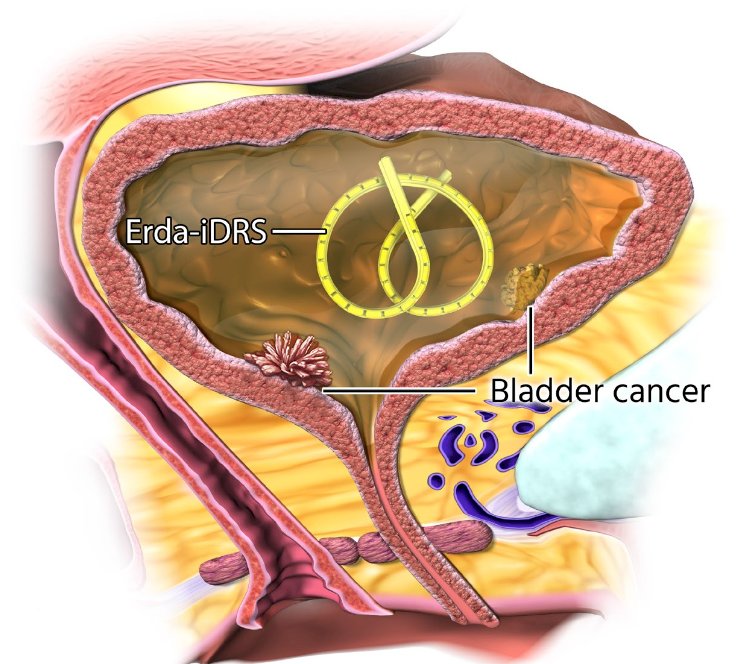
Despite available treatment options for patients with non-muscle invasive bladder cancer, recurrence rates and progression risk remain high. This results in multiple resections or eventually radical cystectomy, underscoring the need for more effective bladder-sparing therapies. FGFR alterations occur in 70% of intermediate risk and 30% of high risk non-muscle invasive bladder cancer tumors and may function as oncogenic drivers. Erdafitinib intravesical drug-releasing (TAR-210) is an intravesical drug-releasing system designed to provide sustained delivery of erdafitinib (pan-FGFR inhibitor) to the bladder in 3-month treatment cycles, aiming to limit systemic toxicities:
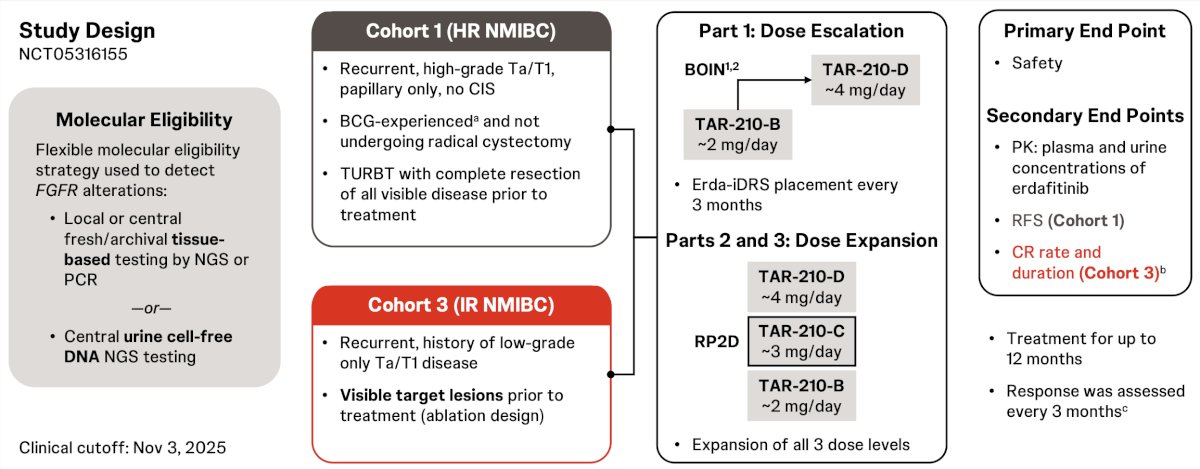
This open-label, multicenter phase 1 study evaluated the safety, pharmacokinetics, and preliminary efficacy of erdafitinib intravesical drug-releasing in patients with non-muscle invasive bladder cancer whose tumors harbor select FGFR alterations.
Cohort 1 patients had recurrent, BCG-experienced high-risk non-muscle invasive bladder cancer (high-grade Ta/T1, papillary only) and refused or were ineligible for radical cystectomy. Before treatment, cohort 1 required all visible tumors to be resected. Cohort 3 patients had recurrent, intermediate-risk non-muscle invasive bladder cancer (Ta/T1) with a history of only low-grade disease. Cohort 3 required unresected tumors at study entry. All patients had FGFR alterations by urine and/or tissue testing. There were 3 different erdafitinib release rates evaluated. The primary endpoint was safety, and secondary endpoints included recurrence-free survival in cohort 1 and complete response rate and duration of complete response in cohort 3 (complete response was defined as the absence of malignant tumors by cystoscopy with negative urine cytology). Response was assessed every 3 months with continued treatment for up to 1 year if recurrence-free (cohort 1) or in complete response (cohort 3):
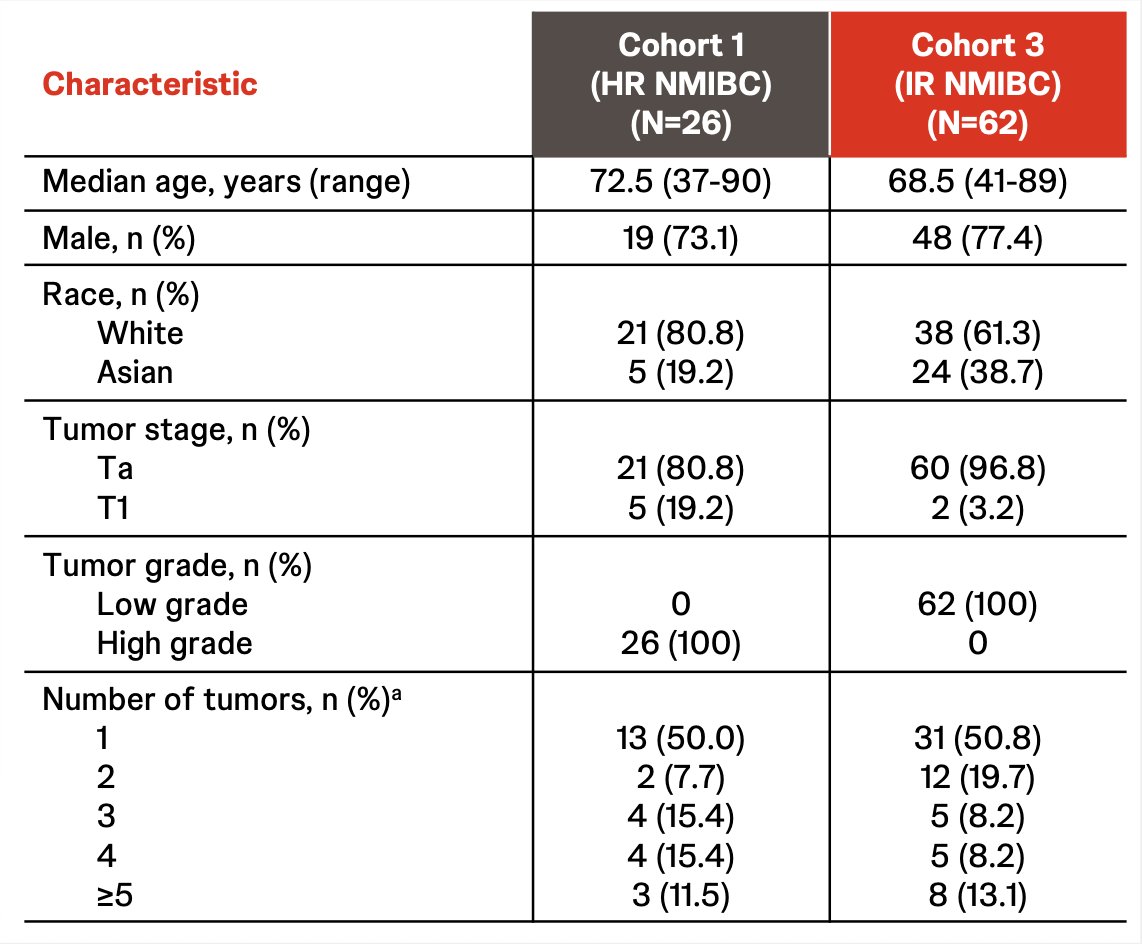
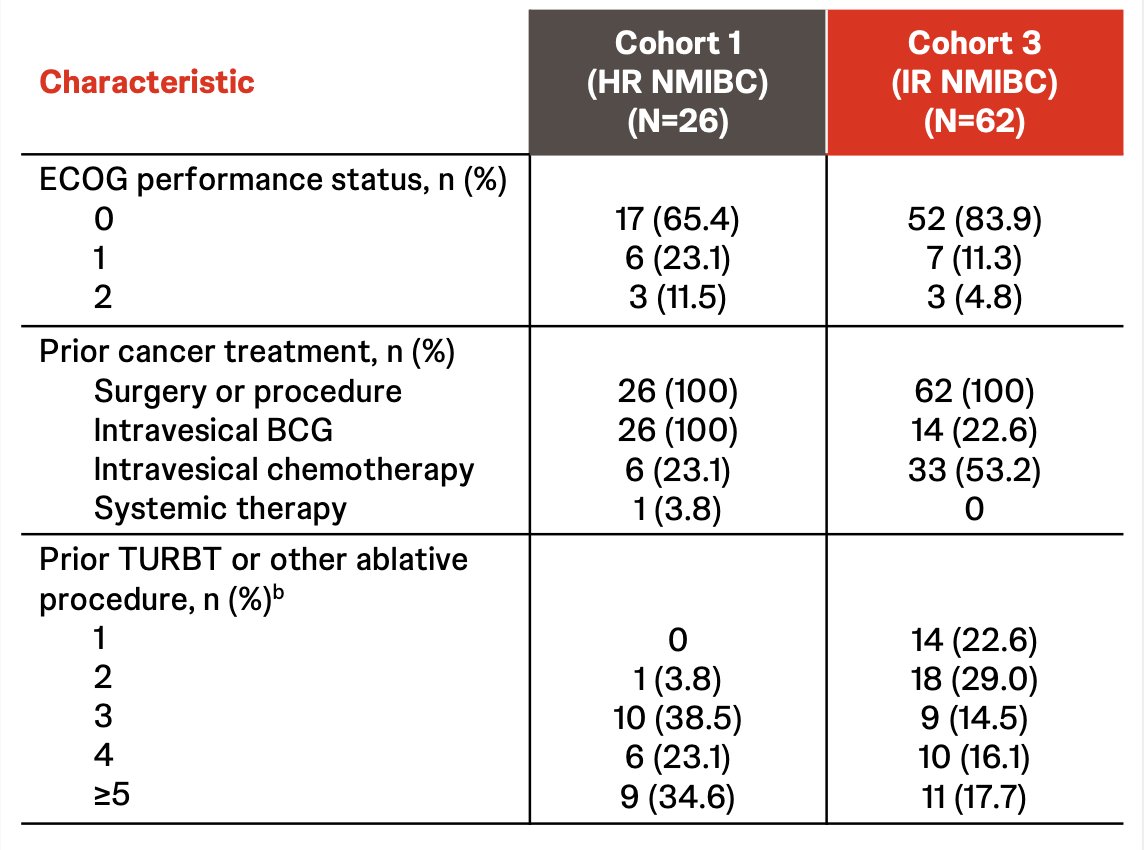
As of November 3, 2025, 26 patients in cohort 1 (median age 72.5 years; 73.1% male) and 62 in cohort 3 (median age 68.5 years; 77.4% male) received treatment:
The median treatment duration was 11.9 months (range 3-15) in cohort 1 and 11.8 months (range 0.1-15) in cohort 3. In cohort 1 and cohort 3, the most frequent treatment related adverse events were hematuria (32%) and dysuria (22%), of which 4 patients (5%) had grade ≥3 treatment related adverse events, 8 (9%) discontinued due to treatment related adverse events, and 2 (2%) had serious treatment related adverse events (1 with pyelonephritis/sepsis; 1 with hematuria):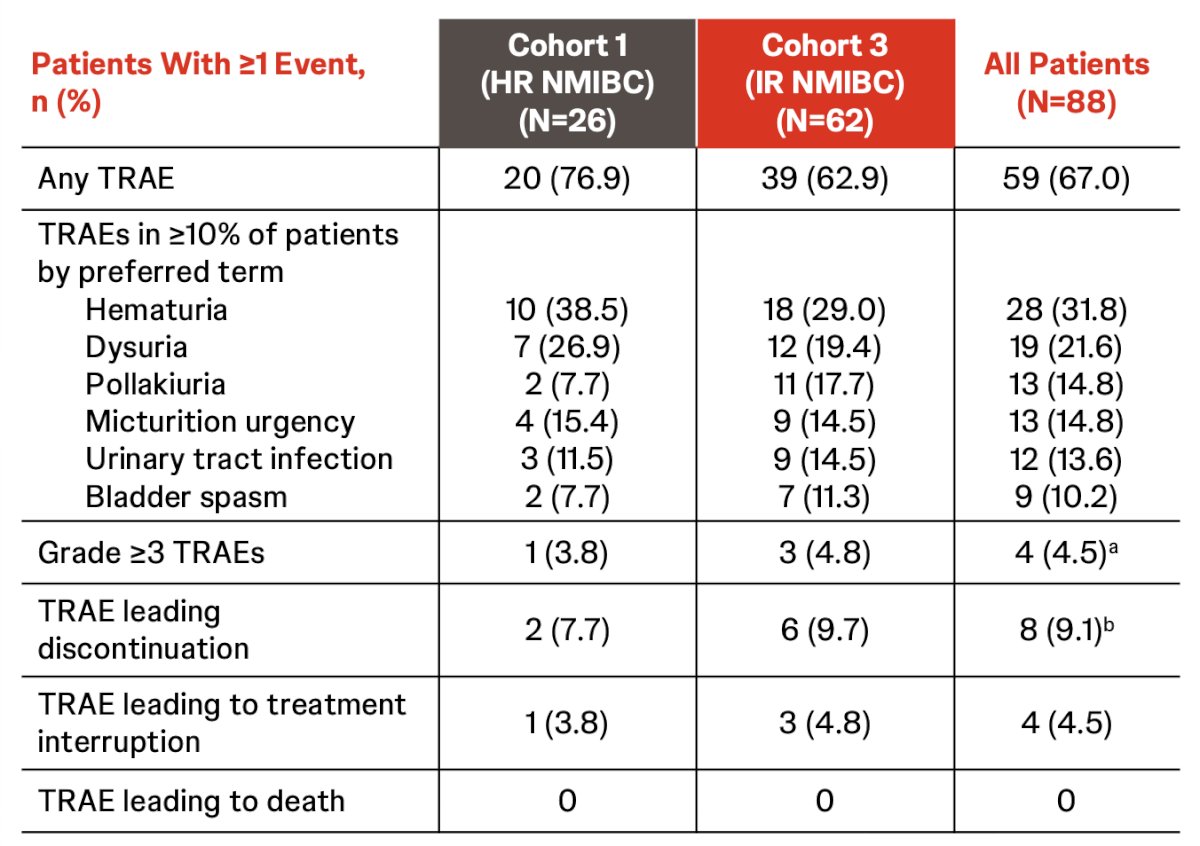
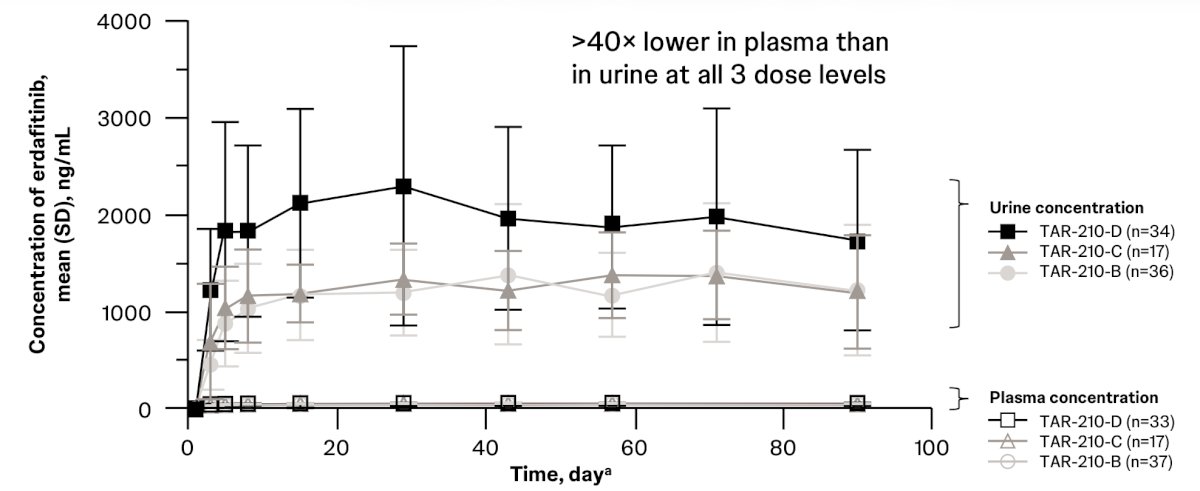
Plasma concentrations of erdafitinib delivered via the erdafitinib intravesical drug-releasing system were >40 times lower than those observed with oral erdafitinib at 9 mg daily:
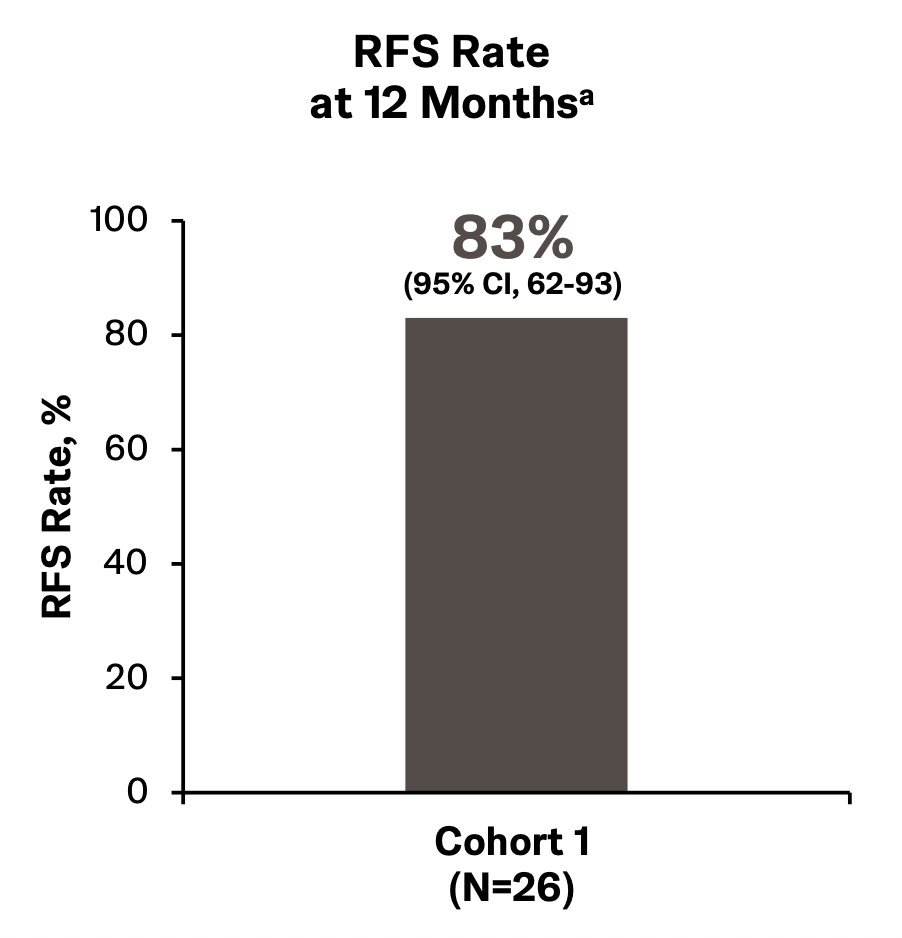
In cohort 1, median recurrence-free survival was 20 months (95% CI 15 - 30), and median recurrence-free survival follow-up was 24 months (range 15-30) (31% ongoing during follow-up). The 12-month recurrence-free survival rate was 83% (95% CI 62-93):
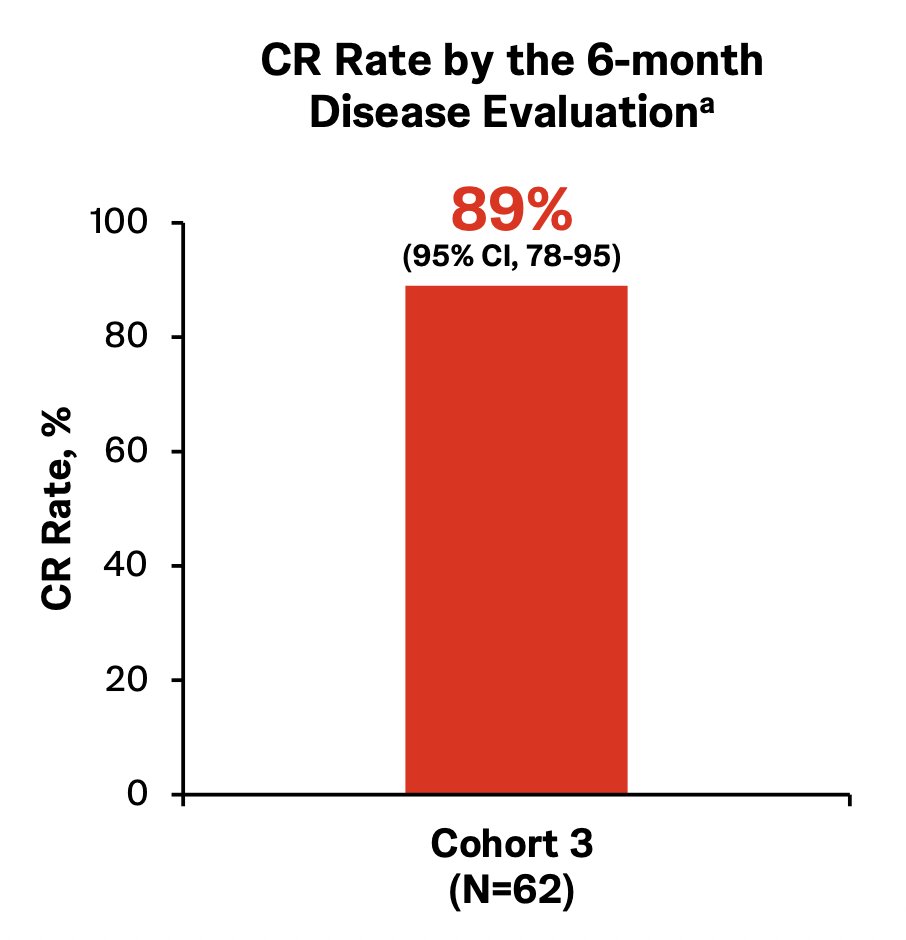
In cohort 3, at the first or second disease evaluation, the complete response rate was 89% (95% CI 78-95). Of note, 81% of patients had achieved a complete response at the 3-month disease evaluation:
Over a median follow-up in responders of 18.0 months (range 15-21), the median duration of complete response was 18.0 months (95% CI 14 - 25), with 49% of responders in ongoing follow-up and remaining in complete response at the clinical data cutoff.
Dr. Vilaseca concluded his presentation discussing the final analysis of the phase 1 first-in-human study of an erdafitinib intravesical drug-releasing system in patients with non-muscle invasive bladder cancer harboring select FGFR alterations with the following take-home points:
- Erdafitinib intravesical drug-releasing system achieved proof of concept for sustained local delivery of erdafitinib and demonstrated preliminary clinical activity in patients with FGFR-altered non-muscle invasive bladder cancer
- Erdafitinib intravesical drug-releasing system was tolerable, with mostly grade 1-2 lower urinary tract symptoms
- The estimated 12-month recurrence-free survival rate was 83%, adjuvant to TURBT in BCG-treated high-risk non-muscle invasive bladder cancer
- The estimated overall complete response rate was 89% with a median complete response duration of 18 months, as ablative therapy in intermediate risk non-muscle invasive bladder cancer
- Phase 2 and 3 trials of erdafitinib intravesical drug-releasing system are ongoing in patients with FGFR-altered non-muscle invasive bladder cancer
- Phase 3, adjuvant versus intravesical chemotherapy in intermediate risk non-muscle invasive bladder cancer (MoonRISe-1; NCT 06319820)
- Phase 2, ablative in intermediate risk non-muscle invasive bladder cancer (MoonRISe-2; NCT05316155)
- Phase 3, adjuvant versus intravesical chemotherapy in papillary-only high-risk non-muscle invasive bladder cancer (MoonRISe-3; NCT06919965)
Presented by: Antoni Vilaseca, MD, PhD, MSc, Hospital Clinic de Barcelona, Barcelona, Spain
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.