(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain was host to a thematic session of rapid-fire debates about common problems and controversies in bladder cancer. Drs. Arnulf Stenzl and Alison Birtle argued in favor of neoadjuvant and adjuvant approaches, respectively, for systemic therapy intensification in patients with high-grade upper tract urothelial carcinoma.
Dr. Morgan Rouprêt began the session with a case presentation of a 73-year-old male who presented with gross hematuria and was found to have bilateral (right > left) hydronephrosis. He underwent a bilateral flexible ureteroscopy with the following findings:
- Left ureteroscopy:
- 1.5 cm renal pelvis tumor
- Biopsy LG Ta
- Laser ablated
- Right ureteroscopy:
- Large, multifocal renal pelvis tumor
- Biopsy HG Ta
- ~40% of tumor laser ablated
Staging scans did not demonstrate evidence of nodal enlargement. Following tumor board discussions, he was recommended for a radical nephroureterectomy (RNU). Should he receive neoadjuvant therapy, or should adjuvant therapy be reserved in case of high-risk pathologic features?
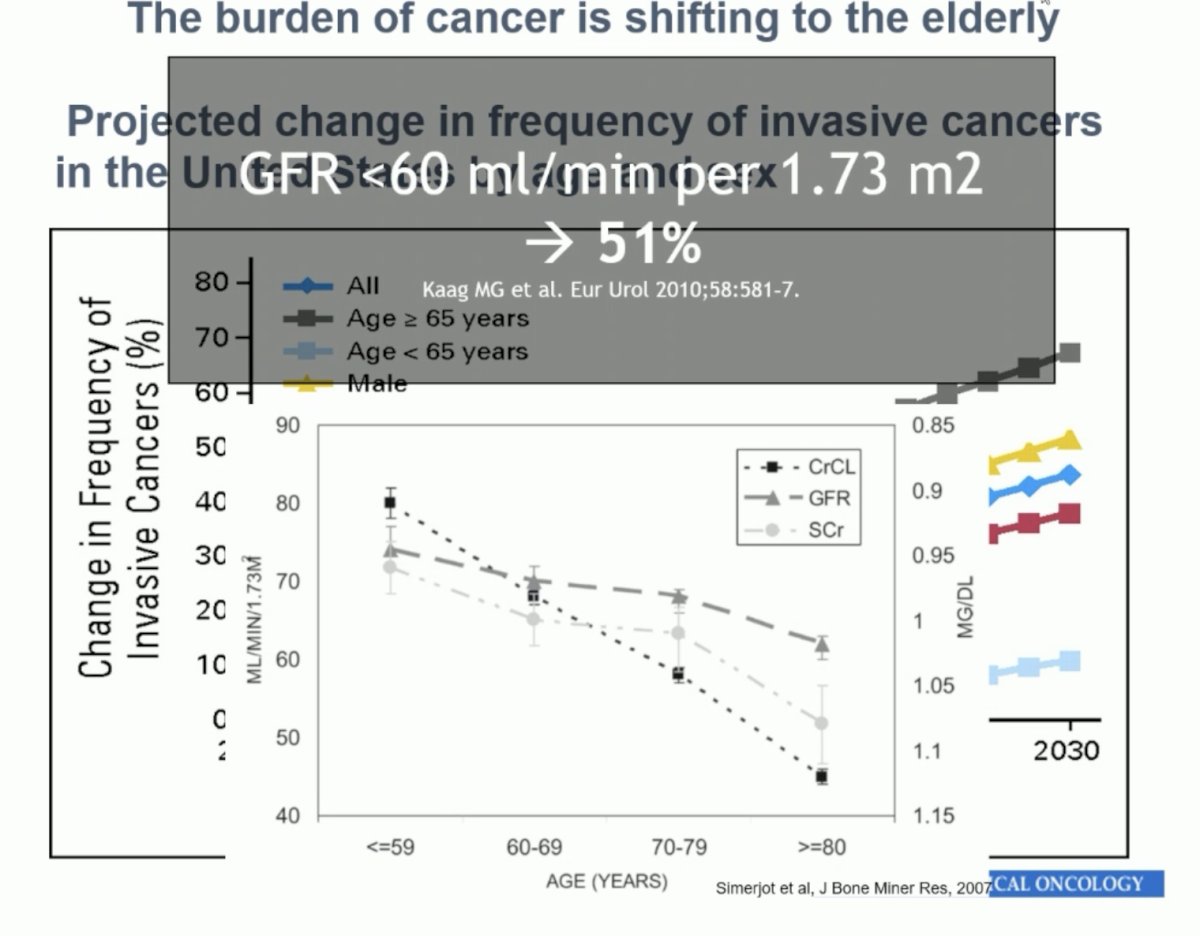
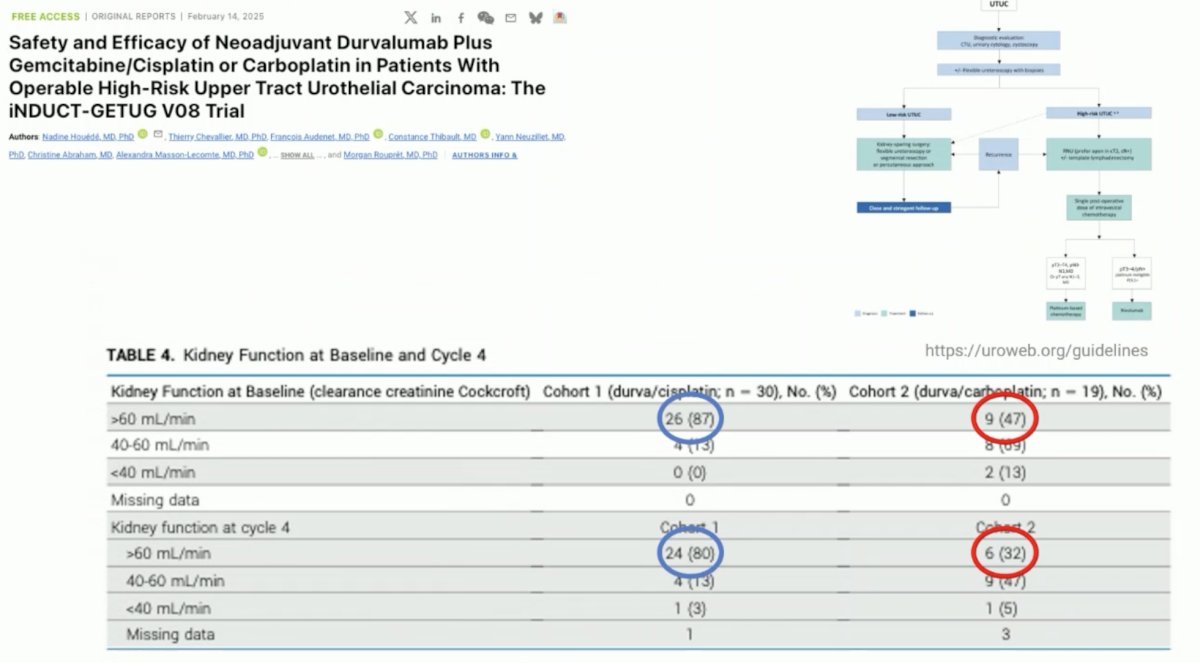
Dr. Stenzl began his argument in favor of neoadjuvant therapy by noting that the burden of bladder cancer is increasing worldwide, particularly in elderly patients, many of whom have compromised renal function that may prohibit the administration of cisplatin combination chemotherapy. This is particularly significant in the post-RNU setting as eGFR is expected to decrease further, thus supporting the use of ‘early’ systemic therapy while patients’ eGFR is at its highest.
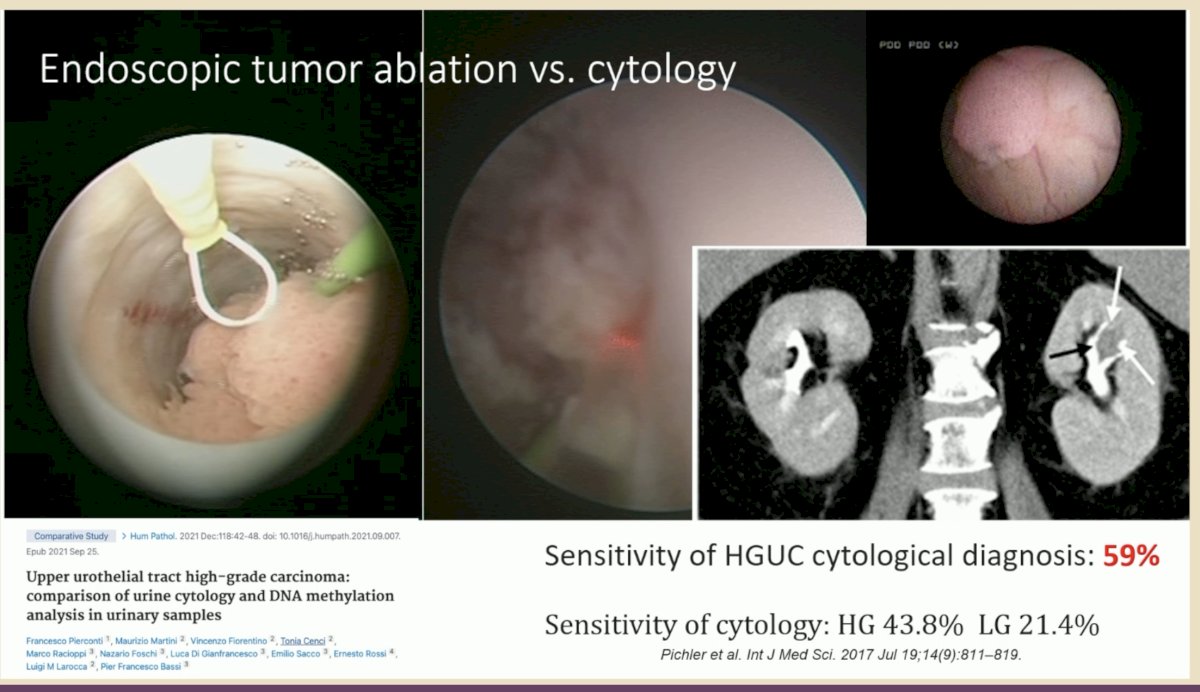
Another reason to consider neoadjuvant, as opposed to adjuvant, therapy is the fact that current staging/grading tools are inaccurate. The sensitivity of selective upper tract urine cytology for detecting high-grade disease is roughly 60%, meaning that up to 40% of patients with high-grade disease have negative urine cytologies.
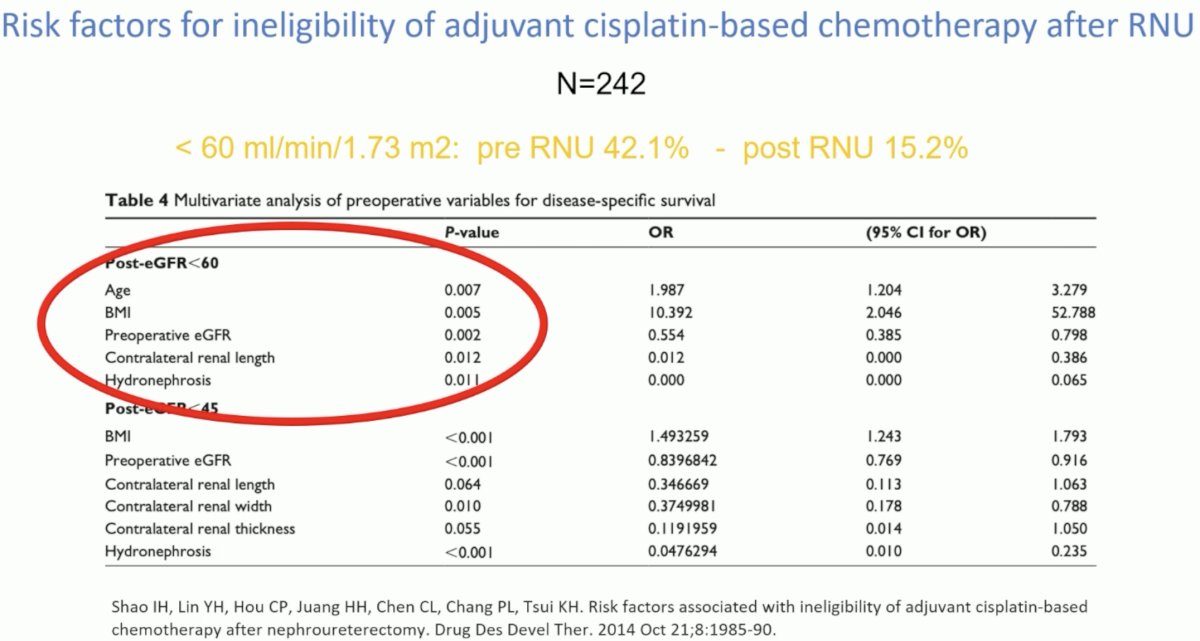
It is also important to consider factors that may predict ineligibility for adjuvant cisplatin-based chemotherapy after RNU. Older patients, those with a higher BMI, lower pre-operative eGFR, and hydronephrosis are at higher risk of compromised post-RNU eGFR and thus should be strongly considered for neoadjuvant therapy, if they have high-risk features.
In 2023, Coleman et al. published the results of a phase II trial of neoadjuvant split-dose Gem-Cis (x4 cycles) for patients with high-risk, localized upper tract urothelial carcinoma. Among 57 patients evaluated, 36 (63%) demonstrated pathologic responses. A complete pathologic response (ypT0N0) was noted in 11 patients (19%). Fifty-one patients (89%) tolerated at least three complete cycles of split-dose Gem-Cis, 27 patients (47%) tolerated four complete cycles, and all patients proceeded to surgery. With a median follow up of 3.1 years, the 2- and 5-year progression-free survival rates were 89% and 72%, while the 2- and 5-year overall survival rates were 93% and 79%, respectively.1

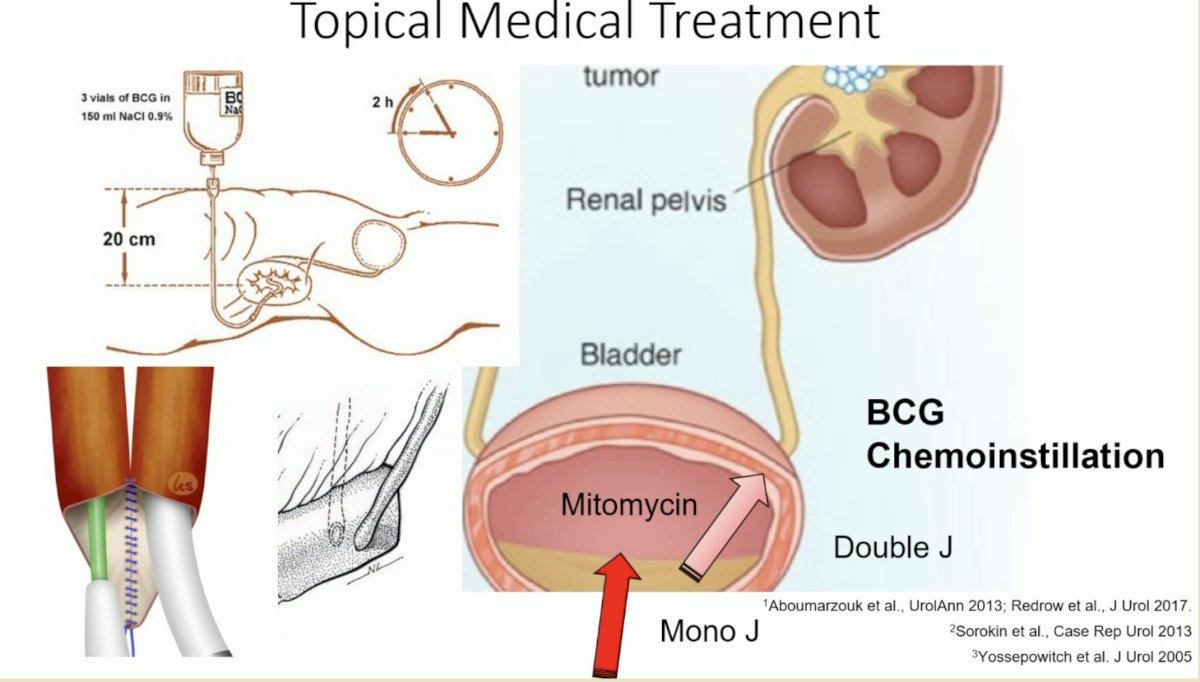
Dr. Stenzl noted that neoadjuvant therapy should not be limited to systemic therapy. Other neoadjuvant options include mitomycin and BCG, which when instilled intravesically can reflux up the collecting system with a stent is in place, and JELMYTO. These neoadjuvant options can be considered in select cases, including those with bilateral upper tract disease.
Another important question is: how do you monitor treatment response in patients receiving adjuvant therapy? In the neoadjuvant setting, we can use tools such as MRI and CT, endoscopic evaluation, and cytology. Dr. Stenzl argued that in the adjuvant setting, options are much more limited.
Another important potential benefit of neoadjuvant therapy is that pathologic complete responders may potentially forgo a RNU in the future. While currently available tools for assessment of complete clinical responses remain suboptimal in the upper tract setting, as the accuracy of these tools improve and we can more reliably identify those patients with a pathologic complete response to neoadjuvant therapy, perhaps RNU can be avoided in select patients.
Dr. Stenzl concluded his argument in favor of neoadjuvant therapy as follows:
- More patients are eligible for neoadjuvant versus adjuvant therapy due to renal function declines following RNU
- Patients receiving neoadjuvant therapy may achieve a ypT0 status
- Topical medical treatment may be considered as part of the neoadjuvant armamentarium
- Monitoring of treatment response to systemic therapy is difficult in the adjuvant setting
- An emerging paradigm with pre-operative cisplatin-based chemotherapy and post-operative immunotherapy may be emerging
Next, Dr. Birtle argued for adjuvant chemotherapy for the patient in the case presentation. She emphasized that an eGFR of 60 ml/min is no longer considered the lower limit for recommending cisplatin chemotherapy and that many patients with an eGFR of 45 ml/min can tolerate cisplatin. Additionally, she highlighted a recent meta-analysis of 4 studies that reported no change in pre- and post-RNU eGFR levels.2

But do we ‘know enough’ from pre-operative clinical data to recommend neoadjuvant chemotherapy ‘blindly’ to high-risk UTUC patients? High-grade disease on biopsy predicts muscle invasiveness in only 60–68% of cases. Other available clinical models predict invasiveness with only 70–90% accuracy. This means that a significant proportion of patients may be overtreated with neoadjuvant therapy. This is highlighted by the fact that patients with pT1 disease have a 5-year disease-specific survival of 92% without neoadjuvant therapy.

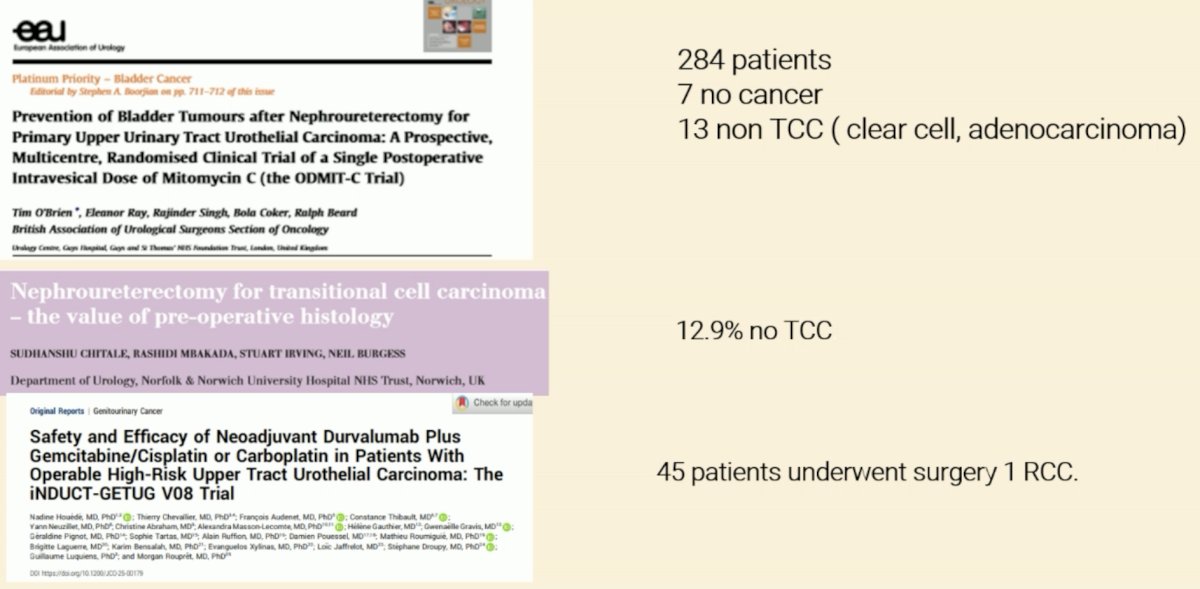
Another important factor to consider is that some patients with reported UTUC may not actually have urothelial carcinoma, and, thus, would be receiving ineffective systemic therapy for their underlying disease. As demonstrated in the studies below, among 284 patients who underwent an RNU, 7 did not have any malignancy and 13 had non-urothelial carcinomas (e.g., clear cell RCC, adenocarcinoma). While these incidents remain uncommon, it is important to be aware of the possibility of such events.
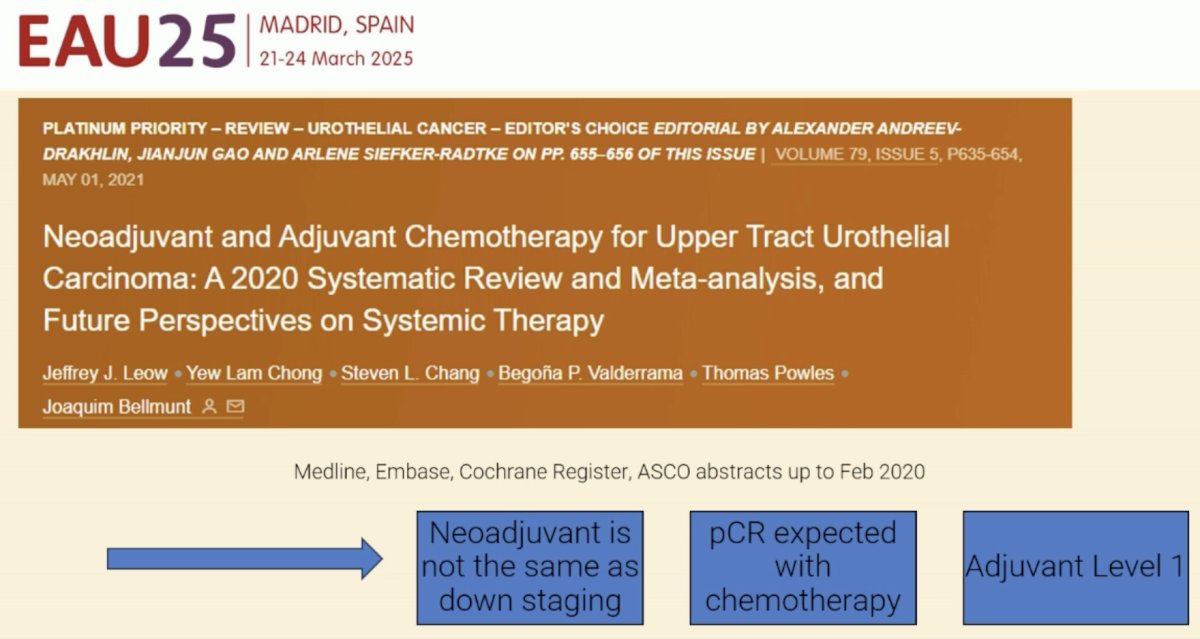
Another important consideration is how many of the observed pathologic responses are secondary to true downstaging with neoadjuvant therapy? Pre-operative clinical assessment tools perform poorly for accurately staging UTUC patients. As such, the observed pathologic responses may reflect underlying disease stage and not the downstaging effects of systemic therapy.
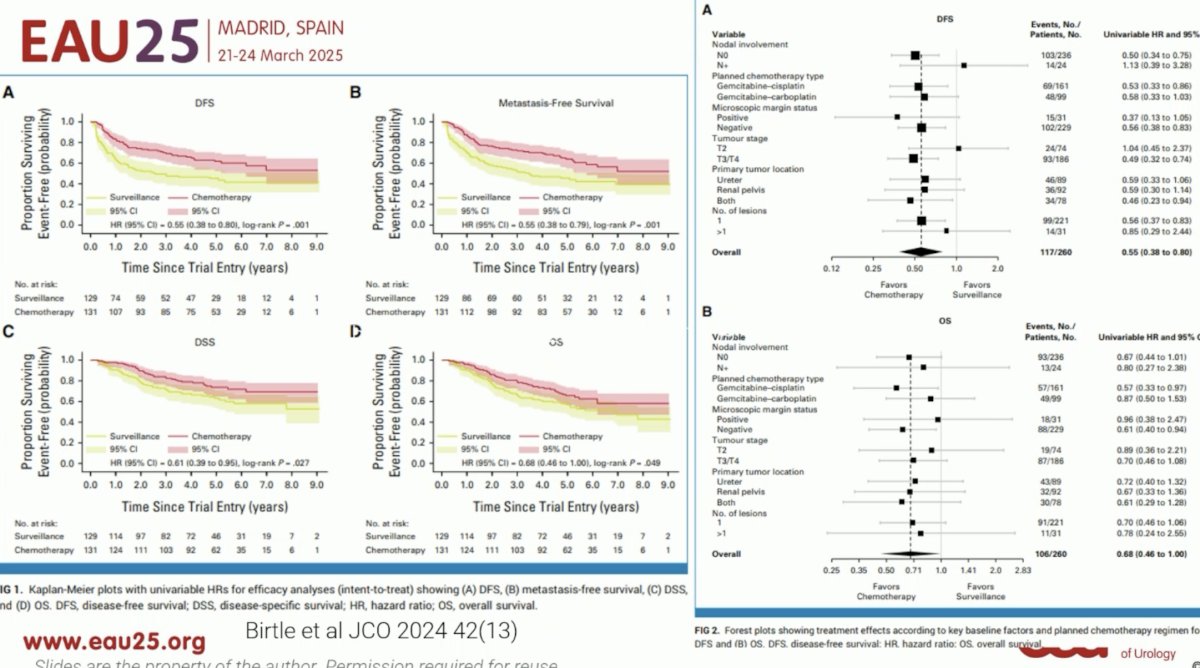
Ultimately, the only level one evidence for systemic therapy is in the adjuvant setting. POUT was a phase III, randomized, open-label trial, including 261 patients with muscle-invasive or lymph node-positive, nonmetastatic upper tract urothelial cancer (UTUC) randomly assigned after radical nephroureterectomy to platinum-based chemotherapy (n=132) or surveillance (n=129). At a median follow-up of 65 months, the 5-year DFS was 62% versus 45%. The restricted mean survival time (RMST) was 18 months longer in the chemotherapy arm. The 5-year OS was 66% versus 57%, with an RMST difference 11 months. Benefits were observed in all evaluable subgroups.3
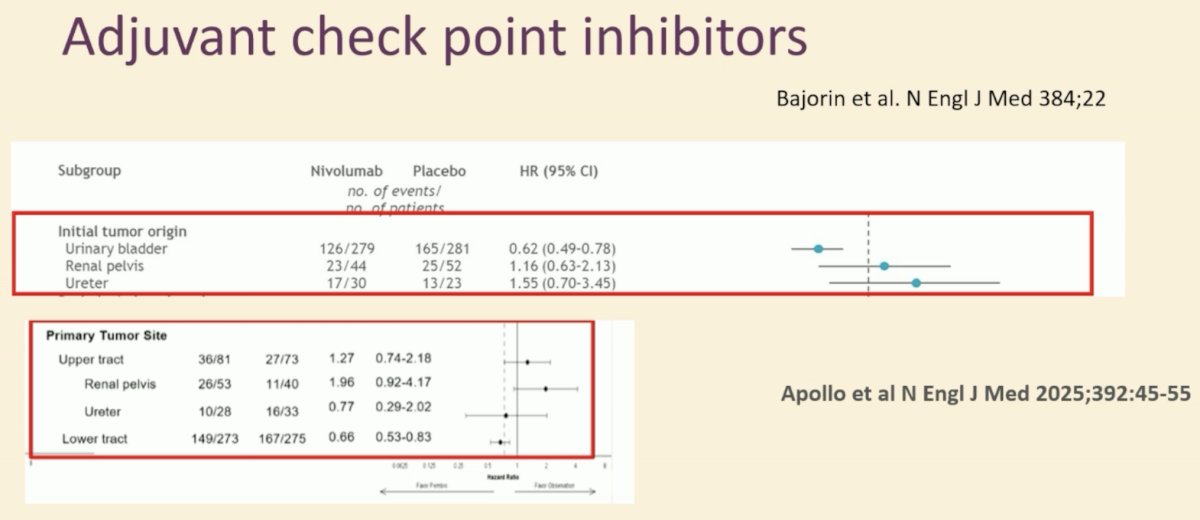
What about adjuvant checkpoint inhibitors? Subgroup analyses from all trials of adjuvant immunotherapy have consistently demonstrated no benefit to adjuvant immunotherapy.4
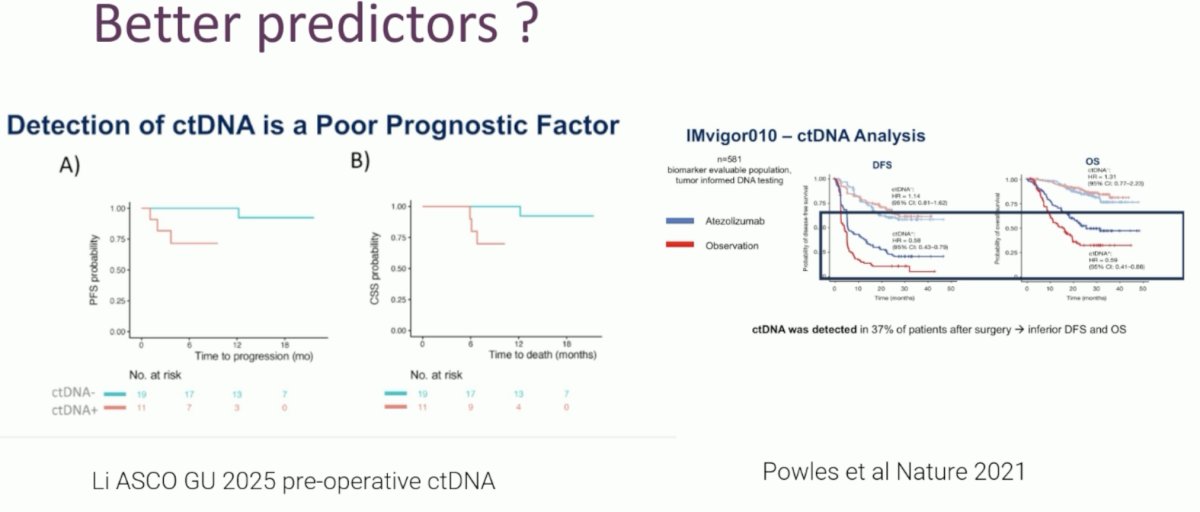
Ultimately, a more nuanced approach to adjuvant therapy is needed for UTUC patient post-RNU, with emerging tools such as ctDNA likely to be incorporated in this setting.
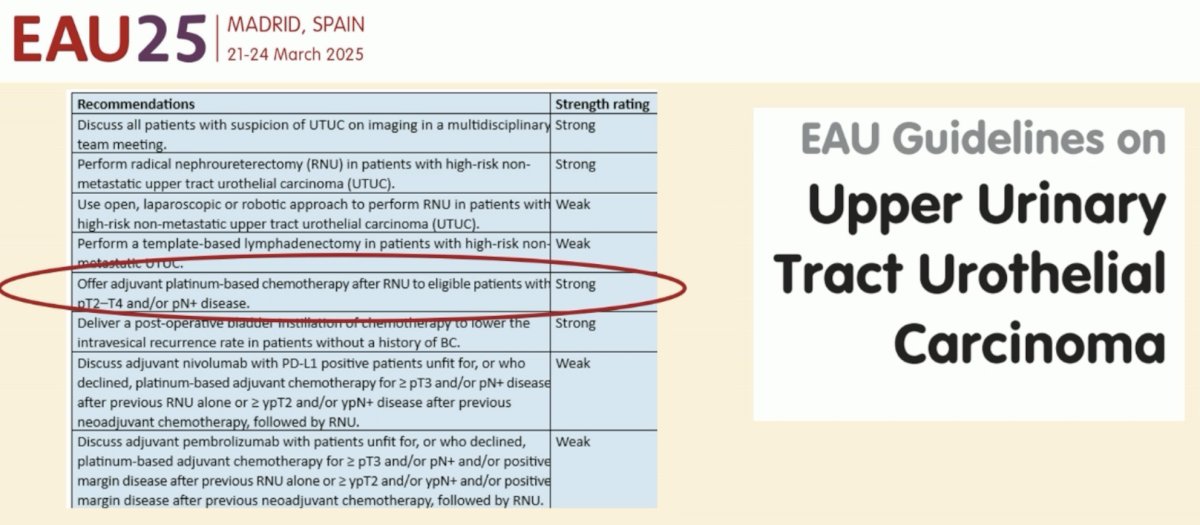
Dr. Birtle concluded by emphasizing that we should ‘simply follow the guidelines’ and only offer adjuvant therapy to RNU patients.
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
Related content: Adjuvant vs Neoadjuvant Chemotherapy Debate for Upper Tract Urothelial Carcinoma - Morgan Rouprêt & Alison Birtle
References:
- Coleman JA, Yip W, Wong NC, et al. Multicenter Phase II Clinical Trial of Gemcitabine and Cisplatin as Neoadjuvant Chemotherapy for Patients With High-Grade Upper Tract Urothelial Carcinoma. J Clin Oncol. 2023; 41(8): 1618-25.
- Deb AA, Chitteti P, Naushad N, et al. Role of Neoadjuvant Chemotherapy on Pathological, Functional, and Survival Outcomes of Upper Tract Urothelial Carcinoma Patients: A Systematic Review and Meta-Analysis. Urol Res Pract. 2024; 50(1): 13-24.
- Birtle AJ, Jones R, Chester J, et al. Improved Disease-Free Survival With Adjuvant Chemotherapy After Nephroureterectomy for Upper Tract Urothelial Cancer: Final Results of the POUT Trial. J Clin Oncol. 2024; 42(13): 1466-71.
- Sayyid RK, Bernardino R, Chavarriaga J, et al. Adjuvant immune checkpoint inhibitors for urothelial carcinoma: systematic review and Meta-analysis. World J Urol. 2024; 42(1): 418.