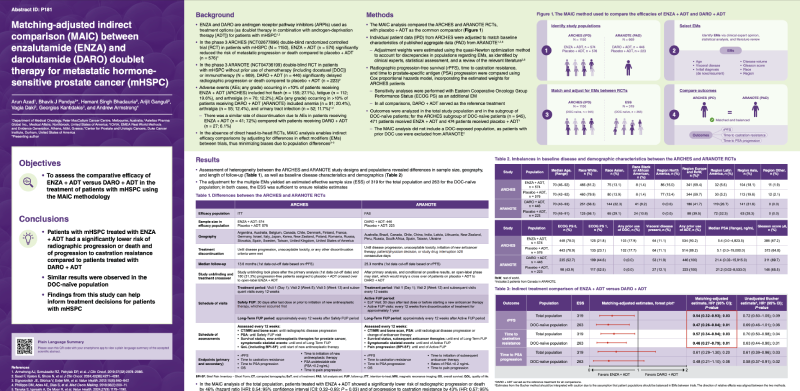
(UroToday.com) The 2025 EAU annual meeting featured a prostate cancer session and a presentation by Dr. Bhavik Pandya discussing a matching-adjusted indirect comparison between enzalutamide and darolutamide doublet therapy for metastatic hormone sensitive prostate cancer (mHSPC). Enzalutamide and darolutamide are androgen receptor pathway inhibitors used as treatment options (as doublet therapy in combination with ADT) for patients with mHSPC. In the phase 3 ARCHES double blind randomized controlled trial in patients with mHSPC, enzalutamide + ADT significantly reduced the risk of metastatic progression or death compared to placebo + ADT.1 In the phase 3 ARANOTE double blind randomized controlled trial in patients with mHSPC without prior use of chemotherapy (including docetaxel) or immunotherapy, darolutamide + ADT significantly delayed radiographic progression or death compared to placebo + ADT. Adverse events occurring in >10% of patients receiving enzalutamide + ADT in ARCHES included hot flashes (27.1%), fatigue (19.6%), and arthralgia (12.2%). Adverse events occurring in >10% of patients receiving darolutamide + ADT in ARANOTE included anemia (20.4%), arthralgia (12.4%), and urinary tract infection (11.7%). Of note, there was a similar rate of discontinuation due to adverse events in patients receiving enzalutamide + ADT (7.2%) compared with patients receiving darolutamide + ADT (6.1%).
There is a lack of direct evidence from randomized controlled trials comparing the outcomes of enzalutamide and darolutamide when added to ADT (enzalutamide/darolutamide doublet) in the mHSPC setting. In absence of direct head-to-head randomized controlled trials, matching-adjusted indirect comparisons enable indirect efficacy comparisons by adjusting for differences in effect modifiers between trials, thus minimizing biases due to population differences. This study presented at the EAU 2025 annual meeting assessed the relative efficacy of enzalutamide versus darolutamide doublet using matching-adjusted indirect comparison in patients with mHSPC.
The matching-adjusted indirect comparison analysis compared ARCHES and ARANOTE randomized controlled trials, with placebo + ADT as the common comparator:

Individual patient data from the ARCHES randomized controlled trial were adjusted to match baseline characteristics of the ARANOTE2 randomized controlled trial. Adjustment weights were estimated using the quasi-Newton optimization method to account for discrepancies in populations for the following effect modifiers as identified by clinical experts, statistical assessment, and review of the relevant literature: age, visceral disease, initial diagnosis (de novo/recurrent), disease volume, Gleason score, race, and region. Radiographic progression-free survival, time to castration-resistance, and time to PSA progression were compared using Cox proportional hazards model, incorporating the estimated weights for ARCHES patients. Sensitivity analyses were performed with ECOG performance status as an additional effect modifier. Outcomes were analyzed in the total study population and in the subgroup of docetaxel-naïve patients. For the ARCHES subgroup of docetaxel-naïve patients (n = 945), 471 patients received enzalutamide + ADT and 474 patients received placebo + ADT.
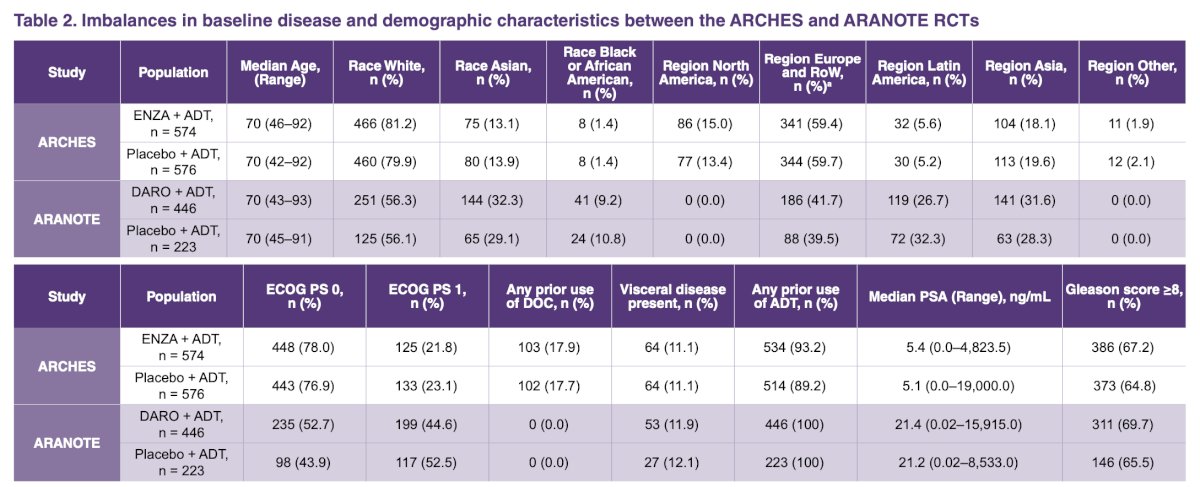
Assessment of heterogeneity between the ARCHES and ARANOTE study designs and populations revealed differences in sample size, geography, and length of follow-up:

There were also differences in baseline disease characteristics and demographics:
The adjustment for multiple effect modifiers yielded an estimated effective sample size of 319 for the total population and 263 for docetaxel-naïve population. In both cases, the effective sample size was sufficient to ensure reliable estimates. In the matching-adjusted indirect comparisons analysis of the total population, patients treated with enzalutamide + ADT showed a significantly lower risk of radiographic progression by 46% (HR 0.54, 95% CI 0.32–0.93; p = 0.03) and of progression to castration-resistance by 43% (HR 0.57, 95|% CI 0.34–0.94; p = 0.03) than those receiving darolutamide + ADT:

Similar results were observed in the docetaxel-naïve population: compared to darolutamide + ADT, patients treated with enzalutamide + ADT had a significantly lower risk of radiographic progression or death by 53% (HR 0.47, 95% CI 0.26-0.84; p = 0.01) and of progression to castration resistance by 54% (HR 0.46, 95% CI 0.27-0.79, p = 0.01). Time to PSA progression for enzalutamide + ADT was similar to darolutamide + ADT in both the total population (HR 0.61, 95% CI 0.29-1.30, p = 0.20) and the docetaxel-naïve population (HR 0.48, 95% CI 0.21-1.10; p = 0.08). In sensitivity analyses, the comparative effectiveness of enzalutamide + ADT and darolutamide + ADT remained similar in direction and significance for all outcomes, however adjusting for ECOG performance status yielded a reduction in estimated effective sample (n = 196).
There are several limitations associated with this analysis:
- Some sources of bias could not be fully addressed in matching-adjusted indirect comparison analysis (ie. length of follow-up and clinical heterogeneity), and any imbalances in covariates not adjusted for in the analysis were assumed to not impose considerable biases in the estimated relative treatment effects
- Adjustment of some effect modifiers that lacked overlap between ARCHES and ARANOTE, such as region and race, substantially reduced the estimated effective sample. However, these adjustments were crucial for obtaining reliable matching-adjusted indirect comparison estimates
- Data immaturity for both trials, and the lack of information on the method underlying the median follow-up estimate in ARANOTE, do not allow a definite conclusion regarding the potential impact of these considerations in the matching-adjusted indirect comparison estimates
- This analysis does not consider how safety may affect provider prescription decisions
Dr. Pandya concluded his presentation by discussing a matching-adjusted indirect comparison between enzalutamide and darolutamide doublet therapy for mHSPC with the following take home points:
- Patients with mHSPC treated with enzalutamide + ADT had a significantly lower risk of radiographic progression or death and progression to castration resistance compared to patients treated with darolutamide + ADT
- Similar results were observed in the docetaxel-naïve population
- Findings from this study can help inform treatment decisions for patients with mHSPC
Click to Enlarge
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Armstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy with Enzalutamide or Placebo in Men with Metastatic Hormone-Sensitive Prostate Cancer. J Clin Oncol. 2019 Nov 10;37(32):2974-2986.
- Saad F, Vjaters E, Shore N, et al. Darolutamide in Combination with Androgen-Deprivation Therapy in Patients with Metastatic Hormone-Sensitive Prostate Cancer From the Phase III ARANOTE Trial. J Clin Oncol. 2024 Dec 20;42(36):4271-4281.