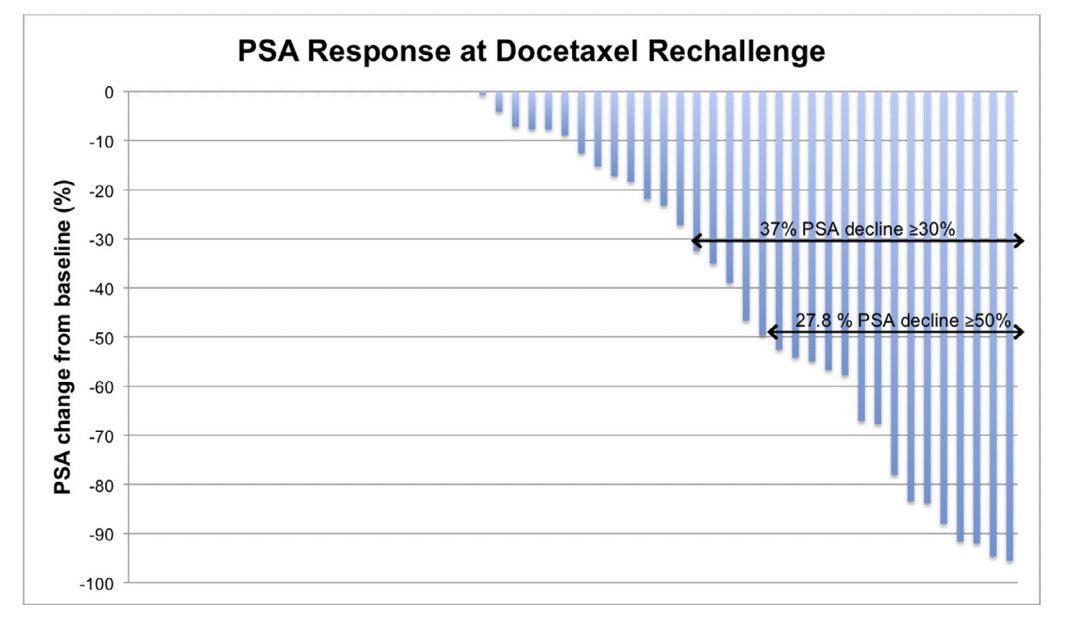
(UroToday.com) The 2025 EAU annual meeting featured a session on managing metastatic castration resistant prostate cancer (mCRPC) after triplet therapy for metastatic hormone sensitive prostate cancer (mHSPC) and a presentation by Dr. Jan Oldenburg discussing the evidence for and against a second taxane. Dr. Oldenburg started his presentation by noting that androgen receptor pathway inhibitor induced resistance can be overcome by taxanes. To discuss docetaxel rechallenge, Dr. Oldenburg highlighted a retrospective analysis of men treated with docetaxel for mHSPC and then rechallenged in the mCRPC setting from four cancer centers in Ontario, Canada. Among 54 evaluable patients, 27.8% had a PSA decline ≥50%, median progression free survival was 4.1 months (95% CI, 2.1-4.8) and median overall survival from ADT initiation was 38.3 months (95% CI, 32.9-41.0). The following is a waterfall plot from this study showing PSA response at docetaxel rechallenge:
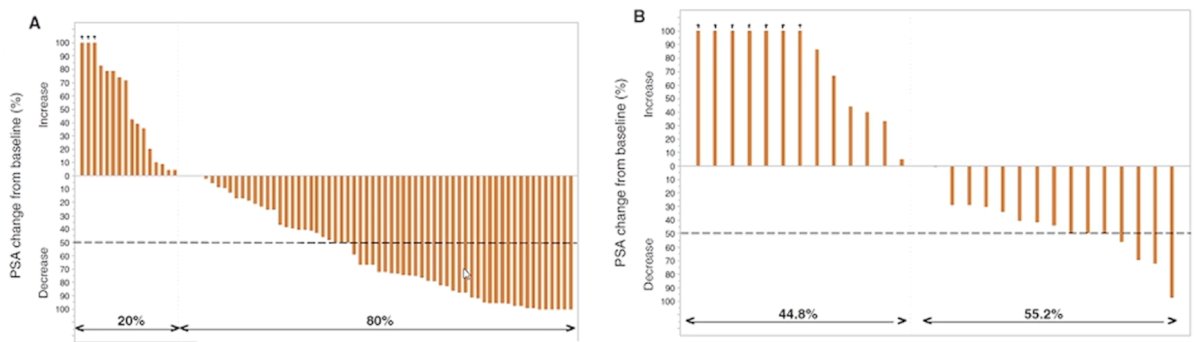
In the GETUG-AFU 15 trial,2 PSA50 response was 38% (25/66; 95% CI 26-51) for upfront ADT alone, and 20% (4/20; 95% CI 6-44) for upfront ADT + docetaxel.
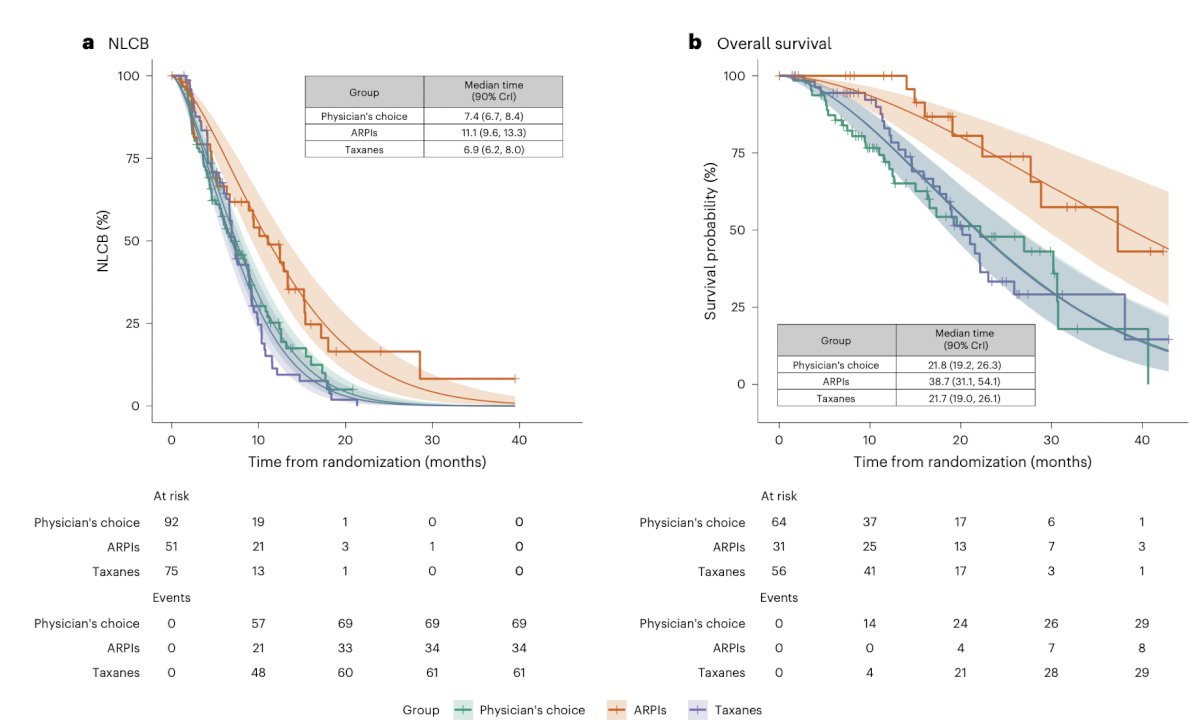
Next, Dr. Oldenburg discussed the ProBio trial, an outcome adaptive and randomized multi-arm biomarker drive study in mCRPC patients.3 Prospective circulating tumor DNA and germline DNA analysis was performed in patients with mCRPC before randomization to androgen receptor pathway inhibitors, taxanes, or a physician's choice control arm. The primary endpoint was the time to no longer clinically benefit:

The survival time ratio for the time to no longer clinically benefitting from androgen receptor pathway inhibitors was 1.50 (90% credible intervals (CrI) 1.20, 1.86) compared to the physician’s choice (median 11.1 versus 7.4 months) and 1.60 (90% CrI 1.28, 2.01) compared to taxanes (median 11.1 versus 6.9 months). The survival time ratio for the time to no longer clinically benefit from taxanes was 0.94 (90% CrI 0.78, 1.12) compared to the physician’s choice (median 6.0 versus 7.4 months). The survival time ratio for overall survival in the biomarker-unselected ‘all’ patients group was 1.77 (90% CrI 1.29, 2.51) for androgen receptor pathway inhibitors compared to physician’s choice (median 38.7 versus 21.8 months) and 1.78 (90% CrI 1.28, 2.61) compared to the taxane arm (median 38.7 versus median 21.7 months):
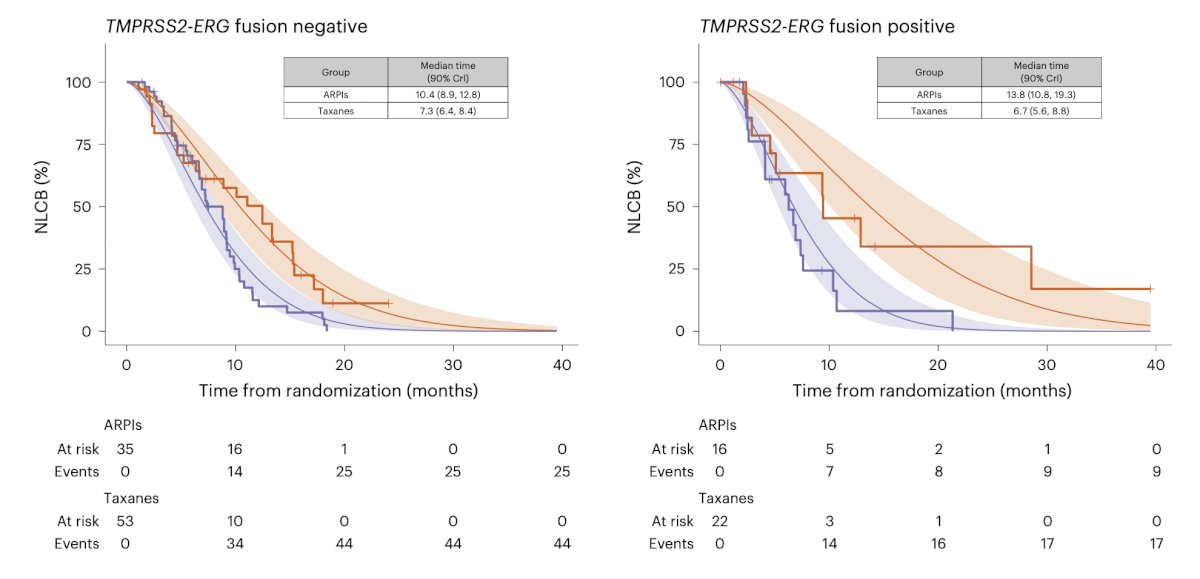
The ProBio trial also showed that for TMPRSS2-ERG fusion as a biomarker, there was no benefit to taxane chemotherapy, which according to Dr. Oldenburg is an argument against taxanes:
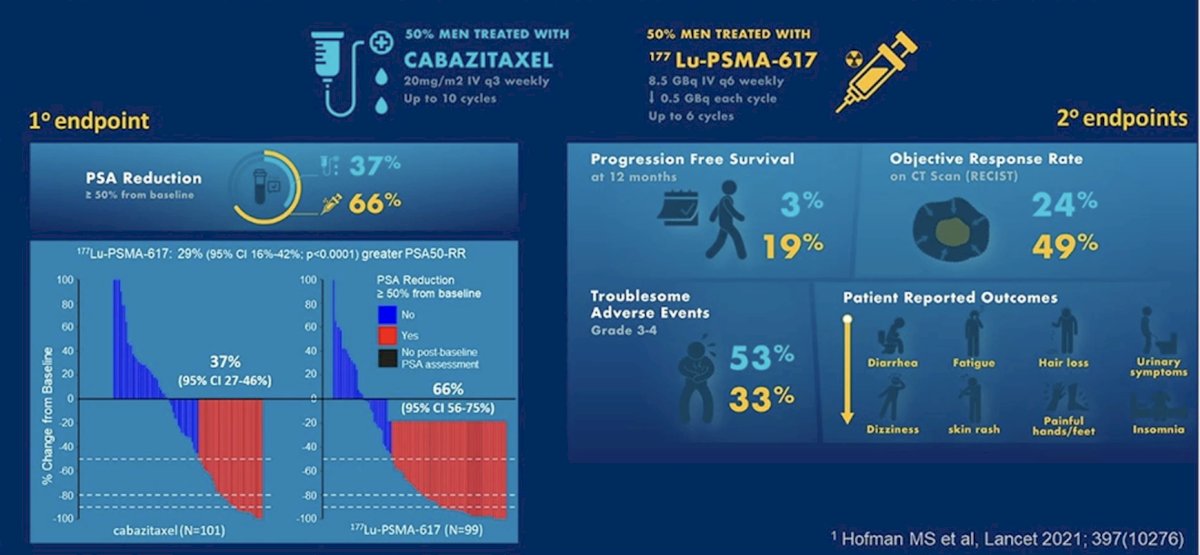
Dr. Oldenburg then discussed the TheraP trial,4 which was the first randomized study to evaluate 177Lu-PSMA-617 vs cabazitaxel for men with mCRPC after docetaxel. In this open label, phase II trial, 200 men were randomized to either 177Lu-PSMA-617 or cabazitaxel. Overall, 200 patients were randomized 1:1 to 177Lu-PSMA-617 6-8 GBq every 6 weeks for up to 6 cycles of therapy or cabazitaxel 20 mg/m2 every 3 weeks for up to 10 cycles. The primary endpoint of this study was a PSA50 response and secondary endpoints included PSA-PFS and overall. After a median follow up of 13 months, 177Lu-PSMA-617 significantly improved PSA-PFS compared with cabazitaxel (HR 0.63, 95% CI 0.46 to 0.86) and a had a much higher PSA50 rate (66% vs 37%):
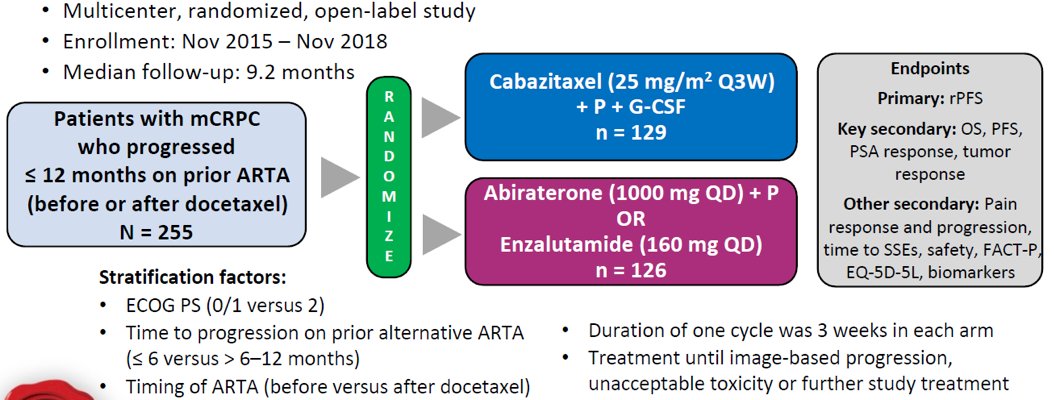
The CARD trial5 was a third-line mCRPC therapy trial. In CARD, patients who had previously received docetaxel and an androgen-signaling-targeted inhibitor (abiraterone or enzalutamide) were randomly assigned, in a 1:1 ratio, to either cabazitaxel or the other androgen-signaling-targeted inhibitor (either 1000 mg of abiraterone plus prednisone daily or 160 mg of enzalutamide daily). The primary endpoint was imaging-based progression-free survival, and a key secondary endpoint was survival:
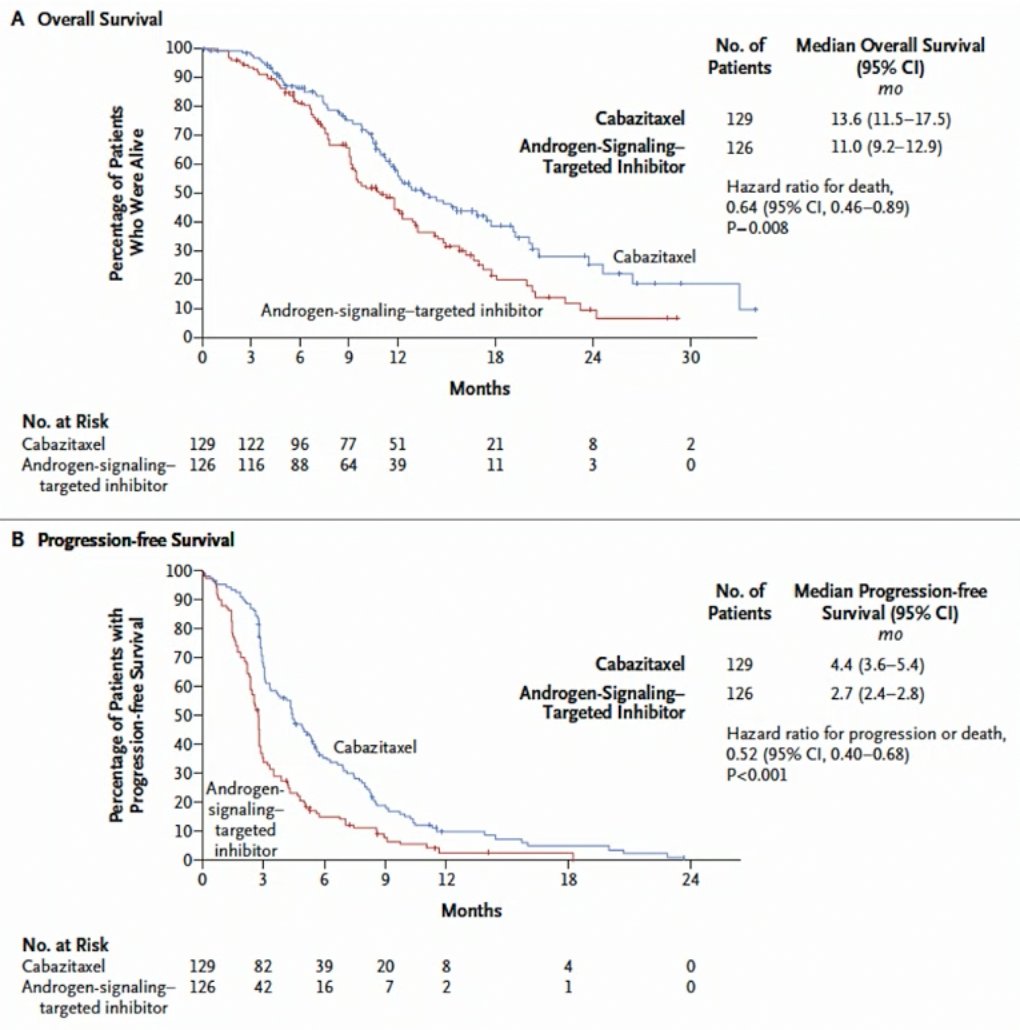
Among 255 patients, over a median follow-up of 9.2 months, imaging-based progression or death was reported in 95 of 129 patients (73.6%) in the cabazitaxel group, as compared with 101 of 126 patients (80.2%) in the group that received an androgen-signaling-targeted inhibitor (HR 0.54, 95% CI 0.40 to 0.73). The median progression-free survival was 4.4 months with cabazitaxel and 2.7 months with an androgen-signaling-targeted inhibitor (HR for progression or death, 0.52; 95% CI, 0.40 to 0.68). The median overall survival was 13.6 months with cabazitaxel and 11.0 months with the androgen-signaling-targeted inhibitor (HR 0.64, 95% CI 0.46 to 0.89):
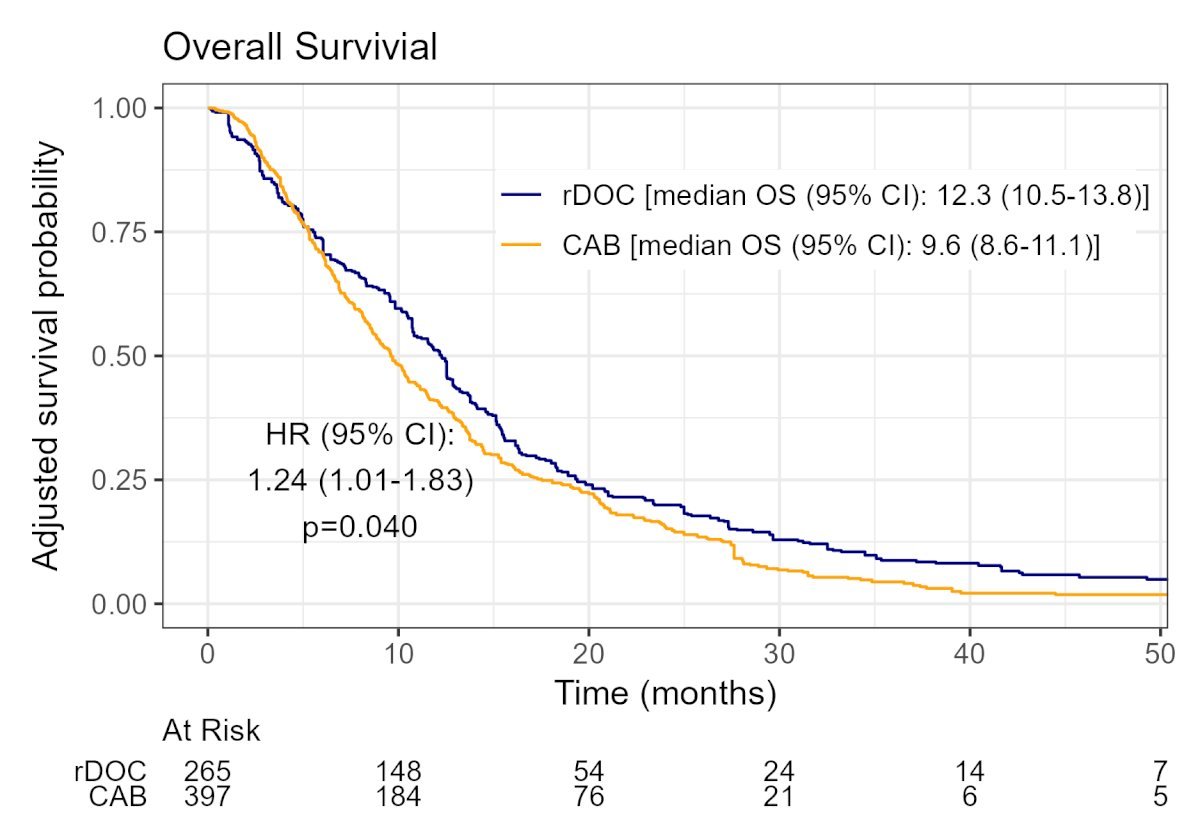
Dr. Oldenburg cautioned that what we do not know based on the CARD trial is whether cabazitaxel is superior to docetaxel after docetaxel chemotherapy since there has not been a head to head comparison. Finally, at ASCO GU 2025, Dr. Barata presented results of docetaxel rechallenge versus cabazitaxel in patients treated with docetaxel for mCRPC. This study included a total of 262 patients who received a docetaxel re-challenge and 407 who underwent a cabazitaxel switch. The median patient age was 72 years (IQR: 67–77). As illustrated in the weighted Kaplan-Meier curve below, patients who received a docetaxel re-challenge had superior overall survival outcomes (median: 12.3 versus 9.6 months; HR 1.24, 95% CI 1.01–1.83, p = 0.04).
PSA responses (i.e., PSA30, PSA50, PSA90) all favored patients receiving a docetaxel re-challenge:

Dr. Oldenburg concluded his presentation by discussing the evidence for and against a second taxane with the following take home points:
- Given that evidence is limited, academic trials are invaluable
- Taxanes are superior to a second androgen receptor pathway inhibitor
- Biomarkers are needed: ctDNA has not shown a treatment prediction advantage as of yet in ProBrio
- Currently, the best evidence is for cabazitaxel, but there is no head to head comparison with docetaxel
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Mahler M, Al-Ezzi E, Shrem NS, et al. UnCHAARTED territory: The role of docetaxel following chemohormonal therapy for metastatic castration-sensitive prostate cancer. Urol Oncol. 2022 Dec;40(12):539.e17.539.e22.
- Lavaud P, Gravis G, Foulon S, et al. Anticancer activity and tolerance of treatments received beyond progression in men treated upfront with androgen deprivation therapy with or without docetaxel for metastatic castration-naïve prostate cancer in the GETUG-AFU 15 phase 3 trial. Eur Urol. 2018 May;73(5):696-703.
- De Laere B, Crippa A, Discacciati A, et al. Androgen receptor pathway inhibitors and taxanes in metastatic prostate cancer: An outcome-adaptive randomized platform trial. Nat Med. 2024 Nov;30(11):3291-3302.
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- de Wit R, de Bono J, Sternberg CN, et al. Cabazitaxel versus Abiraterone or Enzalutamide in Metastatic Prostate Cancer. N Engl J Med 2019 Dec 26;381(26):2506-2518.