(UroToday.com) The 2025 EAU annual meeting featured a session on managing metastatic castration resistant prostate cancer (mCRPC) after triplet therapy for metastatic hormone sensitive prostate cancer (mHSPC) and a presentation by Dr. Niven Mehra discussing utilization of PARP inhibitors alone or in combination. Dr. Mehra started his presentation by emphasizing the importance of biomarker testing, given that many genes in the HRR pathway are involved in prostate cancer. The following shows the HRR pathway gene hierarchy and the effect of a single gene alteration on HRR:

Dr. Mehra also highlighted molecular testing of HRR mutations beyond BRCA:
- Next generation sequencing (NGS) test:
- Which NGS test should be used? What panel composition?
- What details on the test results are important?
- BRCA status: is the patient BRCA1 or BRCA2 or wildtype?
- Non-BRCA HRR mutation status: which genes should be tested?
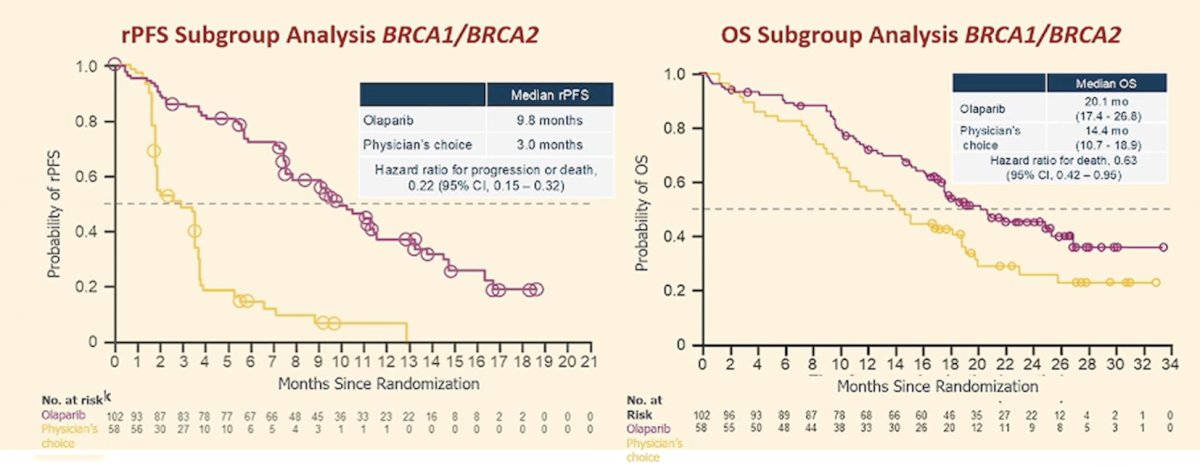
With regards to monotherapy PARP inhibitors, Dr. Mehra discussed the PROfound trial, which assessed olaparib monotherapy.1 In this trial, olaparib was permitted if there was progression on the physician’s choice of treatment, with 80% of patients crossing over to olaparib. In the TRITON3 trial assessing rucaparib,2 crossover was also permitted if there was progression on physician’s choice of treatment. This included 75% of patients, specifically 34/44 progressing after docetaxel, and 29/40 progressing after abiraterone/enzalutamide. In the PROfound BRCA1/BRCA2 cohort, the median radiographic progression free survival was 9.8 months for olaparib versus 3.0 months for physician’s choice (HR 0.22, 95% CI 0.15-0.32). For overall survival, the median was 20.1 months for olaparib versus 14.4 months for physician’s choice (HR 0.63, 95% CI 0.42-0.96):
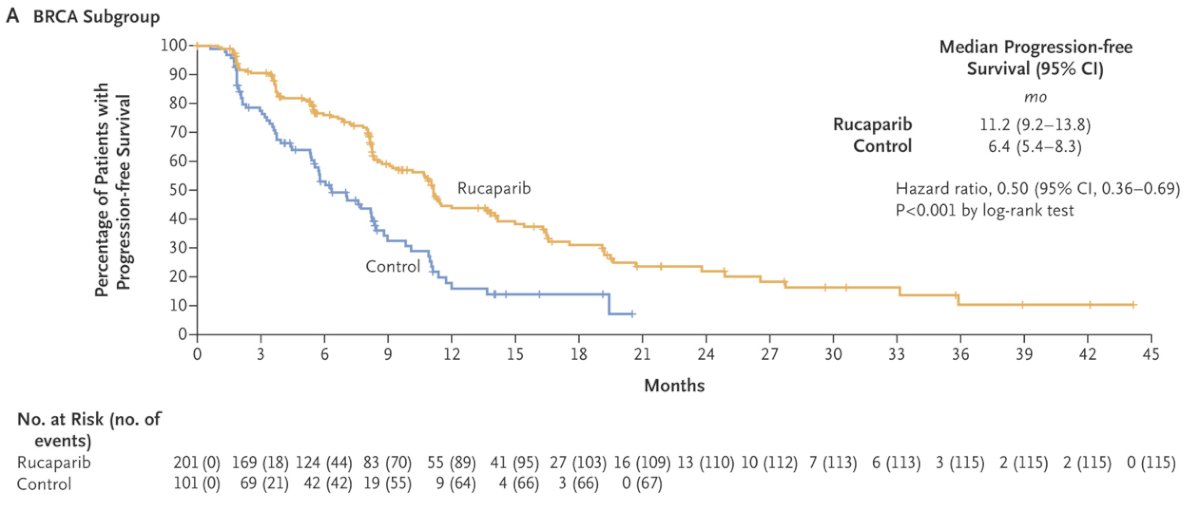
In the TRITON3 trial, rucaparib demonstrated a significant improvement in imaging-based progression-free survival (median:10.2 versus 6.4 months; HR: 0.61, 95% CI: 0.47 to 0.80, p < 0.001), compared to a physician’s choice control (docetaxel or an alternative androgen receptor pathway inhibitor). This benefit was most pronounced in the BRCA patient subgroup (median: 11.2 versus 6.4 months; HR: 0.50, 95% CI: 0.36 to 0.69, p < 0.001).
Dr. Mehra notes that in a subgroup analysis from both PROfound and TRITON3, there was no efficacy of a PARP inhibitor for the HRR mutation ATM versus standard of care. There is also limited evidence for the efficacy of PARP inhibitor monotherapy for non-BRCA HRR mutations, thus not all HRR mutation genes are equal and can be grouped together. This includes PALB2, RAD51B, RAD51C, RAD51D, RAD54L, and BRIP1 (none of these genes have EMA approval).
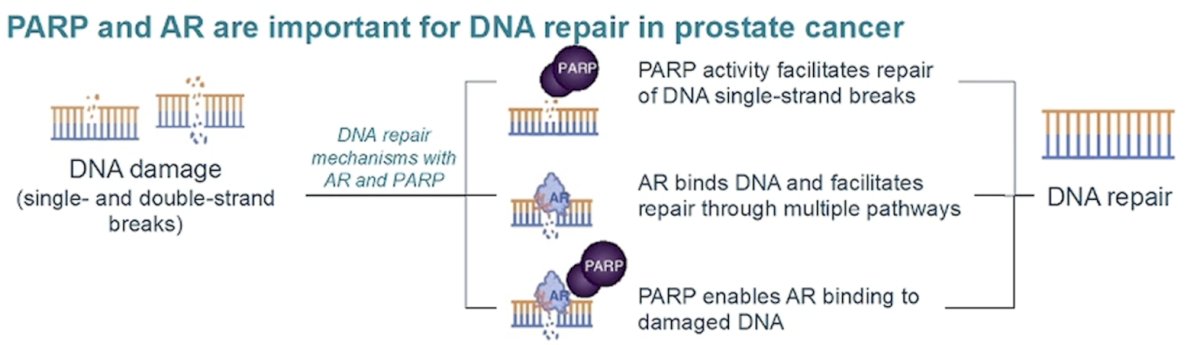
Switching to PARP inhibitor combination therapy, there is preclinical rationale for a combined effect of PARP and androgen receptor inhibition, given that both PARP and the androgen receptor are important for DNA repair in prostate cancer:
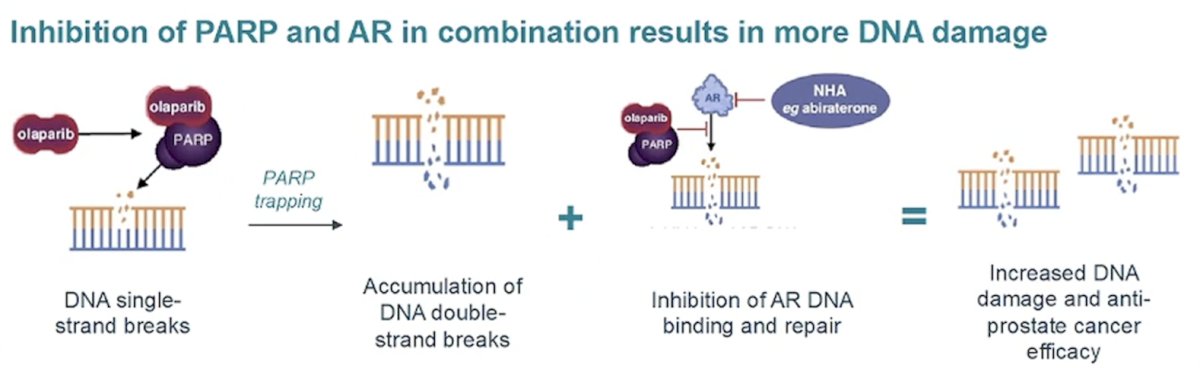
Additionally, the inhibition of PARP and the androgen receptor in combination results in more DNA damage:
The following figure demonstrates the current landscape of efficacy of PARP inhibition + androgen receptor pathway inhibitors in combination in BRCA, non-BRCA HRR mutation, and unselected populations:
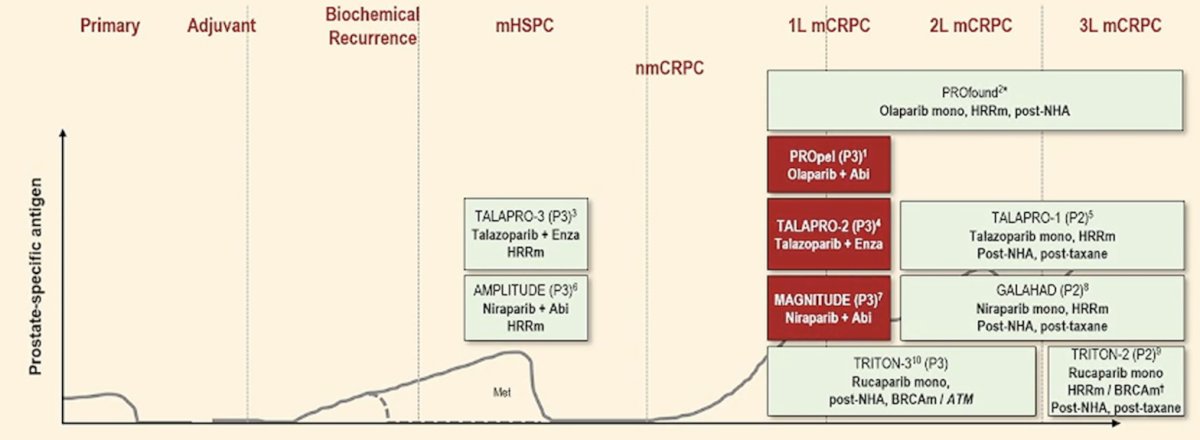
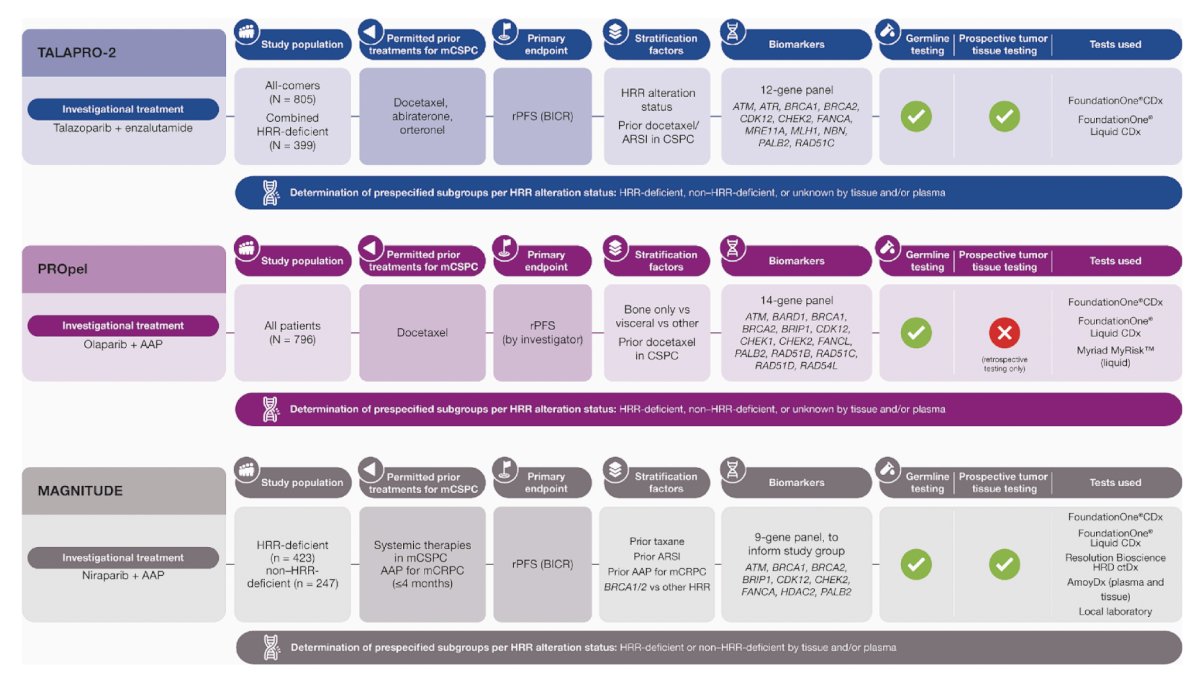
At a high level, the TALAPRO-2,3 PROpel,4 and MAGNITUDE5 trials evaluating PARP inhibitors + androgen receptor pathway inhibitors in the first line mCRPC setting are outlined below:6
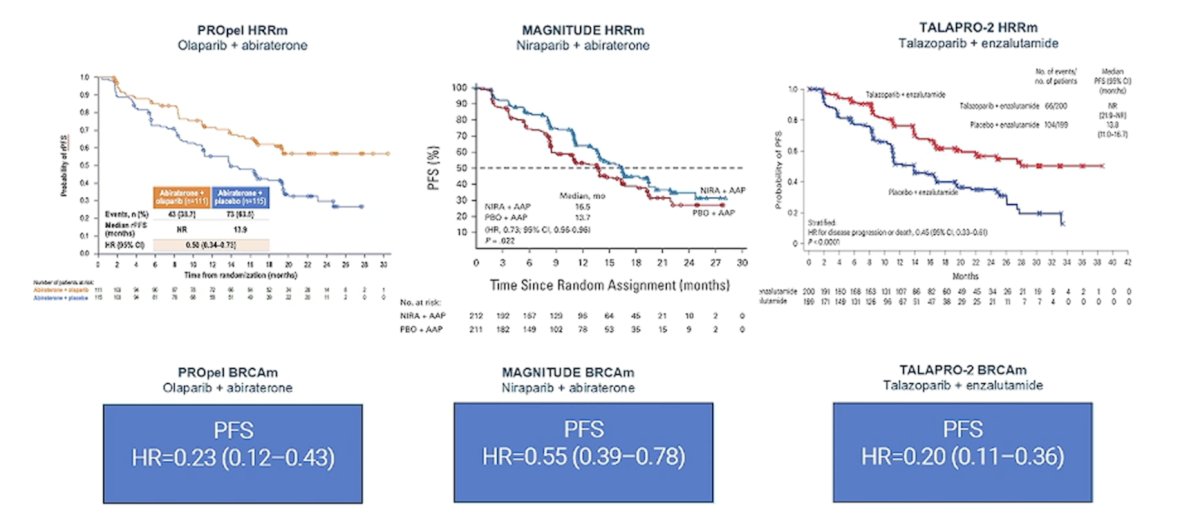
The efficacy of all three trials showed benefit in the intention to treat analysis for the PARP inhibitor + androgen receptor pathway inhibitor arm, with noteworthy results in the BRCA mutated patients:
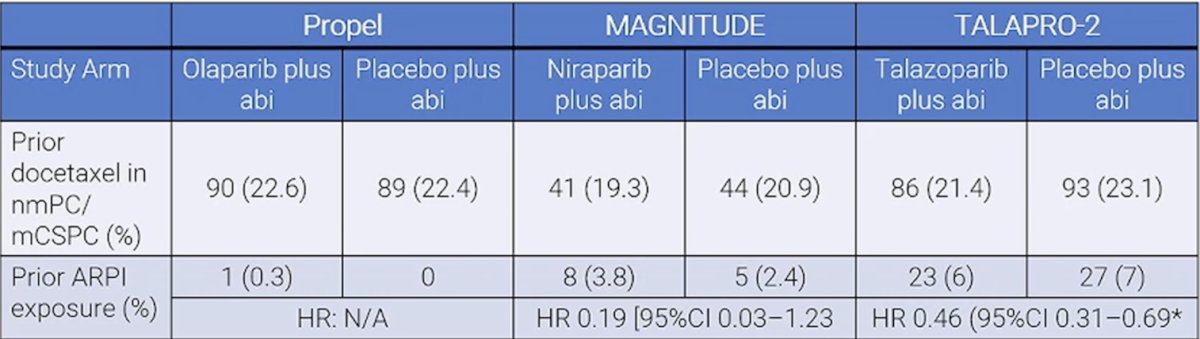
Importantly, there is limited evidence of an effect of PARP inhibitor + androgen receptor pathway inhibitor in patients with prior androgen receptor pathway inhibitor exposure, although there does appear to be a signal of benefit (although with a very small sample size):
Dr. Mehra concluded his presentation by discussing the utilization of PARP inhibitors alone or in combination with the following take home points:
- Among androgen receptor pathway inhibitor naïve patients:
- If there is a BRCA mutation: treat with a PARP inhibitor + androgen receptor pathway inhibitor
- If there is an HRR mutation: consider the PARP inhibitor + androgen receptor pathway inhibitor combination, however the benefit to toxicity ratio is key
- If the patient is HRR wild type: there should be careful consideration of a PARP inhibitor + androgen receptor pathway inhibitor combination, due to the lower benefit to toxicity ratio
- Among androgen receptor pathway inhibitor exposed (triplet therapy) patients:
- The evidence for PARP inhibitor + androgen receptor pathway inhibitor combinations is minimal
- There is limited evidence of an androgen receptor pathway inhibitor switch
- Toxicity of PARP inhibitor + androgen receptor pathway inhibitor combination is much greater than PARP inhibitor monotherapy
- BRCA1 and BRCA2: there is evidence for PARP inhibitor monotherapy
- Non-BRCA HRR mutation: consider PARP inhibitor + androgen receptor pathway inhibitor combination (CDK12, PALB2)
- Non HRR mutation: do not consider PARP inhibitor + androgen receptor pathway inhibitor combination
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- de Bono J, Mateo J, Fizazi K, et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med 2020 May 28;382(22):2091-2102.
- Fizazi K, Piulats JM, Reaume MN, et al. Rucaparib or Physician’s Choice in Metastatic Prostate Cancer. N Engl J Med. 2023 Feb 23;388(8):719-732.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.
- Saad F, Clarke NW, Oya M, et al. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomized, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108.
- Chi KN, Rathkopf D, Smith MR, et al. Niraparib and abiraterone acetate for metastatic castration-resistant prostate cancer. J Clin Oncol. 2023 Jun 20;41(18):3339-3351.
- McKay RR, Morgans AK, Shore ND, et al. First-line combination treatment with PARP and androgen receptor-signaling inhibitors in HRR-deficient mCRPC: Applying clinical study findings to clinical practice in the United States. Cancer Treat Rev. 2024 May:126:102726