(UroToday.com) The 2025 EAU annual meeting featured a session on managing metastatic castration resistant prostate cancer (mCRPC) after triplet therapy for metastatic hormone sensitive prostate cancer (mHSPC) and a presentation by Dr. Bertrand Tombal discussing the evidence for and against a second androgen receptor pathway inhibitor. Currently, back to back androgen receptor pathway inhibitors are widely used in the treatment of mCRPC. Barata and colleagues1 recently looked at mCRPC treatment patterns among patients across 5 European countries who received treatment with a novel hormonal therapy in the mHSPC setting (n = 76), noting that the most common first line treatment in the mCRPC setting was abiraterone:

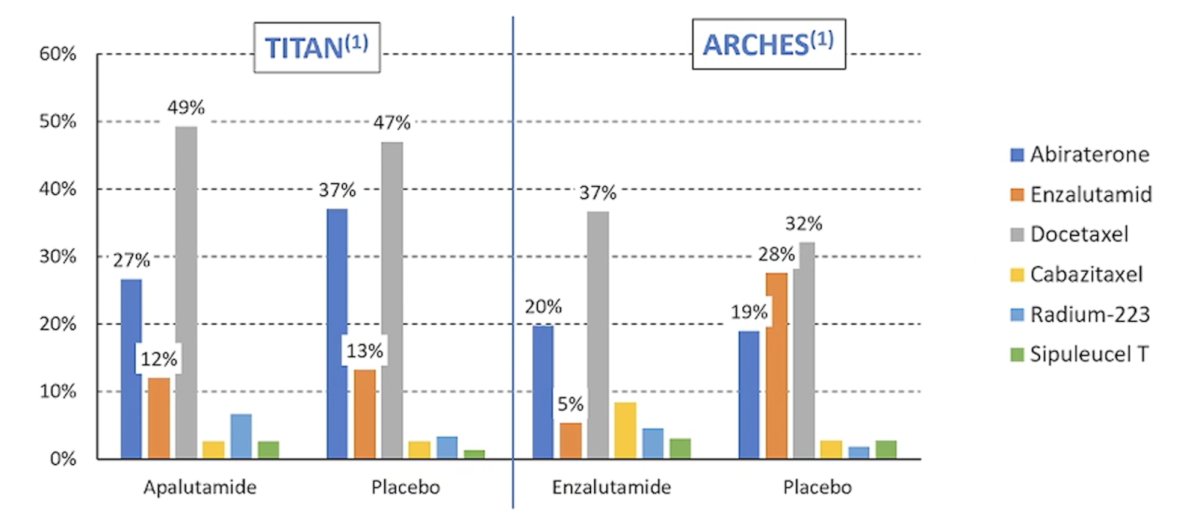
Treatment at time of progression in registration trials also provides several important insights. In TITAN,2 the most common treatment at progression in both arms was docetaxel, which was also the most common treatment at progression in the ARCHES trial:3
With regards to PEACE-1,4 in both abiraterone and placebo arms, cabazitaxel was the most common first line mCRPC therapy used, and in ARASENS,5 the most common first line mCRPC agent used was abiraterone:

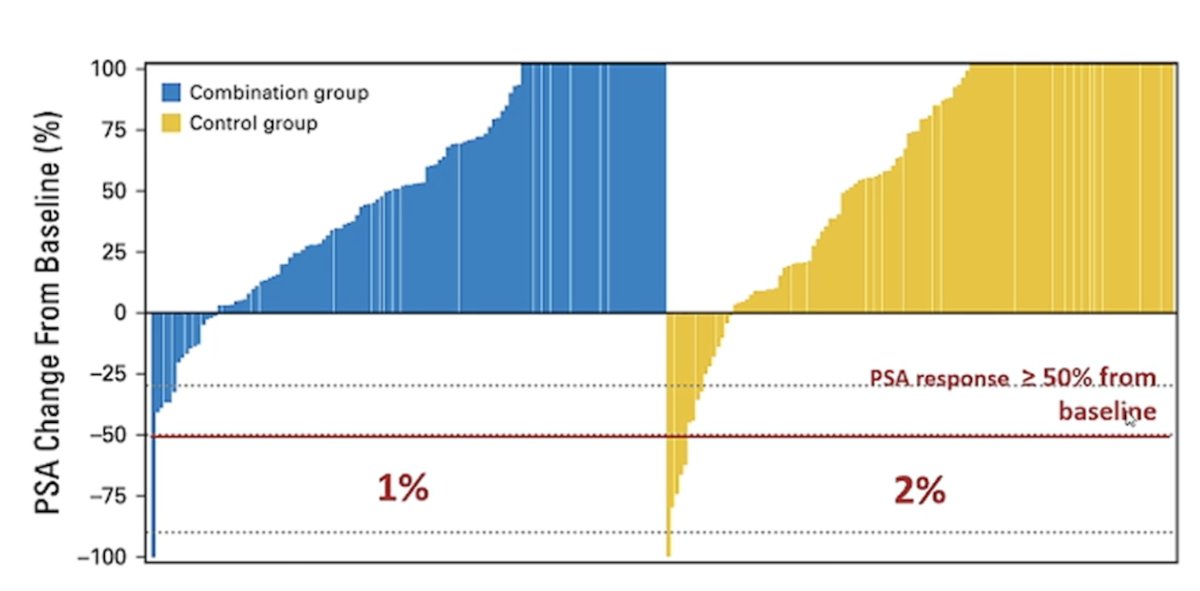
Next, Dr. Tombal noted that although androgen receptor pathway inhibitors are commonly used in mCRPC, the responses, mostly on PSA, are usually short. The PLATO trial6 was published in 2018 and assessed abiraterone alone or in combination with enzalutamide in 251 mCRPC patients. Unfortunately, the PSA50 responses in the combination group were only 1% and in the control group was 2%:
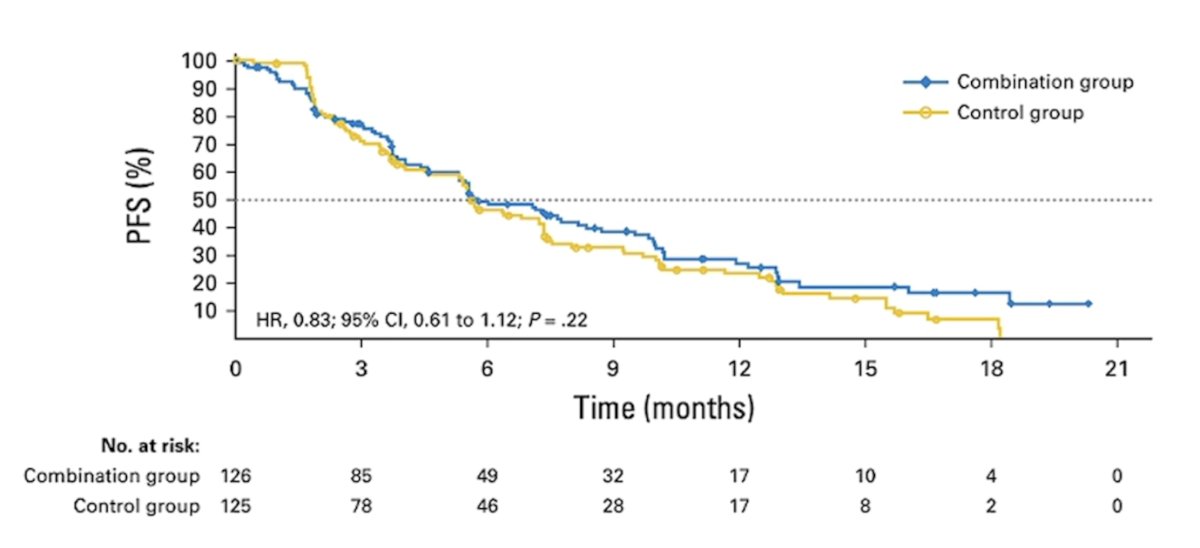
Moreover, the median progression free survival was only 5.6 months, with no difference between the two groups:
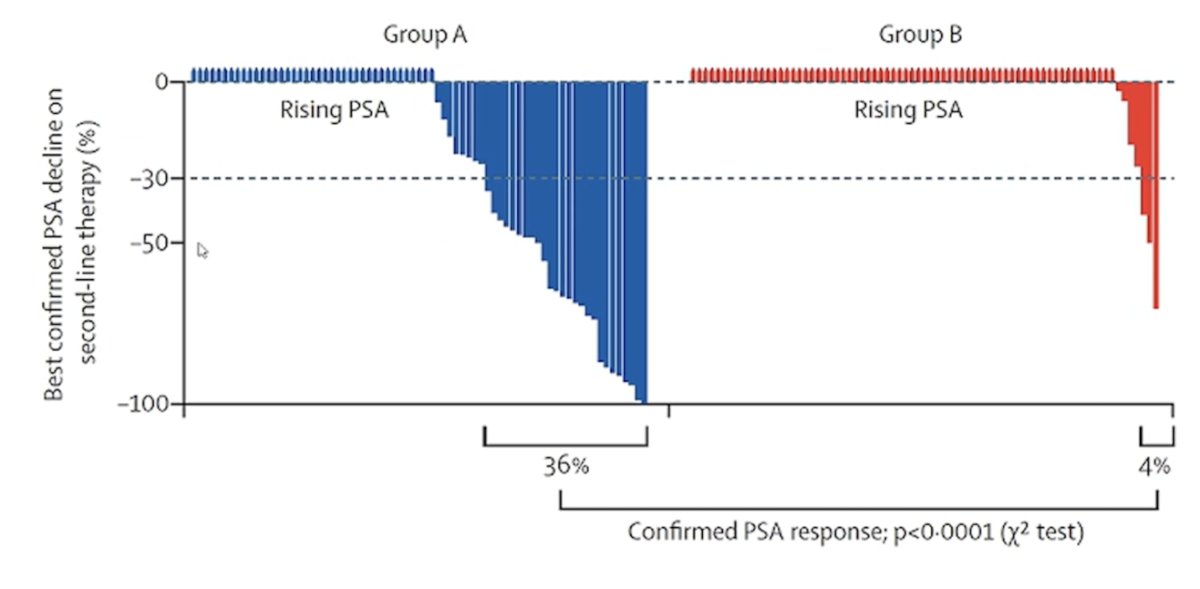
In a phase II trial published in Lancet Oncology in 2019, Khalaf et al.7 demonstrated that the sequence of abiraterone followed by enzalutamide was associated with superior time to second PSA progression by 4 months and had a deeper response to second line therapy compared to those who received enzalutamide followed by abiraterone:
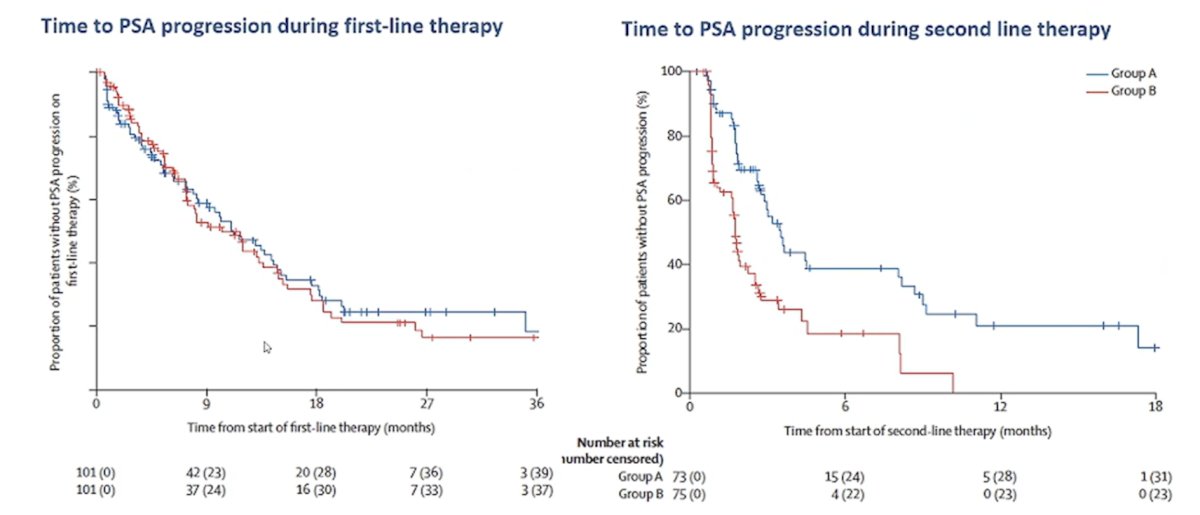
It must be noted however that overall response rates were modest in both arms (PSA response rate: 36% for abiraterone-enzalutamide versus 4% for enzalutamide-abiraterone sequences):
In work from Dr. Dan George and Dr. Tombal, they assessed treatment patterns and outcomes in patients with metastatic castration-resistant prostate cancer in a real-world clinical practice setting in the United States.8 Of 2,559 patients with mCRPC, 1,980 (77%) received at least one line of life-prolonging therapy (abiraterone, enzalutamide, docetaxel, cabazitaxel, sipuleucel-T, or radium-223). Abiraterone + prednisone and enzalutamide accounted for 65% of first-line therapies and 54% of second-line therapies, and docetaxel was the most common third-line therapy (24%).
Dr. Tombal noted that each time a second androgen receptor pathway inhibitor has been used as a “best valuable comparator”, it showed significantly lower radiographic progression free survival and overall survival in most cases:
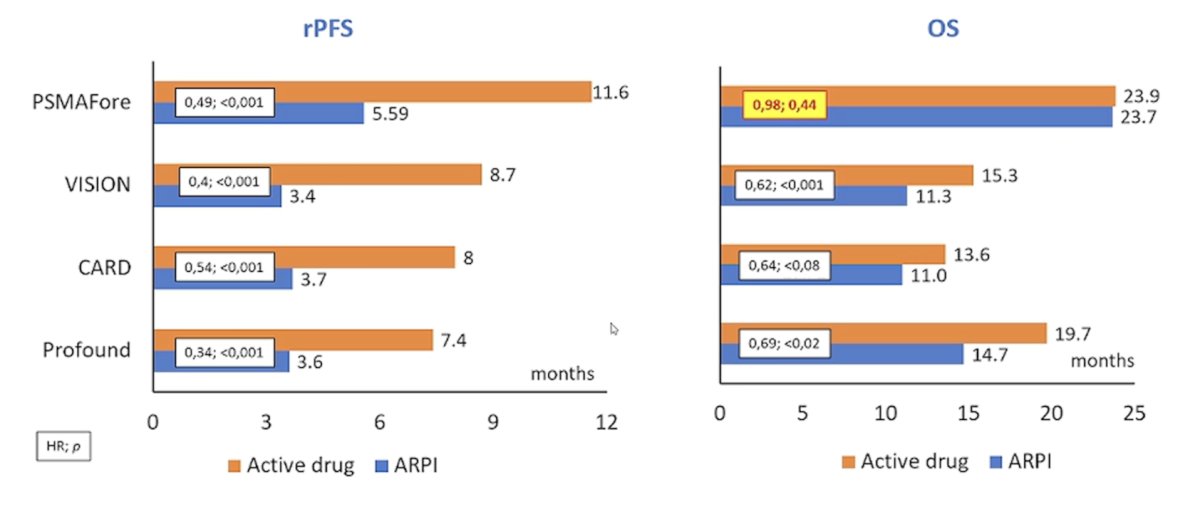
As such, a second androgen receptor pathway inhibitor is not considered by the guidelines and consensus. Although, Dr. Tombal mentioned what he calls the “PSMAfore paradox.” PSMAfore9 showed that 177Lu-PSMA-617 (median 11.6 months) demonstrated a radiographic progression free survival benefit versus androgen receptor pathway inhibitor change (median 5.59 months; HR 0.49, 95% CI 0.39–0.61) in chemotherapy-naïve mCRPC patients:
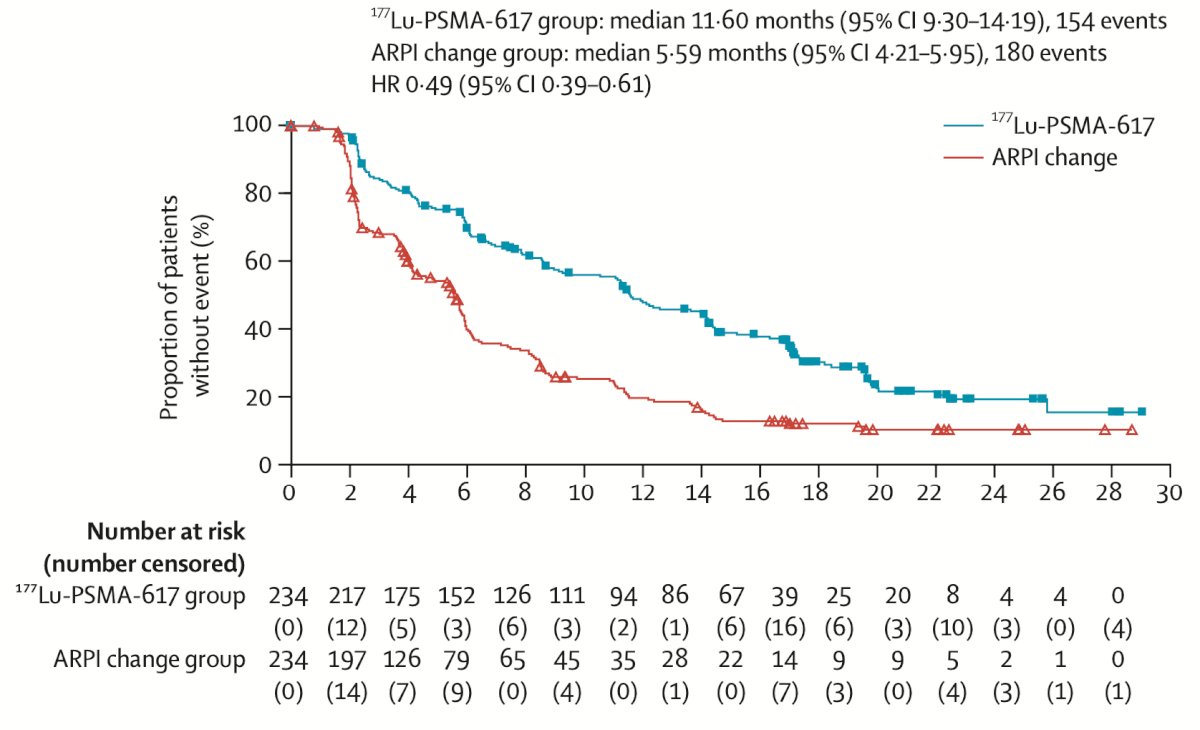
However, overall survival showed no difference between the two arms (HR 0.98, 95% CI 0.75-1.28), with a notable 57% of patients in the androgen receptor pathway inhibitor change arm receiving LuPSMA. Thus, there may be some activity in the androgen receptor pathway inhibitor change arm with a second androgen receptor pathway inhibitor.
Dr. Tombal concluded his presentation by discussing the evidence for and against a second androgen receptor pathway inhibitor with the following take home points:
- Prolonged responses are sometimes seen, but androgen receptor pathway inhibitor switch should not replace active treatments such as cabazitaxel, PARP inhibitors, LuPSMA, or radium-223
- One interpretation of PSMAfore is that slightly delaying the following line of treatment with an androgen receptor pathway inhibitor switch, especially in patients having received abiraterone, is not that detrimental
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Barata PC, Leith A, Ribbands A, et al. Real-world treatment patterns among patients with metastatic castration-resistant prostate cancer: Results from an International Study. Oncologist. 2023 Sep 7;28(9):e737-e747.
- Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med 2019 Jul 4;381(1):13-24.
- Armstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy with Enzalutamide or Placebo in Men with Metastatic Hormone-Sensitive Prostate Cancer. J Clin Oncol. 2019 Nov 10;37(32):2974-2986.
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142.
- Attard G, Borre M, Gurney H, et al. Abiraterone alone or in combination with enzalutamide in metastatic castration-resistant prostate cancer with rising prostate-specific antigen during enzalutamide treatment. J Clin Oncol. 2018 Sep 1;36(25):2639-2646.
- Khalaf DJ, Annala M, Taavitsainen S, et al. Optimal sequencing of enzalutamide and abiraterone acetate plus prednisone in metastatic castration-resistant prostate cancer: a multicentre, randomised, open-label, phase 2, crossover trial. Lancet Oncol. 2019l20(12):1730-1739.
- George DJ, Sartor O, Miller K, et al. Treatment patterns and outcomes in patients with metastatic castration-resistant prostate cancer in a real-world clinical practice setting in the United States. Clin Genitourin Cancer. 2020 Aug;18(4):284-294.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.