(UroToday.com) The 2025 EAU annual meeting featured a session on managing metastatic castration resistant prostate cancer (mCRPC) after triplet therapy for metastatic hormone sensitive prostate cancer (mHSPC) and a presentation by Dr. Himisha Beltran discussing aggressive variants. After triplet therapy, there are several treatment options available, including (i) an androgen receptor pathway inhibitor switch, (ii) Lu-PSMA-617, (iii) PARP inhibitor, (iv) radium-223, and (v) cabazitaxel.
The role of platinum chemotherapy in mCRPC dates back several decades, with carboplatin + taxane chemotherapy showing activity in pooled analyses, activity in DNA repair mutations (ie. BRCA), small cell carcinoma, and aggressive variant prostate cancer.
In 2020, Schmid and colleagues1 assessed the activity of platinum-based chemotherapy in patients with advanced prostate cancer with and without DNA repair gene aberrations. This was a case series of 508 patients with mCRPC treated with platinum chemotherapy at 25 academic medical centers from 12 countries. They noted a PSA decrease >= 50% in 47.1% of patients with known DNA repair deficits, and 36.1% in patients with no DNA repair deficits. In 44 patients with BRCA2 gene alterations, the PSA decrease >= 50% was 63.9% and soft tissue response was 50.0%. Among patients with no profiling available, PSA and soft tissue responses were 28.5% and 20.5%, respectively. Dr. Beltran cautions that there is often cross resistance between platinum and PARP inhibitors for BRCA, so we should consider PARP inhibitors in these patients if available.
Dr. Beltran notes that there is limited prospective clinical trial data for small cell/neuroendocrine prostate cancer. In 2002, a phase 2 study assessed doxorubicin, etoposide, and cisplatin in patients with fully characterized small cell carcinoma of the prostate, noting that among 36 patients assessable for response, 22 patients had a partial response (61% response rate).2 Notably, toxicity was severe, with grade 3 or 4 neutropenia noted in 100% of patients, thrombocytopenia in 66%, mucositis in 21%, and infection in 68%; three patients died of toxicity. The median time to progression and overall survival were 5.8 months, and 10.5 months, respectively. In the 2024 NCCN guidelines the general recommendation for treatment of neuroendocrine prostate cancer is to treat it like small cell lung cancer: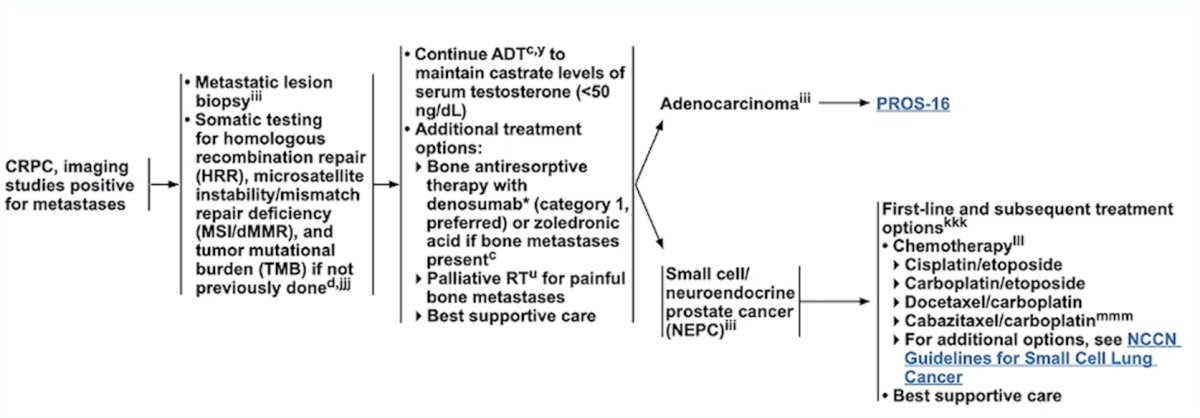
Dr. Beltran notes that “de novo” neuroendocrine prostate cancer has similar pathologic and molecular features as treatment emergent neuroendocrine prostate cancer and can be heterogeneous. For instance, some patients present with “neuroendocrine features”, but are androgen receptor positive, their PSA is high, and their PSMA PET is positive. Currently, these patients are managed like mHSPC, but there are important treatment considerations, such as whether we should give triplet or quadruplet therapy (ADT, androgen receptor pathway inhibitor, docetaxel, and carboplatin).
The term “aggressive variant prostate cancer” was used as specific clinical criteria for therapy intensification (platinum-taxane) phase 2 clinical trials for CRCP, including the following criteria:
- Exclusive visceral metastases
- Lytic bone metastases
- Bulky lymphadenopathy (>= 5 cm) or mass (>= 5cm, Gleason >= 8) in the prostate/pelvis
- Low PSA (<10 ng/mL) at initial presentation (before ADT) or at the time of symptomatic CRPC + high volume (>20) bone metastases
- Serum CEA and/or LDH twice the upper limit of normal
- A short interval (<6 months) to CRPC
- Small cell/neuroendocrine prostate cancer morphology
Previously, a phase 1-2 trial assessed whether adding carboplatin to cabazitaxel would improve the outcomes of men with metastatic castration-resistant prostate cancer.3 Among 160 patients in the phase 2 portion of the trial (n = 79 cabazitaxel; n = 81 cabazitaxel + carboplatin), at a median follow-up of 31.0 months (IQR 20.5-37.1), this combination improved the median progression-free survival from 4.5 months (95% CI 3.5-5.7) to 7.3 months (95% CI 5.5-8.2; HR 0.69, 95% CI 0.50-0.95, p = 0.018).
With regards to aggressive variant prostate cancer in phase 2 platinum trials, approximately 50-60% are RB1 loss, ~80% are TP53 loss, and ~50% are PTEN loss. In a post-hoc analysis of a phase 1/2 study of cabazitaxel + carboplatin versus cabazitaxel, patients with 2+ alterations in TP53, RB1, and PTEN had a longer median progression free survival (7.5 versus 1.7 months) and median overall survival (20.2 versus 8.5 months) when treated with the combination chemotherapy. So, can we use loss of 2/3 tumor suppressor genes instead of using clinical criteria? Dr. Beltran emphasized that there are numerous studies suggesting that loss of tumor suppressors is associated with aggressive disease, lineage plasticity, and androgen receptor independence.
When deciding how to test for tumor suppressor loss, there are several options:
- HSPC tissue, although this may not be present at the time of diagnosis
- Typically associated with 38% PTEN loss, 22-31% TP53 loss, and 0-2.7% RB1 loss
- ctDNA: most copy number changes (deletions) are challenging to detect
- Metastatic CRPC biopsy: the most reliable
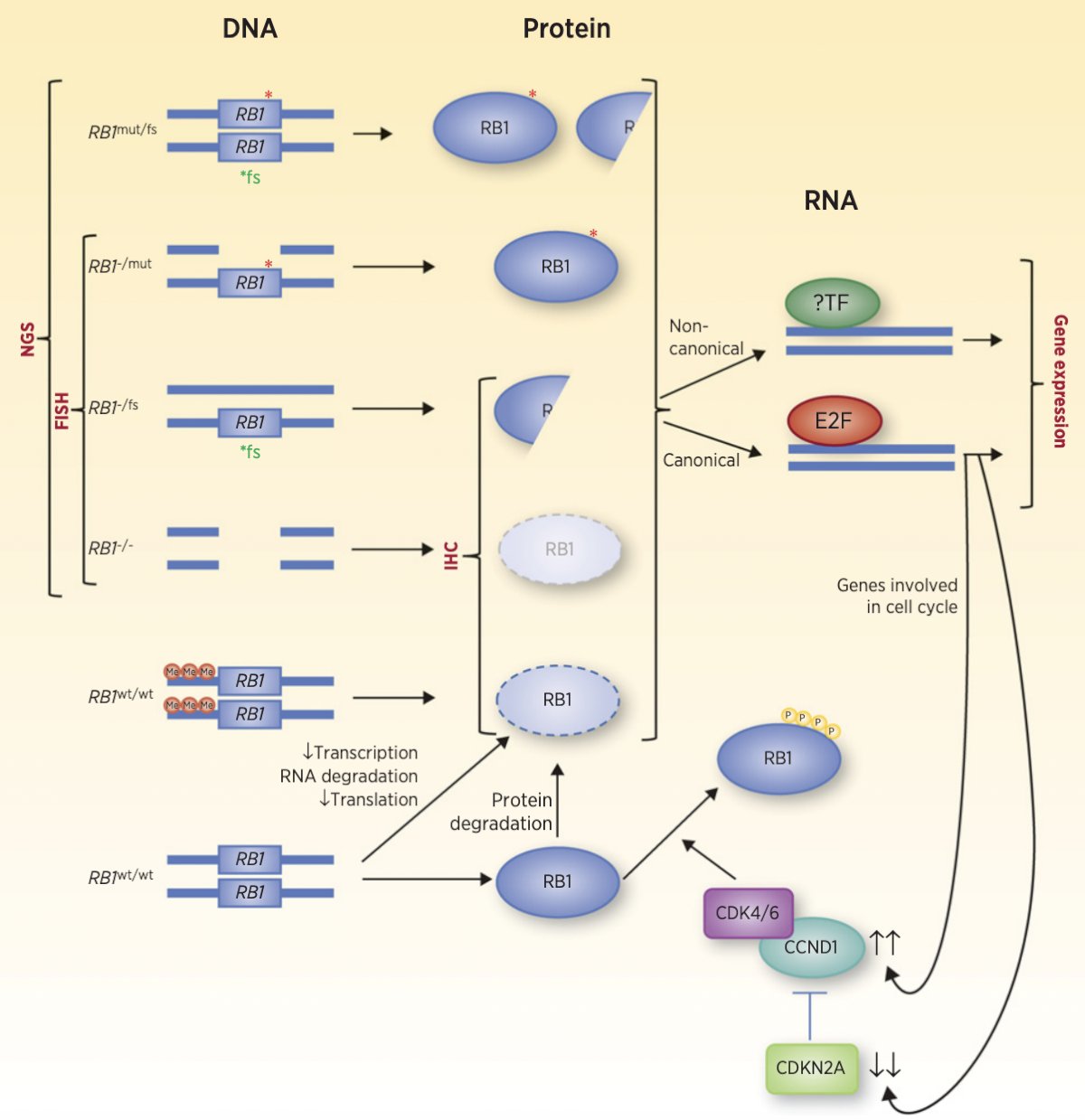
Dr. Beltran notes there are many ways to lose RB1:4
- DNA next generation sequencing, FISH
- Mutation, deletion
- Most commercial assays only report homozygous losses and do not detect complex rearrangements
- Methylation: silencing of RB1 expression
- Protein immunohistochemistry: loss of protein expression due to deletion or methylation, but does not capture mutations
- RB1 phosphorylation
- RNA-transcriptome signature
- Functional loss
- Canonical (cell cycle), or non-canonical role
Dr. Beltran then highlighted the Alliance A032102 PRecision Diagnostics In Prostate Cancer Treatment (PREDICT) trial, of which she is a co-PI with Dr. Rana McKay: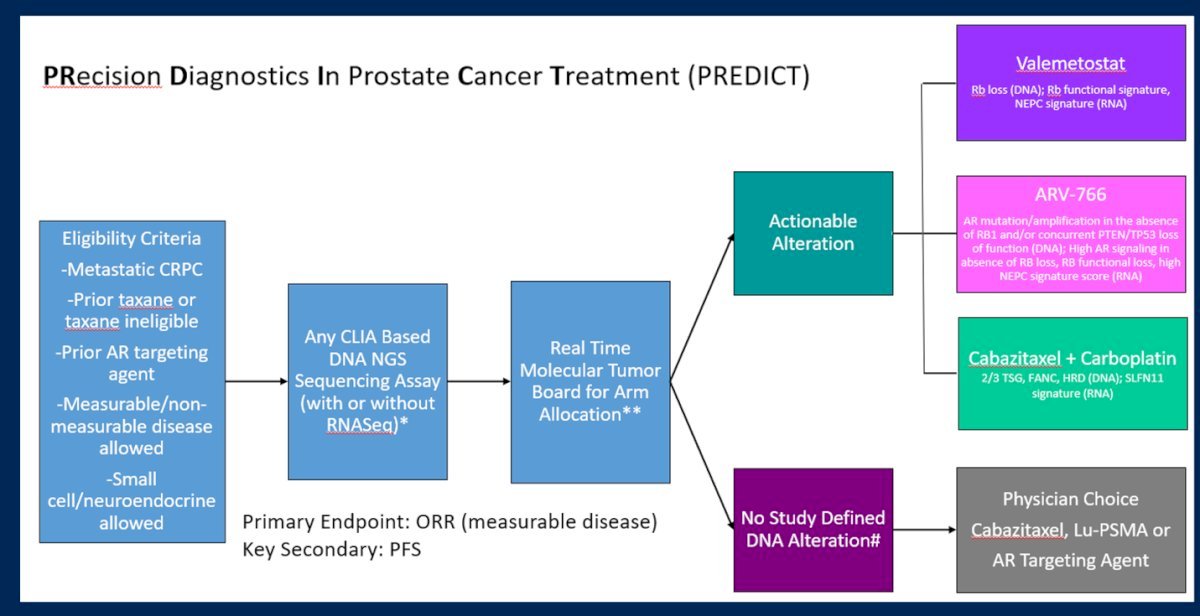
Dr. Beltran emphasized that we should be considering a new biopsy in patients if there is atypical progression, a low PSA, and in cases of aggressive disease. With regards to the role of PSMA PET imaging, if the PSMA PET is negative/low activity, it is important to look at the CT to see if the patient is progressing or responding to therapy. There may also be a role for FDG PET in these situations, and we should also consider a re-biopsy. If a re-biopsy is undertaken, there are several items to look for on a new biopsy:
- Genomics: DNA repair, tumor suppressor loss, etc
- Immunohistochemistry: quicker and more cost effect, but we need to define antibody and cutoffs for tumor suppressor loss; p53 expression is lost with deletion and increased with a mutation
- Histology
- In the future: cell surface targets, mRNA, epigenetics, spatial profiling, etc
Future systemic therapy options for aggressive variants beyond platinum will target neuroendocrine prostate cancer, specifically DLL3, which is expressed in neuroendocrine prostate cancer, and has approval for tarlatamab in small cell lung cancer. Other targets may include tumor suppressor loss (ie. AKT inhibitors), epigenetic therapies, radioligand therapies, and combination options.
Dr. Beltran concluded her presentation discussing aggressive variants with the following take home points:
- Multiple systemic therapies exist after progression on triplet therapy. The choice at first line mCRPC should consider both clinical features and molecular alterations
- Some patients have a particularly aggressive disease that warrants treatment intensification not only in mHSPC (with triplet therapy), but also potentially at mCRPC (ie. platinum)
- Molecular biomarkers to better identify aggressive variants and responders to platinum (ie. DDR, TSG loss, biopsy features) to help guide subsequent therapies are needed to improve outcomes in these patients
Presented by: Himisha Beltran, MD, Dana Farber Cancer Center, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Schmid S, Omlin A, Higano C, et al. Activity of platinum-based chemotherapy in patients with advanced prostate cancer with and without DNA repair gene aberrations. JAMA Netw Open. 2020 Oct 1;3(10):e2021692.
- Papandreou, CN, Daliani DD, Thall PF, et al. Results of a phase II study with doxorubicin, etoposide, and cisplatin in patients with fully characterized small-cell carcinoma of the prostate. J Clin Oncol. 2002 Jul 15;20(14):3072-3080.
- Corn PG, Heath EI, Zurita A, et al. Cabazitaxel plus carboplatin for the treatment of men with metastatic castration-resistant prostate cancers: A randomized, open-label, phase 1-2 trial. Lancet Oncol. 2019 Oct;20(10):1432-1443.
- Choudhury AD, Beltran H. Retinoblastoma loss in cancer: Casting a wider net. Clin Cancer Res. 2019 Jul 15;25(14):4199-4201.