(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain was host to a thematic session on clinically relevant questions in the management of advanced, hormone-sensitive prostate cancer. Dr. Noel Clarke discussed the use of intensified approaches with radiation therapy for the contemporary management of locally advanced prostate cancer.
What are the relevant questions for radiotherapy in non-metastatic prostate cancer?
- What is the benefit of ADT + radiotherapy?
- Prostate radiotherapy fractionation trends – how low can we go?
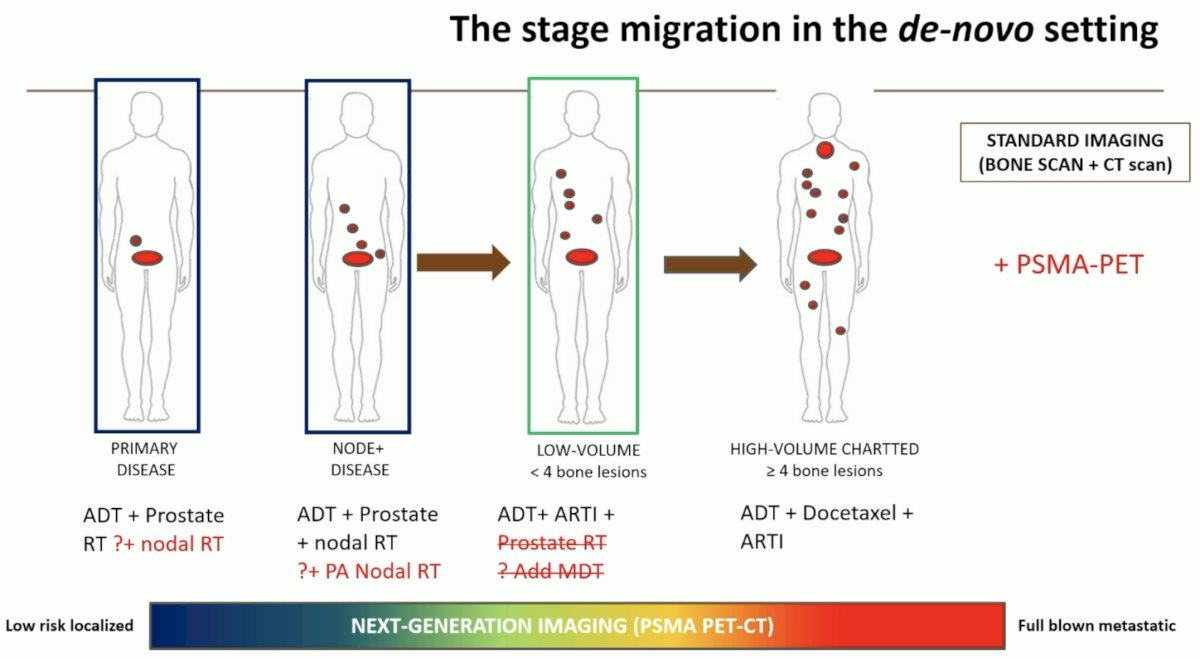
- New generation imaging blurs the distinction between high high-risk M0 and low volume M1
- Should we add additional systemic therapies to ADT and radiotherapy?
Addressing the issue of next generation imaging (i.e., PSMA PET) blurring the distinction between high high-risk M0 and low volume M1, he noted that PSMA PET likely leads to a stage migration phenomenon whereby patients with node positive-only disease on conventional imaging are likely to have low-volume metastases on PSMA PET.
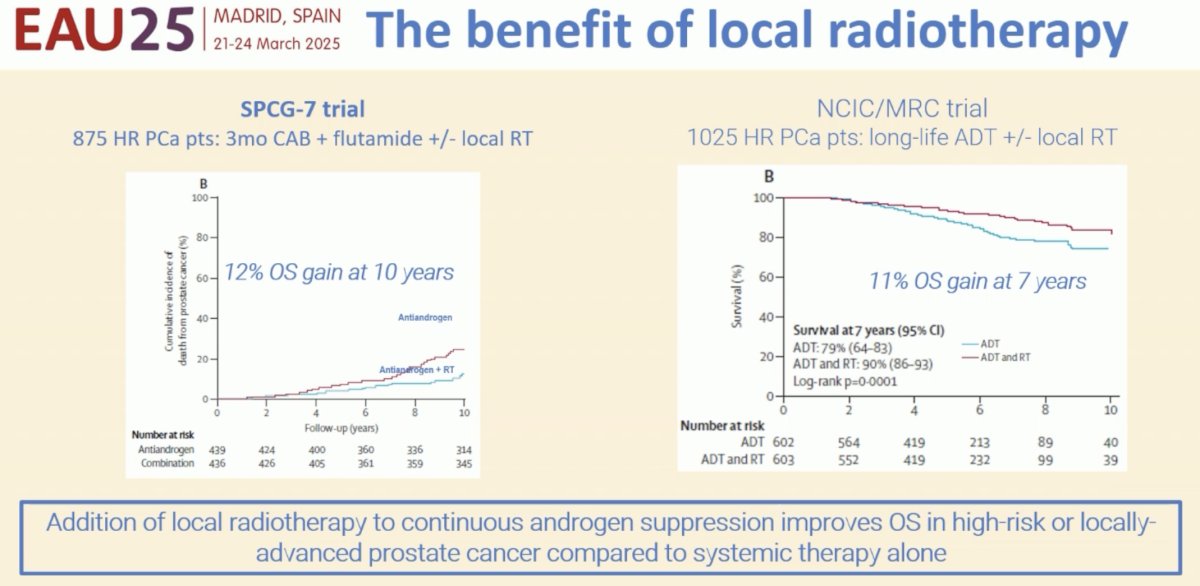
What is the evidence for combining local radiotherapy with ADT? The existing literature clearly supports the addition of local radiotherapy to continuous ADT to improve overall survival in high-risk and locally advanced prostate cancer patients. The phase III randomized SPCG-7 trial randomized patients with locally advanced prostate cancer to 3 months of complete androgen blockade followed by continuous flutamide +/- radiotherapy. Patients in the radiotherapy arm were shown to have lower 10-year prostate cancer-specific mortality (12% versus 24%) and overall mortality (29.6% versus 39.4%).1 The Canadian-UK NCIC/MRC trial demonstrated that the addition of local radiotherapy to life-long ADT was associated with an 11% improvement in 7-year overall survival.2
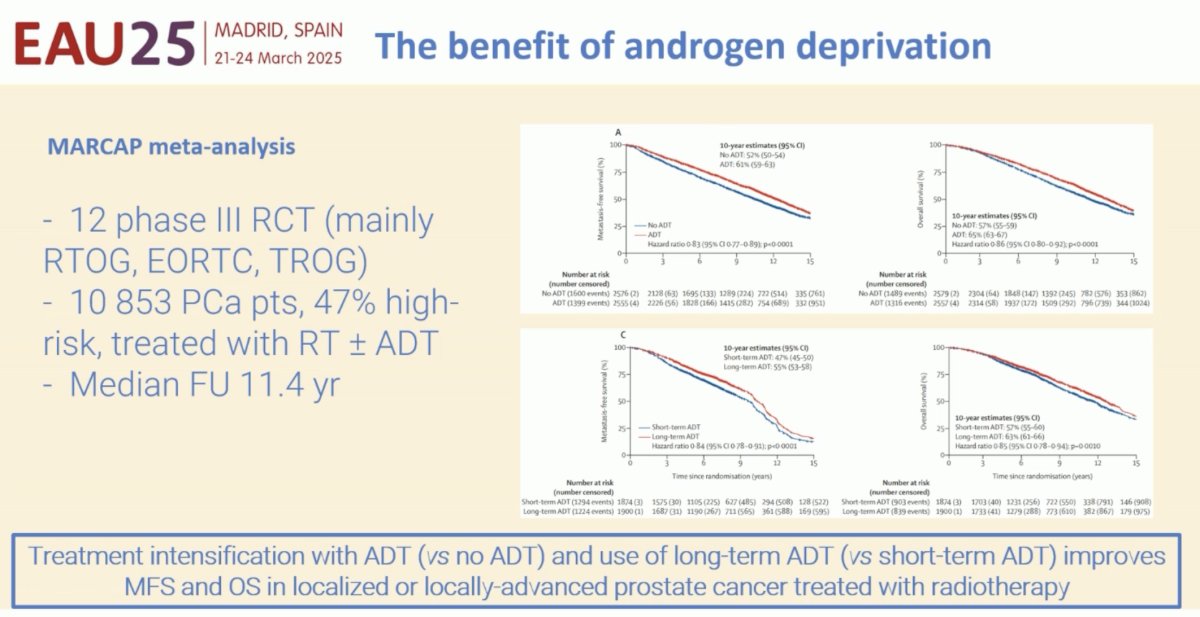
Conversely, what is the benefit of adding androgen deprivation to radiotherapy? There have been numerous studies over the past decades demonstrating that the addition of ADT to prostate radiotherapy for localized/locally advanced prostate cancer patients improves survival outcomes. Dr. Clarke highlighted the recent MARCAP meta-analysis of 12 trials with a median follow-up of 11.4 years that demonstrated that the addition of ADT to radiotherapy significantly improves metastasis-free survival (HR: 0.83, p<0·0001), as does adjuvant ADT prolongation (0.84, p<0·0001).3
Dr. Clarke’s key takeaways regarding ADT + radiotherapy were as follows:
- ADT improves the outcomes with radiotherapy
- Radiotherapy improves the outcomes with ADT
- More ADT is better than less ADT with respect to long-term prostate cancer outcomes
BUT
- Lower grade and stage prostate cancer has excellent prognosis
- More ADT is more toxic than less ADT
- More ADT may increase death rates from non-cancer causes
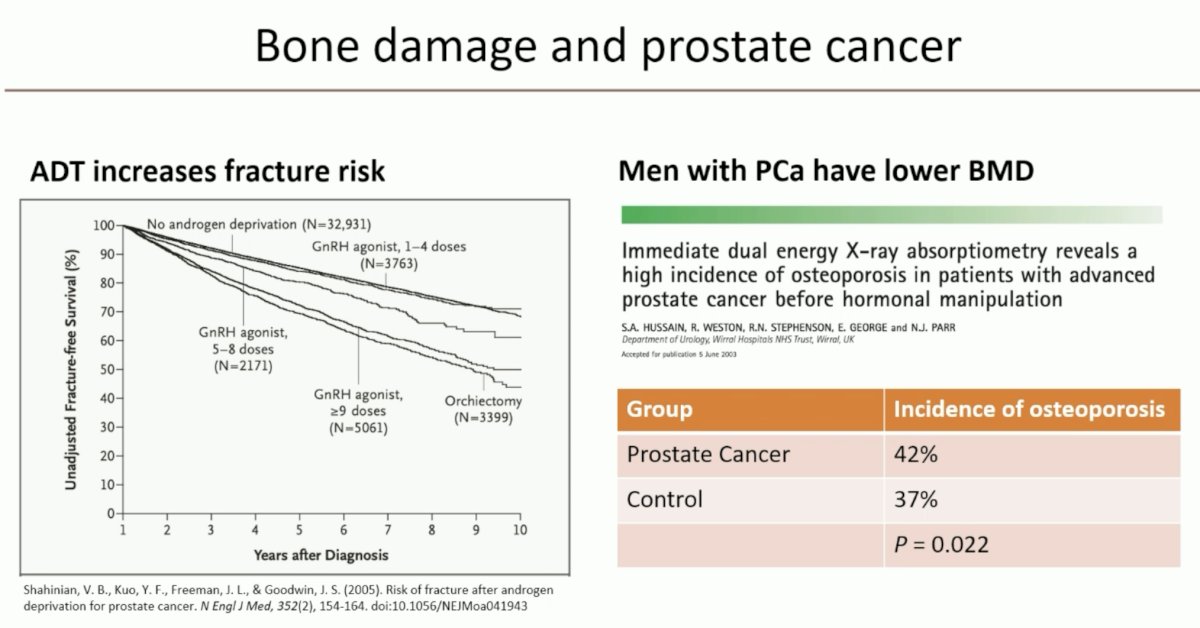
Dr. Clarke cautioned that treating physicians must be wary of the increased risk of bone loss and fractures with long-term ADT and prescribe bone-protecting agents as currently recommended by the guidelines to higher risk patients.
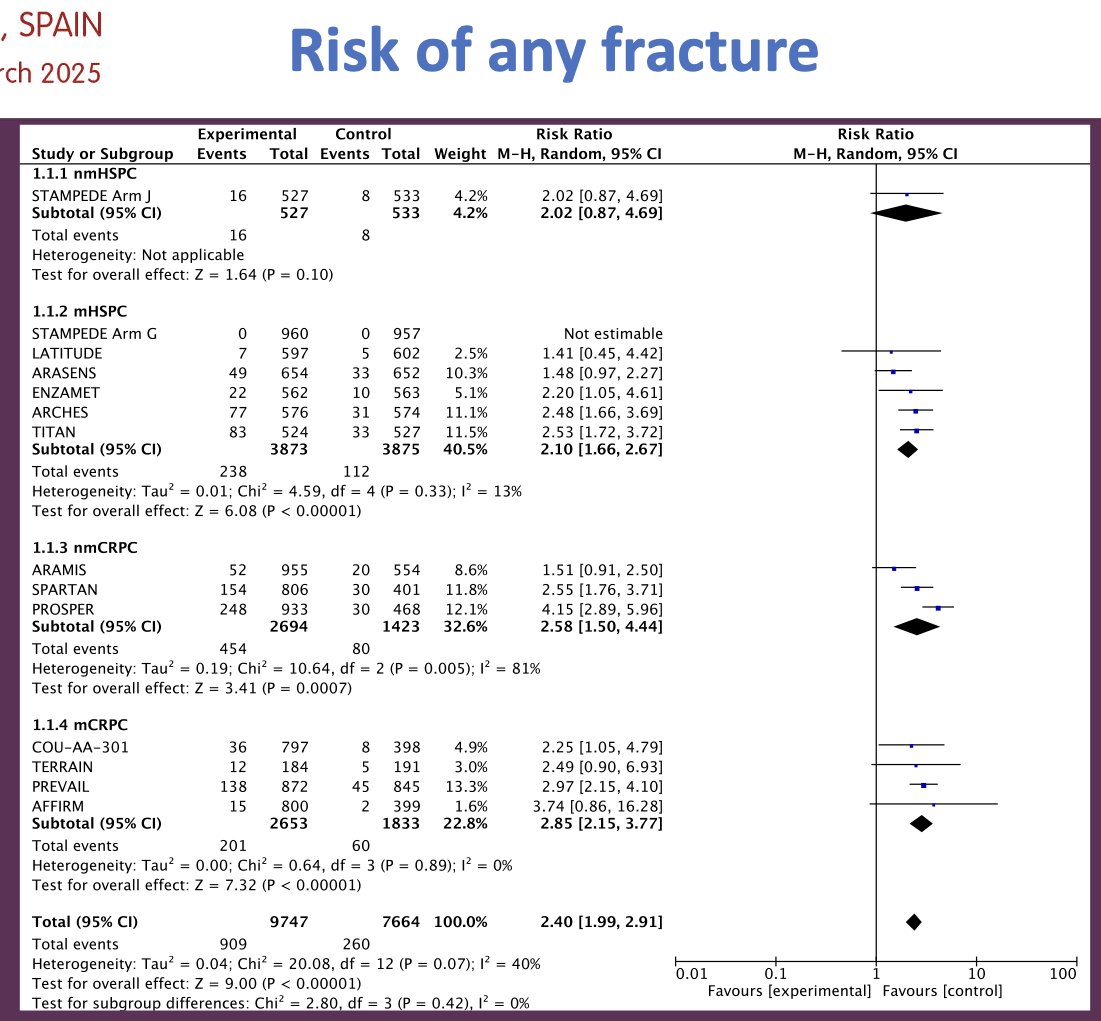
In the systematic review and meta-analysis of all randomized trials of androgen receptor signaling inhibitors (ARSIs) for non-metastatic and metastatic HSPC and CRPC (nmHSPC, mHSPC, nmCRPC, mCRPC), El-Taji et al demonstrated that the use of ARSIs increases the risk of any fracture 2.4-fold.4
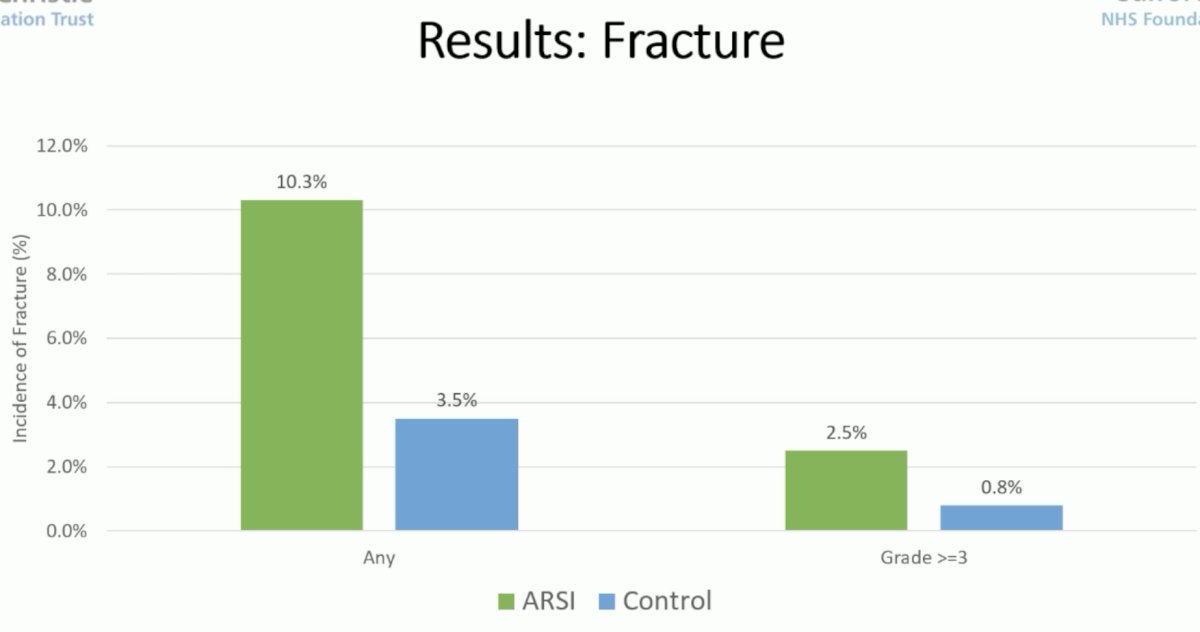
As seen in the bar graph below, long-term ARSI use increases the risk of any fracture from 3.5% to 10.3% and grade ≥3 fractures from 0.8% to 2.5%.
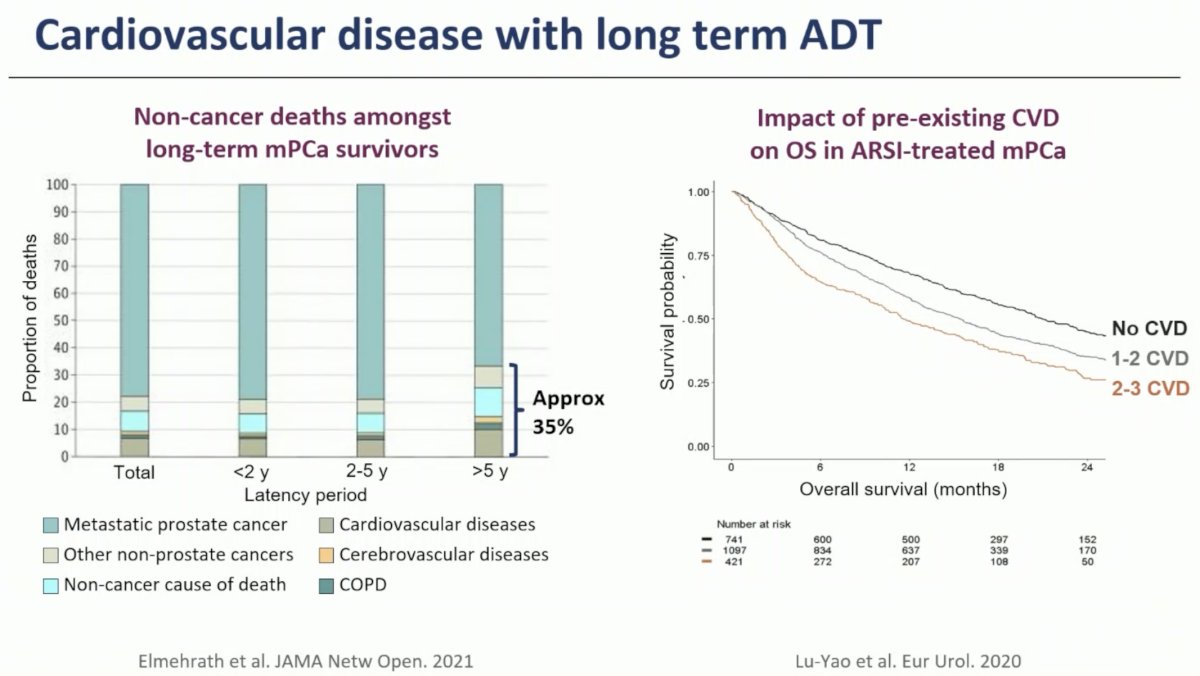
Dr. Clarke also highlighted the increased risk of cardiovascular events with long-term ADT, which is particularly significant for patients with pre-existing cardiovascular disease.
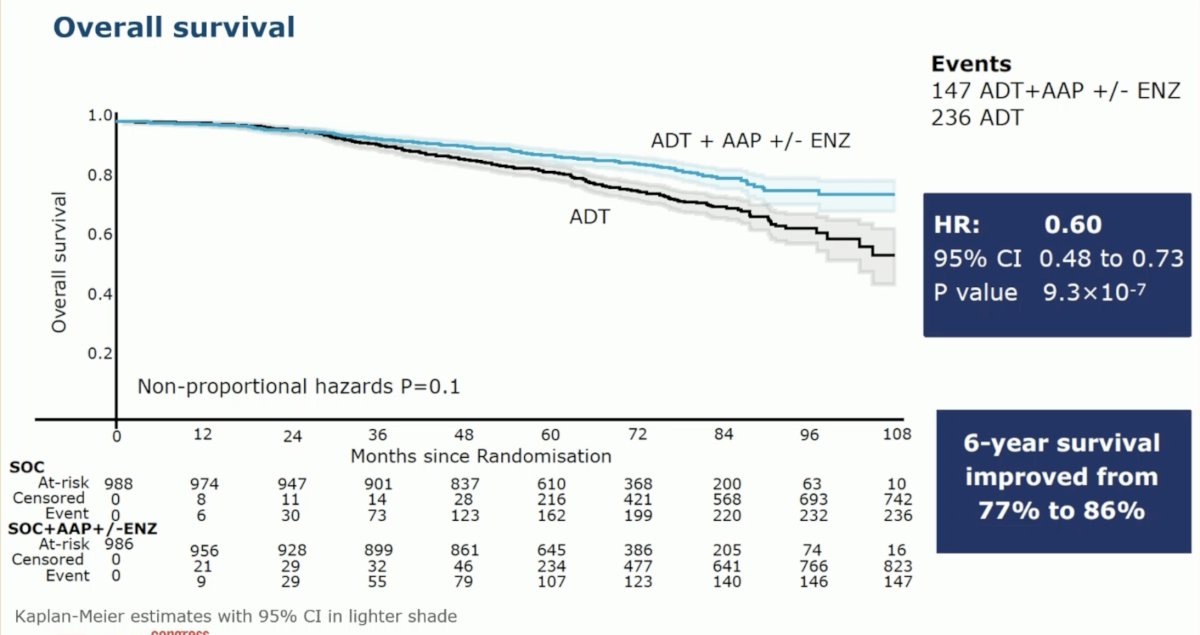
Next, Dr. Clarke addressed the use of ARSIs with ADT + radiotherapy in patients with high-risk, localized prostate cancer. In 2022, the combined results of two phase III trials (STAMPEDE arms G and J) were published in The Lancet in 2022.5 These arms of the STAMPEDE trial were designed to assess the benefit of ARSI addition to standard of care treatment for men with high-risk non-metastatic prostate cancer, as per conventional imaging, defined as:
- Node positive, OR
- If node negative:
- High-risk, defined by at least two of the following:
- cT3-4
- Gleason Score 8-10
- PSA ≥40 ng/mL
- High-risk, defined by at least two of the following:
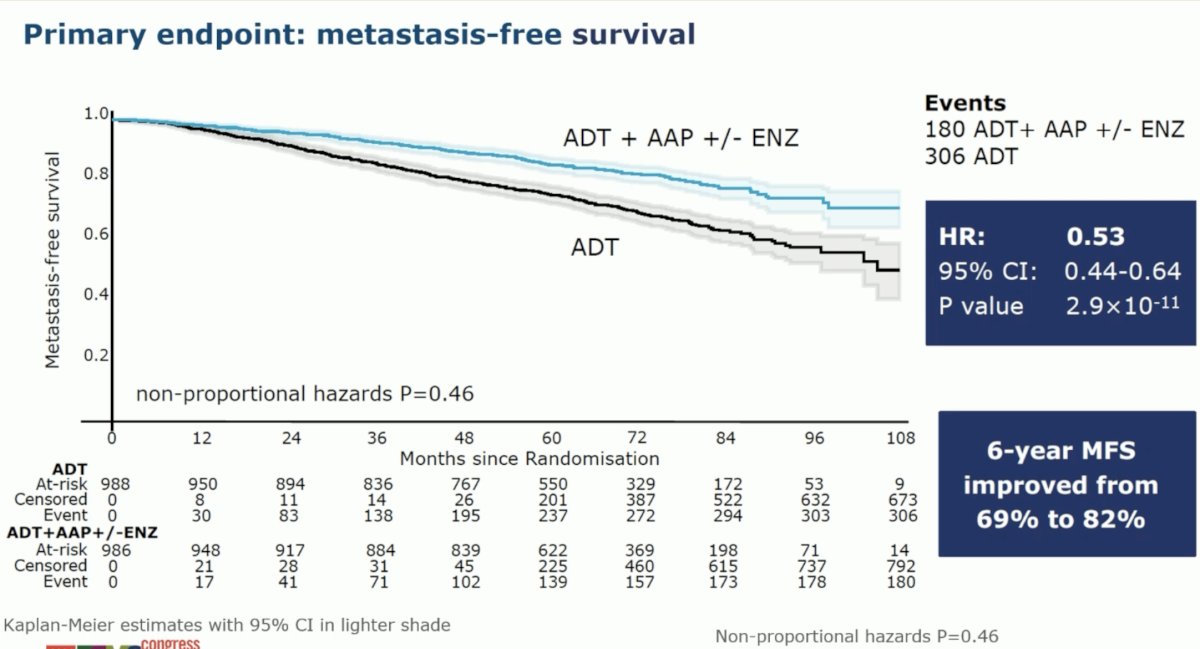
The addition of abiraterone +/- enzalutamide to radiotherapy + ADT was associated with improved metastasis-free survival (HR: 0.53, 95% CI: 0.44–0.64, p<0.000). Secondary outcomes of overall survival (HR: 0.60, 95% CI: 0.48–0.73), prostate cancer-specific survival (HR: 0.49, 95% CI: 0.37–0.65), biochemical failure-free survival (HR: 0.39, 95% CI: 0.33–0.47), and progression-free survival (HR: 0.44, 95% CI: 0.36–0.54) were all superior with the addition of abiraterone +/- enzalutamide to radiotherapy + ADT.
What about prostate radiotherapy in the metastatic setting? The current evidence supports the use of prostate radiotherapy in patients with CHAARTED low volume metastases. HORRAD was a multicenter, prospective, randomized controlled trial of 432 patients with previously untreated, de novo mHSPC at 28 centers across The Netherlands between November 2004 and September 2014. Patients were randomized in a 1:1 fashion to either ADT with external beam radiotherapy (EBRT) or ADT alone. At a median follow up of 47 months, there were no significant differences in median overall survival between the two treatment arms: 45 and 43 months in the EBRT + ADT and ADT arms, respectively (HR: 0.90, 95% CI: 0.70-1.14, p=0.4). However, subgroup analysis by number of metastatic lesions suggested a potential overall survival benefit for radiotherapy in patients with <5 metastatic sites (HR: 0.68, 95% CI: 0.42-1.10).6
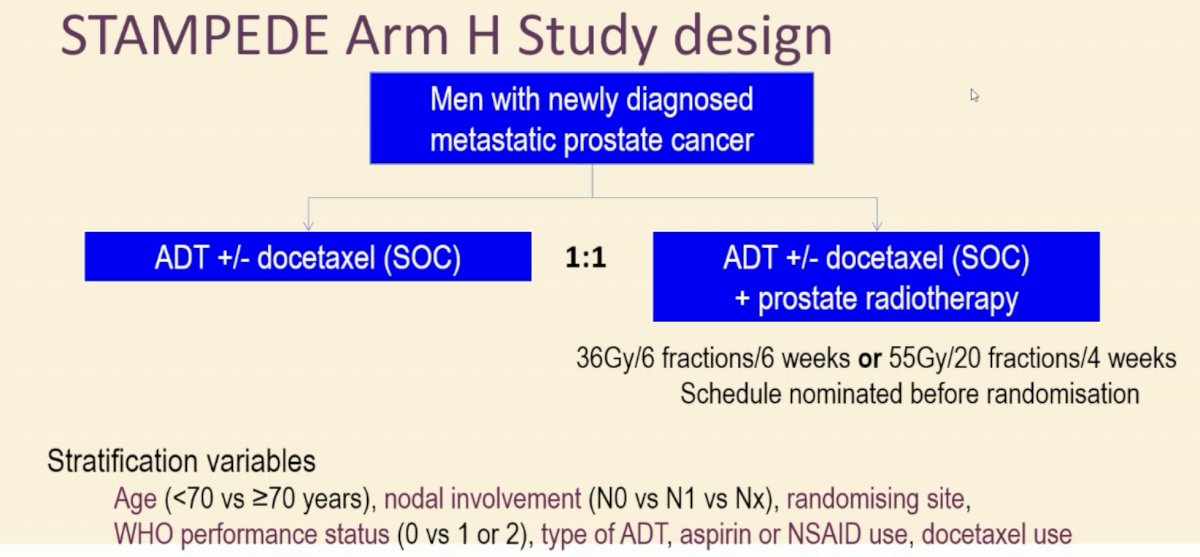
STAMPEDE (Arm H) was an open label, randomized controlled phase III trial of 2,061 men from 117 hospitals across Switzerland and the UK. This arm randomized patients with de novo mHSPC in a 1:1 fashion to standard of care plus radiotherapy versus standard of care alone between January 2013 and September 2016. Standard of care was lifelong ADT with upfront docetaxel permitted from December 2015. Men allocated to radiotherapy received either a daily (55 Gy in 20 fractions over 4 weeks) or weekly (36 Gy in six fractions over 6 weeks) schedule that was nominated before randomization.
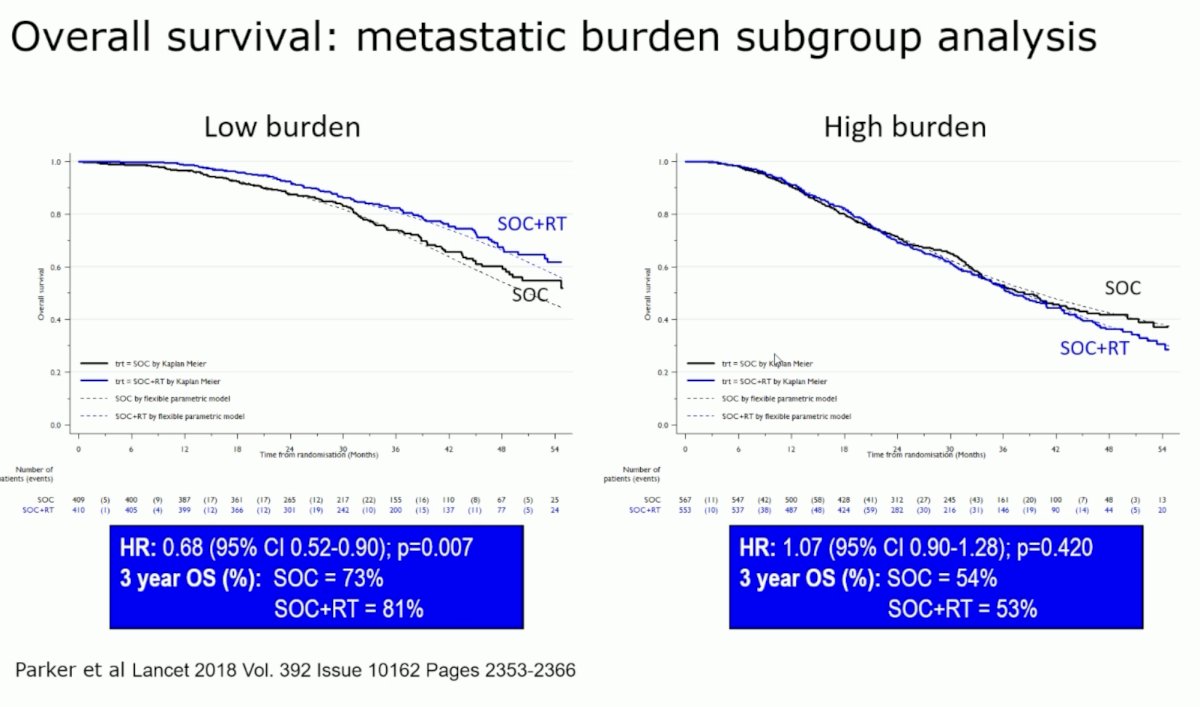
In the overall cohort, radiotherapy improved failure-free survival (HR: 0.76, 95% CI: 0.68–0.84) but not overall survival (HR: 0.92, 95% CI: 0.80–1.06). However, when stratified by metastatic burden, overall survival benefits were seen in the CHAARTED low volume group (HR: 0.68, 95% CI: 0.52-0.90) with restricted mean survival time improved by 3.6 months from 45.4 to 49.1.7 Updated results of this trial were published in 2022. With a median follow up of 61.3 months, prostate radiotherapy continued to demonstrate overall survival benefits in patients with low metastatic burden (HR: 0.64, 95% CI: 0.52-0.79).8
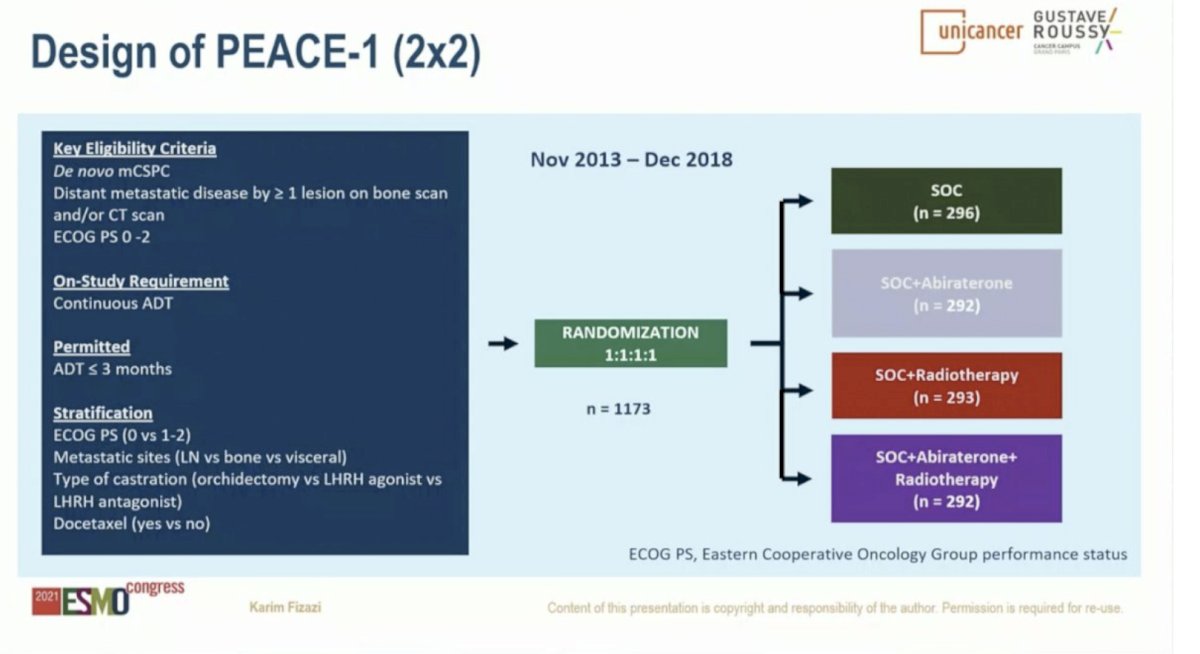
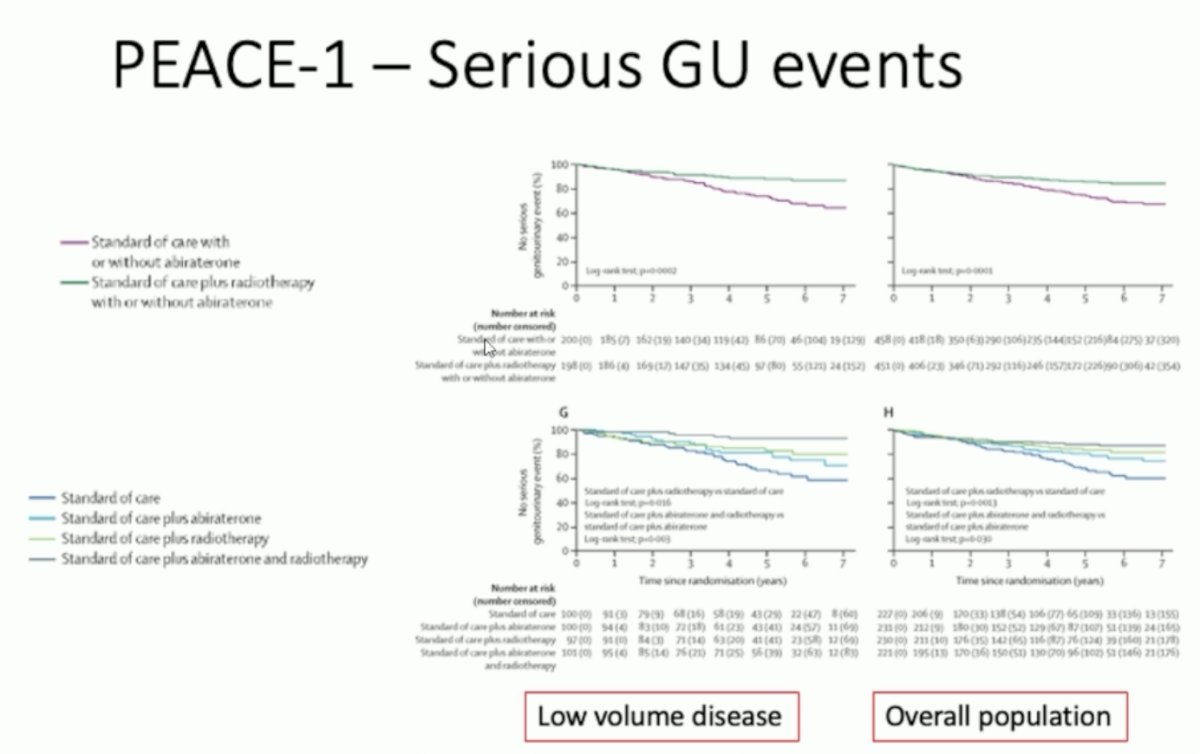
In addition to potential survival benefits, the PEACE-1 trial demonstrated that the addition of prostate radiotherapy to standard of care +/- abiraterone was associated with significant improvements in the time to serious genitourinary events in both the low volume and overall cohorts.9
Dr. Clarke concluded as follows with regard to radiotherapy in low volume M1 and M0 patients:
- There is good evidence to treat the primary in low volume M1 HSPC
- There is good evidence for combining radiotherapy, abiraterone + ADT in high risk M0 disease
- Docetaxel’s effects in M0 disease less pronounced than abiraterone
- As many high risk M0 will be low volume M1 on PSMA PET, this suggests that we may need to re-look the need for long-term ADT in all cases, given how good the M0 outcomes are
Presented by: Noel Clarke, MBBS, FRCS, ChM, Professor of Urological Oncology, Salford Royal Hospital & The Christie NHS Foundation Trust, Manchester, UK
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Widmark A, Klepp O, Solberg A, et al. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7/SFUO-3): an open randomised phase III trial. Lancet. 2009; 373(9660): 301-8.
- Warde P, Mason M, Ding K, et al. Combined androgen deprivation therapy and radiation therapy for locally advanced prostate cancer: a randomised, phase 3 trial. Lancet. 2011; 378(9809): 2104-11.
- Kishan AU, Sun Y, Hartman H, et al. Androgen deprivation therapy use and duration with definitive radiotherapy for localised prostate cancer: an individual patient data meta-analysis. Lancet Oncol. 2022; 23(2): 304-16.
- El-Taji O, Taktak S, Jones C, et al. Cardiovascular Events and Androgen Receptor Signaling Inhibitors in Advanced Prostate Cancer: A Systematic Review and Meta-Analysis. JAMA Oncol. 2024; 10(7): 874-84.
- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022; 399(10323): 447-60.
- Boeve LMS, Hulshof MCCM, Vis AN, et al. Effect on Survival of Androgen Deprivation Therapy Alone Compared to Androgen Deprivation Therapy Combined with Concurrent Radiation Therapy to the Prostate in Patients with Primary Bone Metastatic Prostate Cancer in a Prospective Randomised Clinical Trial: Data from the HORRAD Trial. Eur Urol. 2019; 75(3): 410-418.
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet. 2018; 392(10162): 2353-66.
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the prostate for men with metastatic prostate cancer in the UK and Switzerland: Long-term results from the STAMPEDE randomised controlled trial. PLoS Medicine. 2022; 19(6): e1003998.
- Bossi A, Foulon S, Maldonado X, et al. Efficacy and safety of prostate radiotherapy in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2024; 404(10467): 2065-76.